
Abstract
Introduction
Medical examiners/coroners serve various functions beyond the medicolegal framework, including making contributions to public safety and health. In order to effectively fulfill this role, it is essential to ensure accurate certification of each death.
Materials and Methods
In Vermont, the Department of Health, Vital Records Division has developed a death certificate surveillance program in which all registered deaths are reviewed by the Office of the Chief Medical Examiner (OCME). A death certificate is fagged by the OCME for further investigation when cause and manner of death statements are incomplete, erroneous, or suggest the possibility of an unnatural death. If necessary, after review, death certificates are amended. Death Certificate Review (DCR) cases between 2008 and 2011 were retrieved from the OCME database. Data were evaluated for amendments of cause and manner of death.
Results
The OCME reviewed all death certificates and further investigated 4.4% and amended 3.3% of all death certificates in Vermont between the years 2008–2011. Eighty-eight percent of the amended DCRs were for cause of death statements and 10% resulted in change of manner. For the latter, change from natural to accident was most frequent.
Conclusions
Death certificates are a major source of epidemiologic data. Ensuring complete and accurate death certification through death certificate surveillance is a small but significant contribution of the OCME to public health.
Keywords
Introduction
Primarily, the role of medical examiners/coroners is to determine cause and manner of death, collect evidence, and lend expertise in forensic medicine for criminal cases involving unnatural, wrongful deaths. Over the years, this role has expanded and evolved to serve various functions beyond the medicolegal framework. These include making contributions to public safety, public health, and the medical community by collecting and cataloging epidemiologic data and supporting programs and initiatives that reduce morbidity and mortality (1–4). To effectively fulfill this role, it is essential to collect pertinent information and ensure accurate certification of each death. Identifying errors and developing solutions to improve the accuracy of data has thereby become a critical component in death investigation.
Every death is certified by a medical practitioner or medical examiner/coroner and documented in the form of a death certificate. Important data are collected via the death certificate, most notably cause and manner of death, along with significant contributory factors. This legal document has multiple applications. Not only does it provide families a sense of closure, it is often required for many end-of-life legal matters such as life insurance policies and banking/estate management. Moreover, the information required and gathered on a death certificate is compiled into state, regional and national databases from which morbidity and mortality statistics are generated. Data are then used for surveillance of health and illness, identifying hazards to safety and trends in injury/illness and proper allocation of resources to prevent injury/illness, and promote public welfare (2, 5–7). As such, the accuracy of data analyses rely heavily on cause of death and manner of death statements recorded on death certificates. Thus, the importance of accurate documentation and amendments of erroneous death certificates cannot be overstated.
The Vermont Office of Chief Medical Examiner (OCME), established in 1953, is a section of the Division of Health Surveillance of the Vermont Department of Health. Other sections under this division include Vital Records and Epidemiology. The Vermont OCME is a statewide medical examiner system, serving a population of approximately 620,000. With assistance from the Vermont OCME, the Vermont Department of Health Vital Records has developed a death certificate surveillance program in which all Vermont death certificates are reviewed by the OCME. Incorporated into the daily work flow of the OCME, death certificates are reviewed by forensic pathologists or certified medicolegal death investigators and fagged for further investigation when cause and manner of death statements are incomplete, erroneous, or suggest the possibility of an unnatural death. After investigation, death certificates are amended by the OCME when necessary. This study aimed to examine the frequency of errors and amendments to the cause and manner of death statements in the state of Vermont between the years 2008 to 2011.
Materials and Methods
In the years 2008–2011, there were 20,781 death certifications in the state of Vermont, all of which were reviewed by the OCME. Of these, 915 (4.4%) cases were identified as requiring additional investigation. These cases were given an OCME case number and a designated case type of “Death Certificate Review” in the OCME database. By definition, none of these were formally reported to the OCME by an outside agency or person and none were originally certified by the OCME. DCR cases were retrieved from the OCME database (Justice Trax LIMS Plus) and data were sorted and tabulated using Crystal Reports and Microsoft Excel. Analyzed data included the certified and amended cause of death (COD), contributory cause of death (CCOD) and manner of death (MOD), as well as comments included in the “how injury occurred” box of each death certificate. Types of amendments were tabulated. Natural deaths in 2011 which required amendment of only the cause of death (i.e., manner remained natural) were reviewed in more detail and classified according to the following four categories: Major change in COD statement; Underlying etiology added to COD; Change to CCOD only; and Removal of nonsense/narrative or correction of major typographical errors.
Results
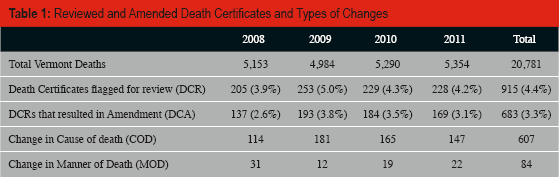
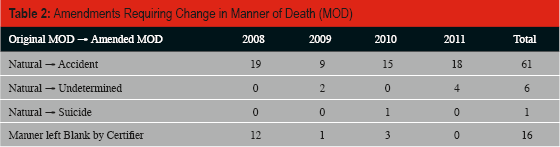
Over twenty thousand death certificates were reviewed by the OCME during the years 2008 through 2011. The OCME performed further investigation into 4.4% (915) and amended 3.3% (683) of these death certificates. Eighty-seven point eight percent (607) of the amendments were for cause of death statements and 12.2% (84) resulted in a change of manner (Table 1), these categories not being mutually exclusive. Of the 84 manner of death errors, 68 natural deaths were amended to an unnatural manner (Table 2). The most frequent MOD change was from natural to accident, followed by natural to undetermined. Erroneous certification of fall-related injuries in the elderly (e.g., pelvic or femur fractures and subdural hemorrhages) as natural manners of death was a recurring problem. Blunt trauma from motor vehicle collisions, choking on food, and hypothermia from exposure were also erroneously certified as natural. MOD errors also included 16 certificates where manner was left blank; after investigation, fourteen were determined to be natural, one undetermined, and one accidental.
Reviewed and Amended Death Certificates and Types of Changes
Amendments Requiring Change in Manner of Death (MOD)
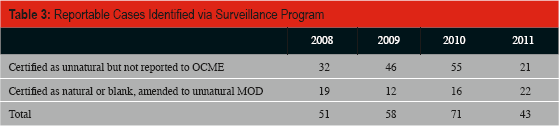
There were 223 unnatural deaths (1% of all deaths) that should have been reported to the OCME, as defined by statute, but were not (Table 3). These deaths were either originally certified as unnatural but not reported to the OCME, or erroneously certified (as natural or left blank) and had to be changed to unnatural MOD (Table 3). These cases represent deaths which would have been missed were it not for the surveillance system.
Reportable Cases Identified via Surveillance Program
A detailed review of natural deaths in 2011 that required a change in COD or CCOD only (i.e., no MOD change), showed that lack of a sufficient underlying etiology was the most common error (93 of 131). Common examples include: “pneumonia” being changed to “bronchopneumonia due to Alzheimer's disease”, “congestive heart failure” being changed to “congestive heart failure due to hypertensive and atherosclerotic cardiovascular disease”, and “intracranial hemorrhage” being changed to “intracerebral hemorrhage due to hypertensive cardiovascular disease.” Five of 131 had a major change in the COD that entirely altered the substance of the statement.
Discussion
There are two major parts of the death certificate that relate to the cause of death. Part I includes the immediate, intermediate and underlying etiology of death. As defined, the immediate COD is the disease or complication that occurred closest to the time of death and the underlying COD is the disease or injury that initiated the train of events leading directly to death. Part II captures diseases or conditions that contributed to death though did not result in the underlying cause. Historically, there were four classes under manner of death: Natural, Accident, Suicide and Homicide. Over the years, another class, Undetermined, has become widely used in circumstances in which a definitive manner of death cannot be determined. Some jurisdictions have elected to add therapeutic complication as another manner of death (8). Of note, the Vermont OCME uses Undetermined manner of death and specifies therapeutic complication in the “how injury occurred” section in applicable circumstances.
In an effort to standardize death certificates to ensure proper collection of pertinent information and data, National Center for Health Statistics (NCHS) within the Center for Disease Control (CDC) has issued a standard death certificate format which most states have adopted with minor variations (6). To aid physicians and other practitioners in compliance and proper documentation, the CDC, along with the College of American Pathologists (CAP), has published handbooks and guidelines.
In spite of these efforts, errors in death certification remain common. Many previous studies at academic institutions and medical examiners'/coroners’ offices have looked at death certificate errors, reporting a wide spectrum ranging from minor, albeit nontrivial, errors such as spelling and demographic errors, illegible handwriting and the use of abbreviations, to major errors such as insufficient, absent, or incorrect underlying etiologies of cause and manner of death (9–18). Approaches and interventions to minimize errors and subsequent amendments have been implemented with variable results. However, the variability of settings in which these studies are performed precludes accurate synthesis of their results. That is, studies assessing death certificate errors in the hospital setting typically assess accuracy by comparing death certificates that are certified by clinicians to those certified by pathologists after postmortem examination or via the use of mock death certificates in training program settings. In this setting, studies report major error rates ranging from 24–45% (9–12). In contrast, studies done in the medical examiner/coroner office setting involve assessment of amendment rates due to additional toxicology or investigatory results report amendment rates ranging from 1–4% (16–18). Moreover, these studies are limited by the types of deaths included; hospital studies are, for the most part, limited to natural deaths, and thus cannot properly assess errors regarding manner of death. Conversely, in medical examiner/coroner studies, unnatural deaths are overrepresented.
Furthermore, death investigation systems as well as administrative authority to amend death certificates vary across the nation. Systems are established at state, region or county levels, with cases falling into different jurisdictions accordingly. There are over two thousand death investigation jurisdictions within the country. As of 2010, only 25 states have a statewide medical examiner system. Vermont is one of few states in which the medical examiner system is not only statewide but is also administratively within the state's health department with full authority to modify death certificates. Our study is therefore unique in that it encompasses all deaths within a state, regardless of the institutional affiliation or training level of the certifier, and includes all manners of death. That is, all registered deaths filter through one central location from which our data has been generated.
The death certificate surveillance program in our state was established by the OCME to identify and correct errors in cause and manner of death; demographic errors are corrected by the funeral directors. The primary objective is to identify unnatural deaths that were not reported to and certified by the OCME in accordance with statute. Review of amended cases in 2011 indicates an overwhelming majority of errors to be due to missing underlying etiology, followed by changes in contributory causes. Common examples are listing only pneumonia, sepsis, or heart failure with no explanation of the underlying etiology. Of note, many previous studies have included illogical sequence into their error rate. However, it has been our practice to prioritize the presence and accuracy of an underlying etiology while tolerating some problems among listed mechanisms. Illogical sequences of events that are medically improbable but that do not change the substance of the statement were not tabulated or corrected. Inclusion of such cases would likely have resulted in much higher numbers of amendments.
Ten percent of amendments were due to manner of death errors. Seventy cases (7.6% of DCR cases; 0.3% of all deaths) were changed from natural to unnatural: 62 to accident, seven to undetermined and one to suicide. Regardless of system setup and jurisdiction, medical examiners/coroners examine both natural and unnatural deaths. That is, after thorough investigation and examination, the deaths are classified in their respective manners. However, this method relies heavily on unnatural or questionable deaths being reported to the medical examiner/coroner offices. In most systems, deaths that are documented as natural manner do not get attention from the medical examiner/coroner office. The death certificate review and surveillance program in Vermont allows for these would-be-missed cases to be further investigated and properly documented. In our study, we identified 223 reportable cases (1% of all deaths; average of 55 per year) of which the OCME would not have been aware, were it not for this surveillance system. Not only does an unreported, incorrectly certified death create confusion for the family, there are significant implications for health statistics.
Our study spans four years, therefore it is important to note changes made during this period that may have affected our data. The Vermont OCME has been routinely reviewing and correcting every Vermont death certificate for over a decade, previously through a paper process. In late 2009, an electronic death registration system (EDRS) was initiated statewide with most, but not all, certifiers enrolled by mid-2010. This on-line system greatly facilitated the OCME review process and effectively eliminated many minor errors such as abbreviations, typographical errors, omitted patient information, and areas left incomplete/blank (not tabulated in this study). The electronic system has several types of prompts that improve the quality of certification and increase the likelihood of unnatural deaths being reported to the OCME. A certifier is notified of his/her error and prompted for correction when only mechanisms without underlying etiology are entered in COD statements of Part I (e.g., “chronic renal failure” without the underlying etiology of diabetes mellitus). This provides instant education and feedback. Similarly, when nonspecific etiologies are used, the certifier is asked to provide additional/specific information such as clarifying “cancer” with “small cell lung carcinoma”. The software also identifies key words that may suggest an unnatural etiology, such as fracture, trauma, injury, and poisoning. When such words are recognized in either Part I or II, a message is displayed indicating that the term suggests a reportable death and the medical examiner's phone number is provided. These can be certified “with exception,” meaning that the certifier acknowledges the prompt but is choosing to override it. This override generates an internal fag which can be tracked by vital records. A message prompting the certifier to contact the OCME is also displayed when a non-medical examiner selects any MOD other than natural. Only authorized users of the OCME and Vital Records are able to complete an unnatural certificate. In theory, this should force all unnatural deaths to be reported to the OCME. Unfortunately, Vital Records continues to receive a very small number of paper death certificates that are manually entered.
The prompts and rules built in to EDRS were designed to improve death certification. Since the number of certifiers using the electronic system has increased over the study period, the extent of major errors should theoretically have decreased. Our numbers are sufficiently small that the effect of EDRS on certification quality is not readily apparent.
A detailed review of the DCRs done in 2011 (229 cases) showed that 59% of these cases required only medical record review/phone investigations done from our office by our full-time, medicolegal death investigator (most often) or by the forensic pathologists. Investigation of DCR cases and daily surveillance of the EDRS comprises approximately 30% of a death investigator full-time equivalent. The remainder of the 2011 DCRs (41%) were investigated by our field medicolegal death investigators, who are paid on a fee-for-service basis. In 2011, 5% of DCRs required a full investigation including examination of the body (typically done at the funeral home). Generally, the forensic pathologists need only review the investigator reports and issue death certificate amendments, though some cases require that the pathologist speak directly with the certifying physician. Once the initial burden of setting up such a system is complete, we estimate an average of 2.7 person hours per death certificate review to perform the surveillance, investigation and corrections. Our jurisdiction performs approximately 44 reviews per 1000 deaths.
In conclusion, errors in cause and manner of death certification are common and worth correcting. While the majority of errors relate to incorrect or absent underlying etiologies, incorrect certification of manner does occur and is of significant consequence to families, law enforcement, and the legal system. Electronic death registration systems are a relatively new change to this old process. Implementation of such a system in our jurisdiction has facilitated timely, efficient surveillance of certificates, contributed to the education of certifiers, and eliminated some, though not all, errors. More cases are being reported to the OCME due to the prompts. Future studies will be needed to determine the full impact of EDRS and to identify persisting errors that can be targeted when educating certifiers.
Footnotes
This work was presented at the 2012 Annual Meeting of the National Association of Medical Examiners. Dr. Tatsumi won the Susan P. Baker Public Health Impact Award for this work. The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest.