
Abstract

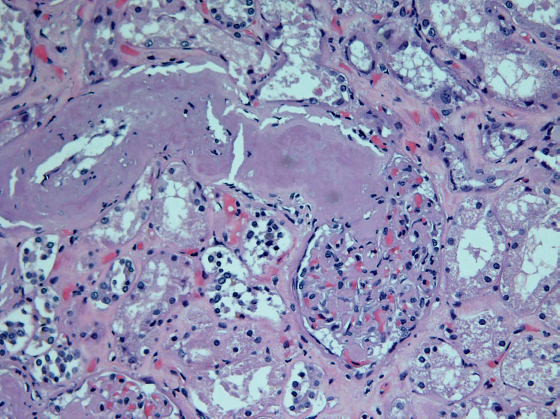
Photomicrograph of the kidney showing marked expansion of the arteriolar wall and juxtaglomerular apparatus. Hematoxylin and eosin (H & E, x200).
Amyloid is an insoluble amorphous, eosinophilic proteinaceous deposit that may deposit locally within any organ or tissue type or may present as a systemic disease (systemic amyloidosis). More than 25 different types of proteins are known to form amyloid fibrils with classification based on the amyloid fibril protein type (1, 2). Accurate diagnosis and classification is essential for proper management.
In amyloid light chain (AL) amyloidosis, also known as primary amyloidosis, the precursor protein is a clonal immunoglobulin light chain or light chain fragment and is associated with various B-cell lymphoproliferative disorders. In the United States and the Western world, AL amyloidosis is the most prevalent type of systemic amyloidosis. In amyloid associated (AA) or secondary amyloidosis, the precursor protein is serum amyloid A, and is associated with chronic inflam-matory processes. AA amyloidosis accounts for an estimated 45% of all systemic amyloidosis worldwide (3).
Clinically, the presentation and symptoms depend on the distribution pattern and amount of amyloid deposited. Organ dysfunction results from disruption of tissue architecture and likely direct cytotoxic effects from amyloidogenic precursor proteins (4). Of the organs involved, renal abnormalities are the most frequent, presenting as nephrotic syndrome with advanced renal failure and enlarged kidneys (1, 2). However, cardiac involvement often determines the patient's prognosis with mortality in more than half of all cases (4). Serious complications include restrictive cardiomyopathy, arrhythmias, conduction disturbances and eventual fibrosis (5).
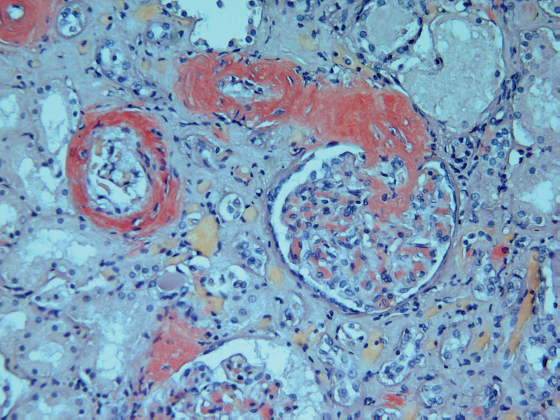
Similar microscopie findings, highlighted by Congo Red stain, x200.
This example of systemic amyloidosis is from a 64 year-old white male with past medical history significant for hypertension, pulmonary hypertension, myocardial infarct, prior cardiac cathe-terization, recent vertigo and sudden loss of consciousness. He was found unresponsive in a ditch in front of his residence. At autopsy, the heart was enlarged with concentric left ventricular hypertrophy, and weighed 720 grams. Microscopic sections of the heart, liver, and spleen demon-strated intraparenchymal vessels with thickened walls containing homogenous eosinophilic material and increased perivascular fibrosis. The kidney demonstrated similar deposits of the afferent and efferent arterioles, juxtaglomerular apparatus, and glomerular basement membrane. Congo Red stains showed characteristic salmon-colored deposits of amyloid within the vascular wall, and polarization demonstrated “apple-green” birefringence.
Footnotes
The authors, reviewers, editors and publication staff do not report any relevant conflicts of interest.