
Abstract
Truncus arteriosus is a rare congenital heart defect characterized by a single common arterial trunk giving rise to both the pulmonary and systemic arteries. Concurrent cardiac abnormalities are common. In the absence of surgical intervention, the condition is associated with extremely high infant mortality, with the mechanism of death being either arrhythmia or congestive heart failure. We report the case of a previously healthy and reportedly normal two-week-old infant who was found dead in his crib. At autopsy he was found to have truncus arteriosus communis persistens, a rare subtype of truncus arteriosus with associated valve atresia and left ventricular hypoplasia. This case highlights that forensic pathologists may encounter severe cardiac malformations in previously normal infants, and the necessity for thorough evaluation and accurate diagnoses.
INTRODUCTION
Truncus arteriosus (TA) is a congenital heart anomaly characterized by a single common arterial trunk arising from the base of the heart and giving rise to the pulmonary, coronary, and systemic arteries. This arterial trunk frequently originates primarily or entirely from the right ventricle (1, 2) and is frequently accompanied by right-side heart defects (3). Right-sided hypertrophy of both the atrium and ventricle is common (1). A variety of specific cardiac malformations can be found in association with TA including atresia of the tricuspid valve, coronary ostial stenosis, abnormal coronary artery origin, and right-sided aortic arch, among others (1, 3, 4).
In this report, we describe an infant with a single (truncal) artery arising entirely from the right ventricle, with accompanying mitral valve atresia and severe left ventricular hypoplasia. This particular constellation of anatomic anomalies in the context of TA is extremely rare, with only a few cases having been reported in the literature (1–3, 5–7).
CASE REPORT
A previously healthy two-week-old white male term infant was found supine and unresponsive in his crib. There was no evidence to suggest an unsafe sleep environment. Emergency Medical Services responded to the residence and commenced resuscitative efforts. He was declared dead shortly following admission to the Emergency Department of a local hospital. His history was significant only for uneventful circumcision two days prior to death; his parents noted that he had ‘not been breathing right’ since the circumcision.
An autopsy performed the day after death showed a small for developmental age male infant with a weight for age that was of the 25th percentile, weight for length of the 10th percentile, and head circumference that was of the 10th percentile. Although he had undergone a circumcision in the days immediately preceding death, no infectious or inflammatory complications of the surgical procedure were observed. External evidence of malformations or injuries was absent. A skeletal survey did not demonstrate features of acute or remote osseous injuries or primary skeletal pathology.
Layered soft tissue examination of the chest and abdominal walls did not reveal injuries. Removal of the chest plate demonstrated profound enlargement of the barrel-shaped heart. The right lung was tetralobar, and the left lung was trilobar. No other malformations or pathologic changes were detected macroscopically at the time of autopsy.
The heart and lungs were perfused with formalin in situ, and removed for later en bloc examination. Detailed studies of the heart-lung block demonstrated severe cardiomegaly (75 grams [expected weight 19 grams]) with marked dilation of the right atrium, a comparatively smaller left atrium, and a prominently left-laterally displaced interventricular groove (

The heart and lungs were perfused with formalin in situ, and fixed prior to evaluation. After examination of the pulmonary arterial and venous systems, the lungs were removed from the heart. The enlarged right atrium and ventricle, single arterial trunk, small left atrium, left-laterally displaced interventricular groove and small left ventricle are obvious. Internal anatomic features were site-appropriate.

Illustration outlining the major malformations identified in the formalin-perfused heart specimen including a single arterial trunk originating from the hypertrophic and spongy right ventricle, right atrial enlargement, a secundum-type atrial septal defect, and a severely hypoplastic left atrium and ventricle.
The interatrial septum had a 6 millimeter diameter secundum-type defect. The small left atrium was found to be in association with mitral atresia. The left ventricular chamber was severely hypoplastic at only 2 millimeters diameter. No obvious connections were between the left ventricle and the right side of the heart (the interventricular septum was intact).
Histologic evaluation of the heart did not reveal features of ischemia, infarction or inflammation. The thickened right ventricular wall had endocardium-lined spaces that extended to the inner third of the myocardium; the ratio of right ventricular compact to non-compact myocardium was approximately 1:5 (
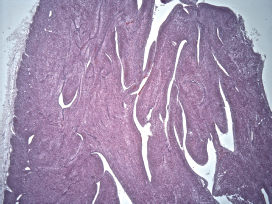
Section of right ventricular free wall stained with hematoxylin and eosin (H&E) and photographed through a 2X objective. The hypertrabeculated or non-compacted ('spongy') nature of the wall is obvious. Endothelium-lined spaces extend deeply into the myocardium.
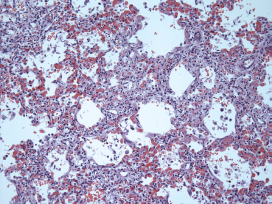
Section of lung stained with hematoxylin and eosin (H&E) and photographed through a 20X objective. The septal capillaries are engorged and dilated (pulmonary hemangiomatosis).
Toxicology testing did not reveal alcohols, acetone or illicit drugs. Microbiological cultures of the blood was negative. Metabolic screening tests were negative.
Based on the totality of available information and the constellation of cardiac pathology, the decedent was diagnosed with truncus arteriosus communis persistens.
DISCUSSION
Definition and Pathophysiology
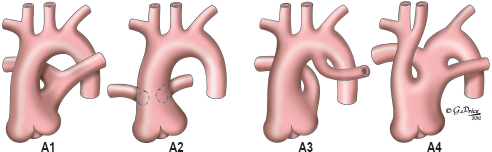
Persistent TA is a rare congenital heart anomaly characterized by the presence of a single common arterial trunk originating from the base of the heart and giving rise to the coronary, pulmonary and systemic arteries. The anatomical configuration of the coronary, pulmonary, and aortic branches is somewhat variable, but generally the pulmonary trunk emerges distal to one or more coronary arteries and proximal to the first branch of the aortic arch (4). Many attempts have been made to effectively classify TA on the basis of anatomical variations (
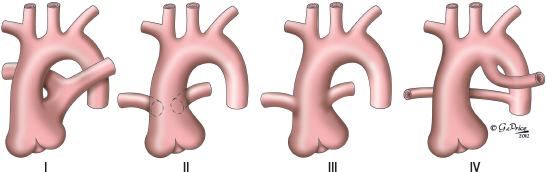
Truncus arteriosus is characterized by a single arterial vessel arising from the heart base, giving rise to systemic, pulmonic and coronary arterial systems. Different systems of classification have evolved over the years including that by Collette and Edwards (8). Their system, which recognized four subtypes, is illustrated here. In Type I, the pulmonary arteries originate with a short pulmonary trunk. Types II and III both have the pulmonary arteries coming directly from the truncus; they are differentiated by how close to one another each pulmonary artery is at its point of origin (close together - Type II; further apart - Type III). Type IV is no longer considered to be a form of truncus arteriosus, but rather a form of pulmonary atresia. It is shown here only for historical reference.
Since the 1970's, successful surgical correction of TA has been possible. In the absence of surgical management in early infancy, TA results in approximately 90% mortality by the age of one year (11) with the underlying mechanism of death being either congestive heart failure or arrhythmia.
Only a select few cases have been described in which TA is accompanied by mitral atresia and severe left ventricular hypoplasia. Secundum-type atrial septal defect has been well-described in the literature in association with TA (12), and has been observed in the rare cases of TA with associated mitral atresia combined with severe left ventricular hypoplasia (3). Similarly, the tricuspid morphology of the truncal valve, as was observed in this case, has been reported to be the most common valve morphology, although it has been described along the morphologic spectrum from bicuspid to pentacuspid (1, 4, 12). It should also be noted that the absence of a ventricular septal defect is highly unusual (13).
Molecular Etiology
Truncus arteriosus arises during development from the complete or partial failure of the septum that divides the embryonic pulmonary and aortic arterial trunks (4). Although the precise genetic etiology of TA has yet to be fully determined, considerable progress has been made in understanding the molecular origins of this condition. In the mid-1980's, developmental studies using experimental animal models established that cardiac neural crest cells were responsible for orchestrating outflow septation under normal developmental conditions, and that selective ablation of the cardiac neural crest generated the truncus arteriosus phenotype in multiple experimental animal models (14).
Under normal developmental conditions, a variety of highly regulated signaling pathways direct the migration, survival, and differentiation of cardiac neural crest cells. In particular, the Wnt signal transduction pathway has been shown to play a crucial role in cardiac development. Mutants of key Wnt signal transduction pathway members such as murine gene disheveled 2 (Dvl2) have been shown to generate the TA phenotype (15). Similarly, homozygous mutants for the paired box transcription factor Pax3, which is important for targeted migration of neural crest cells, develop severe, embryonic lethal TA, amongst other defects (16). Lastly, Semaphorin 3C, a secreted ligand that is instrumental in axonal guidance in the central nervous system, has been shown to be crucial in guiding the migration of cardiac neural crest cells during development of the outflow tract. Semarphorin 3C-null mice develop a phenotype of TA (17).
Truncus arteriosus is often associated with the chromosomal microdeletion in the 22q11.2 band, a region which is etiologically linked to a variety of congenital heart defects (the 22q11.2 deletion syndrome) and which is believed to have an effect on the dysregulation of neural crest cells during development (18, 19).
Prevalence
Truncus arteriosus is very rare, with a frequency ranging from 0.03 (11) to 0.056 (20) per 1000 live births in the United States. Recent estimates suggest that TA accounts for only 1.2% of all live birth congenital heart defects, with a male to female ratio of 1:1 (4).
CONCLUSION
This young infant died suddenly and unexpectedly of a rare and severe form of congenital heart disease. Forensic pathologists tasked with the responsibility of performing autopsies on infants must be aware of the broad spectrum of congenital heart disease that may present at autopsy, and the detailed fashion in which the cardiovascular system must be assessed in sudden infant deaths. The necessity for accurate diagnosis extends far beyond the medical examiner's statutory duty to correctly determine cause and manner of death, and into the responsibility to alert family members of any possibility of hereditofamilial disease. While uncommon, TA is an important finding because of its association with 22q11.2 deletion syndrome - an autosomally dominant inherited disease.
Footnotes
ACKNOWLEDGEMENT
Artwork prepared under contract with Professional Illustrator Gemma Price.
Dr. Matshes is the Director of Operations for Academic Forensic Pathology. The authors, reviewers, editors, and publication staff do not report any other relevant conflicts of interest.