
Abstract
Advances in radiologic imaging are being applied to the study of wound ballistics. Each of the modalities used (fluoroscopy, radiography, computed tomography, and magnetic resonance imaging) has strengths and limitations. Cross sectional digital based modalities have advantages over traditional radiography and fluoroscopy for localization and recovery of projectiles and documentation of wound tracks. Data from multiplanar two-dimensional and three-dimensional imaging can best be used by the forensic pathologist when combined with pathologic findings. With this information it may be possible to enhance the current understanding of wound ballistics.
Introduction
Ballistics is the study of the dynamics of projectiles. When applied to firearms, it is further categorized into interior ballistics, exterior ballistics, and terminal ballistics. Interior ballistics is the study of the bullet within the firearm. For firearms that use a cartridge, this covers the time period from when the firing mechanism strikes the primer to when the bullet exits the barrel. Exterior ballistics is the study of the bullet in flight and covers the time period from when the bullet exits the barrel to when the bullet impacts a target. The target may be paper, wood, animal, human or the ground. Terminal ballistics is the study of the interaction between the bullet and the target.
Although the three ballistic categories are separated from one another based on the location of the bullet, they are interrelated by the laws of physics. However, this interrelation can be complex. In order to understand terminal ballistics, it is necessary to have at least a cursory understanding of interior ballistics, exterior ballistics, and bullet types. In-depth discussion of these topics can be found in Di Maio's book entitled “Gunshot Wounds: Practical Aspects of Firearms, Ballistics, and Forensic Techniques“ (1) and Rinker's book entitled “Understanding Firearm Ballistics: Basic to Advanced Ballistics, Simplified, Illustrated and Explained“ (2). Varying only a single factor such as bullet type (e.g., full metal jacket versus hollow point) may have a significant effect on how the bullet interacts with the target.
Wound ballistics is a subset of terminal ballistics that refers to the study of the dynamics of a bullet within biological tissue and the injuries caused. It is generally accepted that the first scientific investigations of wound ballistics were performed by the Swiss surgeon Emile Theodor Kocher in the 1870s. At the time of these studies, the “explosive” injuries made by conoidal bullets were thought to be due to the bullet's rotation, imparted by the barrel's rifling, which caused centrifugal forces that tore tissue apart. Kocher was able to show that there was no difference between wounds caused by conoidal bullets fired from a barrel with rifling and those from a barrel without rifling. He proposed that these “explosive” injuries were caused by hydrodynamic factors that came to be known as cavitation. In addition, he noted the importance of both bullet deformation and bullet velocity on determining the degree of wounding (3, 4). In England in 1898, Charles Woodruff proposed that it is the transfer of the kinetic energy from the bullet to the tissue and not just the bullet's amount of energy at entry that determines the degree of wounding (5).
Since that time, there have been numerous wound ballistics studies. These include, but are not limited to, studies by LaGarde and Thompson (6), Hatcher (7), Harvey (8), Fackler (9, 10), MacPherson (11), and Sellier (12) and the writings of Di Maio (1) and Bellamy and Zajtchuk (13). These studies have shown that wound ballistics depends on many factors, some controllable and some uncontrollable. Some of these factors include: type of firearm, construction of the cartridge, type of gunpowder, construction of the bullet, flight path of the bullet, intermediary target, angle of impact, location of impact on the body, deformation and fragmentation of the bullet after impact, “tumbling” of the bullet within the body, viscoelastic properties of the tissues, and nature of the permanent and temporary cavities. The permanent cavity is the actual track of tissue crushed by the bullet, including fragments. The temporary cavity is the displacement of tissue around a bullet's track that expands and collapses in milliseconds.
Although there is little controversy that the permanent cavity causes wounding, there is some controversy to the degree of wounding that the temporary cavity causes. For example, fracture of long bones in the extremities not hit by the bullet are mentioned in the literature but are rarely seen clinically (14, 15). Another area of controversy is the possible wounding caused by the sonic shock wave that precedes the bullet as it passes through tissue (11, 16). Information gathered from the traditional forensic autopsy has not been able to either support or reject most of the hypotheses. However, incorporating recent advances in radiologic imaging may lead to relevant information.
Radiologic Imaging
Since the development of the radiograph by Wilhelm Roentgen in 1895, radiologic imaging has been used in medicolegal death investigations (17). In terms of wound ballistics, these images have been used to document the presence and location of projectiles and the injuries caused by them. The National Association of Medical Examiners (NAME) has established minimum standards for the use of radiologic imaging in forensic autopsy performance. The second of the three standards states “Radiographs detect and locate foreign bodies and projectiles“ (18). However, this guideline does not delineate either the extent of imaging required or the imaging modality.
There are four radiologic imaging modalities currently being used in medicolegal death investigations involving ballistic wounds: fluoroscopy, radiography, computed tomography (CT), and magnetic resonance imaging (MRI). All modalities are now available in digital format allowing for electronic recording, viewing, manipulation, and transmission of images. Each modality has its own unique advantages and disadvantages for investigating wound ballistics postmortem. A fifth modality, sonography, can be considered. There are limitations to this modality, mainly soft tissue air that degrades the images, and consequently experience has been limited.
Fluoroscopy displays a continuous X-ray image on a monitor in real-time. The commonly used configuration by medicolegal systems is the “C-arm” unit where X-ray source and receptor are linked and the object studied is placed in between. The main use of the fluoroscope is to facilitate the localization and recovery of projectiles. When viewing the images real-time, as the body or fluoroscope is moved, the field of view is limited and motion obscures detail. The scanning technique may allow one to “miss” a bullet or bullet fragments. The fluoroscope only displays where the projectile is in two dimensions (
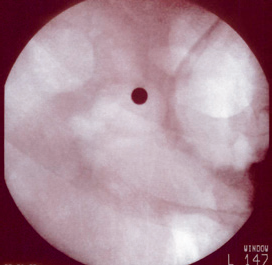
Fluoroscopic (“C-arm”) image of a round projectile showing excellent edge detail.
Radiography uses electromagnetic radiation, “X-rays”, to generate and record a static image after termination of exposure. The medium for viewing these images has changed from film, to receptor plates in computed radiography, to computer monitors in direct digital radiography (DDR) where the X-ray tube and receptor are linked. In order to produce a “whole body” image and not overlook any projectiles or injuries, individual radiographs of the head, neck, torso, pelvis and extremities must be taken separately and then viewed in succession, ensuring all areas of the body are covered. A recent development in the field of radiography has been the introduction of planar whole body digital scanning systems (Lodox Systems Ltd, Saudton, Johannesburg, South Africa). This type of system uses a unique geometry detector configuration and linear slot scanning radiography technology to produce an entire full-body image in seconds. High quality images can be obtained from any angle between the sagittal and coronal planes.
For decades, radiography has been used to document the presence or absence of projectiles, location of projectiles, skeletal injuries, and additional findings such as air in the right atrium and pulmonary outflow tract in an individual with a gunshot wound to the head (19). As long as the projectile is radio-opaque, there is excellent edge detail of the projectile's borders (

Penetrating gunshot wound of the chest from a rifle. Radiographs show a bullet projecting on the scapula. Note scapular fracture (arrow) and right lung opacity.
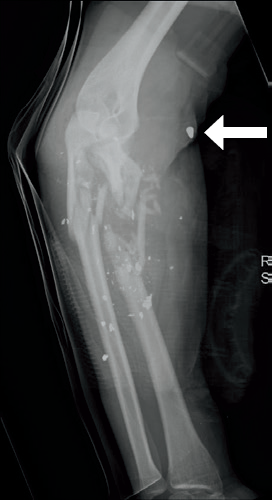
Radiograph of the forearm with a single penetrating gunshot wound. Note bullet fragmentation with comminuted fractures of the radius and ulna. The penetrator tip (arrow) is recognized by its conical configuration.
In computed tomography (CT), the X-ray source and detector rotate around the individual as they are moved through a circular opening on a motorized table. As the detector records the X-rays passing through the individual, this data is sent to a computer that maps the attenuation measurements to picture elements using grayscale. The reconstruction of these data sets produces a series of “slices” or cross-sectional images. Post processing workstations can be used to create multiplanar two-dimensional and three-dimensional images that can be manipulated and reformatted. With multi-detector, helical CT scanners, whole body imaging can be completed in minutes.
Similar to radiography, CT can be used to document the presence or absence of projectiles. In contrast to radiography, the location of projectiles relative to adjacent anatomical structures can be determined in any plane (
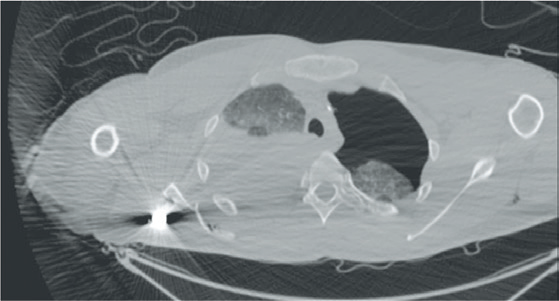
Axial CT of the bullet in Image 2 shows precise location of the bullet posterior to the scapular fracture. Note loss of edge detail by streak artifact. There is a right hemothorax and a left pneumothorax.
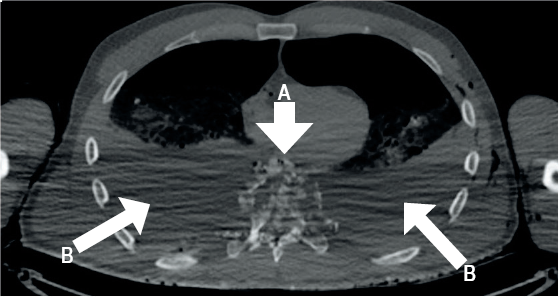
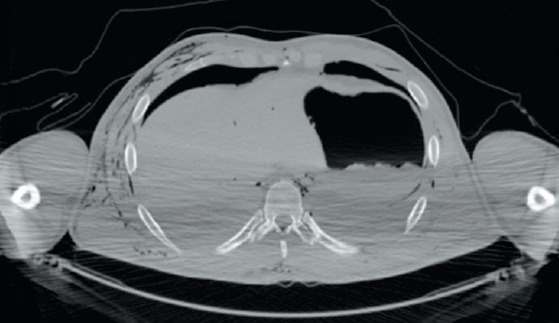
Gunshot wound of the thorax from a rifle shatters the vertebral body with disruption of the posterior elements and spinal canal (arrow A). Bilateral pneumothorax and hemothorax (arrow B) are present.
In many cases, the path of the bullet through the body can be determined using CT. For soft tissue, gas and hemorrhage are the principal markers of the wound track. For bone, fractures and bone fragments in adjacent soft tissue are the principal markers of the wound track (20). In some cases, the direction of the wound track can be determined based on the pattern of fractured bone. The beveling of the skull that has been described in the literature (1, 21, 22) can be demonstrated on CT images. Since the images can be viewed in any plane, it is possible, in select cases, to view the track of the bullet on a single image (
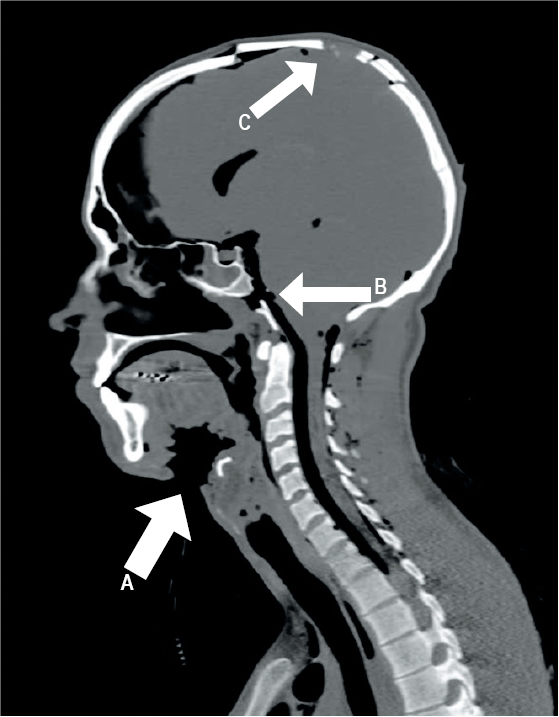
Sagittal reconstruction in the plane of the track shows the submandibular entry wound (arrow A), defect in the clivus (arrow B), and exit at the skull vertex (arrow C).
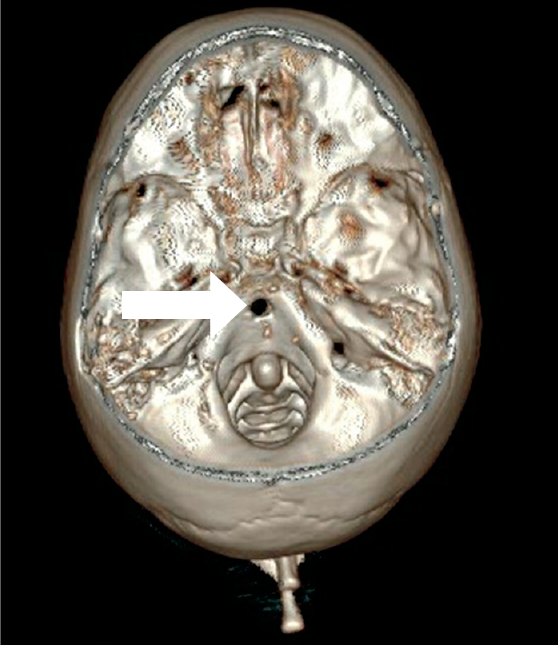
Three-dimensional reconstruction with vertex digitally removed shows the bullet hole in the clivus (arrow).
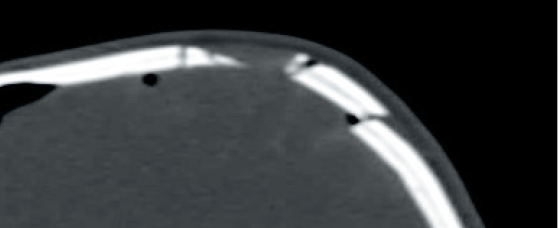
Sagittal reconstruction at the exit wound. Margins of defect demonstrate external beveling.
Axial CT performed without marker does not show the surface wound on the left side of the back.
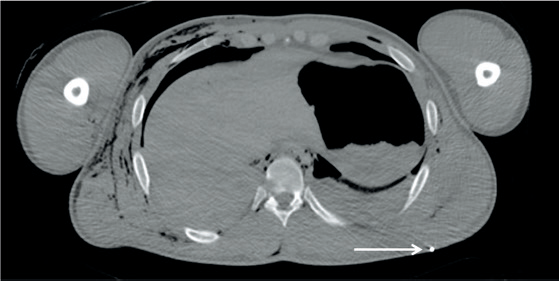
Repeat CT after metallic marker defines the precise location (arrow). Note that a wound in the right chest (not visible on this image) has produced diffuse soft tissue air.
Computed tomography has the potential to help resolve some of the controversies of ballistic wounds such as the degree of wounding by the temporary cavity. For example,
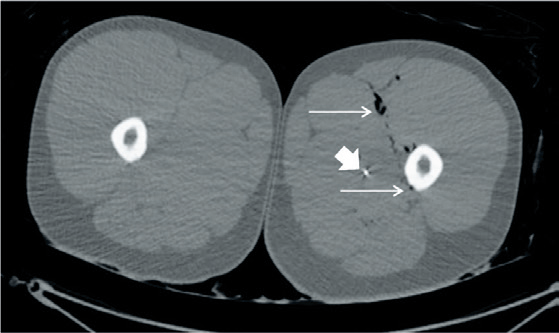
Axial CT of a perforating gunshot wound of the left thigh from a rifle. The soft tissue track (arrows) passes adjacent to the femur without fracture. Note a tiny bullet fragment in the soft tissue (arrowhead).
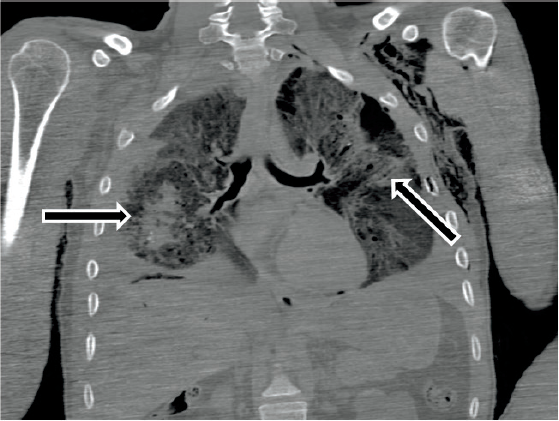
Perforating gunshot wound of the thorax from a rifle. Coronal CT reconstruction demonstrates parenchymal hemorrhage in both lungs (outlined arrows) attributed to the temporary cavity. Note soft tissue air in the left chest wall and axilla.
Magnetic resonance imaging (MRI) uses a magnet to align protons in the body. A radio frequency current is briefly turned on that flips the spin of the protons in the field. After this is turned off, the spin of the protons return and receiver coils capture the radio frequency signal generated during this relaxation phase. Different biological tissues have different relaxation times. The distribution of protons in the body can be mathematically recovered from the signal to create an image. The brightness of the tissue depends on the type of relaxation that is measured. For example, in T1–weighted scans the images depict the differences in spin-lattice relaxation time and water appears darker and fat appears brighter. In T2–weighted scans the images depict the differences in spin-spin relaxation time and water appears brighter and fat appears darker. As with CT, this image can be displayed in any plane. MRI has superior soft tissue contrast resolution as compared to CT. This resolution may allow for further delineation of soft tissue injury created by the temporary cavity (27). In the literature there has been sparse documentation of the use of postmortem MRI in ballistic injury because of the possible presence of ferromagnetic fragments in the body. A main concern is the movement of the ferromagnetic projectiles during the scan as this can distort the forensic findings as well as damage the equipment.
Conclusion
The use of radiologic imaging to study wound ballistics requires integration of imaging data with all information available to the forensic pathologist, in particular the scene investigation and the autopsy itself. Experience to date has demonstrated imaging alone does not allow definitive conclusions about ballistic wounds. Imaging does, however, provide the forensic pathologist with a tool to improve understanding of ballistic wounds both on a case specific basis and as a basic principle. Advancements in imaging have yielded data that can best be understood when it is combined with pathologic findings through careful scientific study.