
Abstract
Drug abuse may involve illicit drugs, prescription drugs, or the combination of illicit and prescription drugs, with or without the use of alcohol. Historically, illicit drugs have been responsible for many of the drug-related deaths investigated by medical examiner and coroner offices. However, in more recent years, deaths resulting from prescription drugs have become increasingly more common. This study reviewed all accidental (unintentional) drug deaths that were investigated at a medical examiner's office over a one-year time frame. The study revealed that prescription drugs made up the largest category of drug deaths, followed by prescription drug/illicit drug combinations, followed by illicit drugs. Drugs capable of causing or contributing to significant respiratory insufficiency such as opioids, benzodiazepines, relaxants (defined as muscle relaxants or sleep medications), and alcohol, or some combination thereof, were detected in 197 out of 256 (77%) of all accidental drug deaths, and were detected in 132 out of 138 (95%) of all prescription drug deaths (cases without any illicit drugs detected). These prescription drugs were most often found in combination, and their similar respiratory depressant effects can be cumulative and deadly.
Introduction
Fatal prescription drug toxicity may result from either the abuse of prescribed drugs, from situations involving unique drug metabolism, or from prescriber error, which may include the cumulative deleterious effects of multiple prescription drugs or inaccurate estimations of a patient's tolerance to prescription drugs (1). In many cases, an individual consumed too many drugs that were prescribed to them, whereas in other cases, the drugs (or at least some of them) were diverted drugs (drugs that were obtained from sources other than the decedent's physicians) (2–4). Prescription drug abuse most commonly involves opioids, followed by benzodiazepines and relaxants, which may be consumed singly or in combination with each other, or in combination with ethanol and/or illicit drugs (5–9).
Deaths from opioid medications are becoming increasingly more common in the United States. Sales of opioid pain relievers quadrupled between 1999 and 2010 (10). In 2008, opioid pain relievers were involved in 14,800 (73.8%) of the 20,044 prescription drug overdose deaths (10). In 2009, emergency department visits related to misuse or abuse of prescribed drugs totaled 1.2 million, an increase of 98.4% from 2004 (10). This issue is not isolated to the United States, as many countries worldwide face increasing prescription drug use and abuse.
Drug abuse can involve many different substances, and may involve either illicit drugs, prescription drugs, or the combination of illicit and prescription drugs, with or without the concomitant use of alcohol. Drug abuse trends are in constant flux, with small or large changes in patterns of drug abuse reactive to different illicit or prescription drugs entering the market and the introduction of different means of drug consumption. Although historically, illicit drug abuse has been responsible for many of the drug-related deaths investigated by medical examiner and coroner offices, in recent years, deaths resulting from prescription drugs have become more common. This study was undertaken to examine and report on the types of drugs involved in accidental (unintentional) drug deaths that were investigated at a medical examiner's office over a one-year time frame.
Materials and Methods
All accidental (unintentional) drug deaths that occurred over a one-year time period (January 1, 2011 thru December 31, 2011) that were investigated by the Travis County Medical Examiner's Office (TCMEO) were included in the study. The TCMEO provides medicolegal death investigation for Travis County (Austin, TX), and also provides autopsy service for a large number of additional counties throughout central Texas. Drug-related causes of death certified by the TCMEO routinely include the word “toxicity” or “toxic” in the cause of death statement. The cases included in the study were retrospectively screened for “tox” (a truncation of “toxicity” or “toxic”) in the cause of death, whether as a primary or a contributory condition, and “accident” for the manner of death. Non-drug-related deaths resulting from toxicity or poisoning such as carbon monoxide toxicity and cyanide toxicity were excluded. Drug deaths were defined as resulting from the toxic effects of illicit and/or prescription drugs with or without the presence of ethanol. Deaths in which drugs may have been a contributory factor in a death, such as fatal physical injury or drowning that was sustained at least in part as a result of drug-induced impairment were not included in the study.
Cases of suspected drug toxicity are routinely autopsied at the TCMEO. All but four of the 256 cases included in this review received a complete autopsy, with microscopic examination performed at the discretion of the particular medical examiner on the case. The four cases that were not autopsied included two hospitalized cases of intracerebral hemorrhage due to acute cocaine toxicity, a case of anoxic encephalopathy due to remote drug toxicity, and a case of a chronic alcoholic with an unexpected high blood concentration of paroxetine. Femoral vein blood, heart blood, urine, and vitreous fluid were routinely sampled on all cases. Femoral blood was placed into 10 mL glass vacutainers preserved with 20 mg potassium oxalate and 100 mg sodium fluoride. Heart blood and urine were placed into separate polypropylene test tubes, and vitreous fluid was placed in a glass vacutainer. Heart blood, urine, and vitreous fluid were not chemically preserved. In cases in which the decedent had been hospitalized prior to death, blood specimens that had been collected by hospital medical staff were obtained for analysis. Following specimen collection or receipt (in the cases of specimens received from a hospital), the specimens were refrigerated at 4°C until analyzed.
Full toxicologic analyses were performed on all cases in this review, except for the three cases of delayed death following drug toxicity that have been previously mentioned (two cases due to intracerebral hemorrhage, and one case due to anoxic encephalopathy). Analysis of specimens was performed by the TCMEO toxicology laboratory, and consisted of screening blood specimens by enzyme-linked immunosorbent assay (ELISA), followed by confirmation and quantification of indicated drugs by gas chromatography-mass spectrometry (GC/MS) or liquid chromatography-mass spectrometry (LC/MS). ELISA screening included cocaine metabolites, amphetamine, barbiturates, benzodiazepines, cannabinoids, opiates, oxycodone, and fentanyl. Ethanol and acetone were screened and quantified by gas chromatography. Suitable quality controls were run in parallel to check assay performance. On occasion, specimens in which assays had not been developed, or were of unsuitable condition for analysis (decomposed) were sent to a referral laboratory (NMS laboratories, Willow Grove, PA) for analysis.
Once pertinent cases were identified and the toxicology results reviewed and tabulated, the case files were reviewed. Because they would not be a significant factor in any of the deaths, morphine, lorazepam, and other drugs that may have been administered therapeutically by emergency medical technicians or by hospital personnel were excluded from the drug tally when their administration was either documented in the EMS or hospital records, or otherwise were deemed likely to have been administered during resuscitation efforts or the ensuing hospitalization. Exempted from this were two cases in which the therapeutic administration of a prescribed drug was believed to be a factor in the death.
Cases in which ethanol was detected were screened for decompositional changes. Ethanol was excluded from the tally in five cases that had low ethanol concentrations and signs of significant decomposition, characterized by green discoloration of the skin, skin slipping, and purge fluid at the mouth and nose. The five decomposed cases consisted of three prescription-only deaths and two prescription drug and illicit drug combination deaths all of which had low blood, vitreous, and/or decomposition fluid ethanol concentrations that generally ranged from 0.02 to 0.03 mg/dL, and up to 0.08 mg/dL in one case. In these five cases, it was believed that the ethanol most likely was generated postmortem by bacteria, and there was no convincing investigative information to suggest antemortem ethanol consumption. Additional case information tallied included the decedent's age, gender, race, and body mass index (BMI).
Toxicology results were interpreted with the recognition that some of the drugs that were detected were likely present as metabolites or impurities. Such substances included morphine (metabolite) and codeine (impurity) present in heroin cases (defined by the detection of 6-monoacetylmorphine), and hydromorphone and oxymorphone, which are metabolites of hydrocodone and oxycodone, respectively. In addition, when only a metabolite was detected (such as nordiazepam or 7-aminoclonazepam), the case was coded according to the metabolite's parent drug.
The cause of death and manner of death were determined based upon careful consideration of the toxicology results in conjunction with the autopsy findings and the complete case investigation. The individual's medical records were routinely reviewed, along with the decedent's drug use/abuse history and possible development of drug tolerance. Additional investigative information included police investigative information and statements from witnesses. Medical examiner investigators routinely performed scene investigations when drug toxicity was a consideration. The decedent's prescription drugs were routinely collected and inventoried.
Results
During the study period, there were 256 cases of accidental (unintentional) drug-related death, comprising approximately 30% of the 857 accidental deaths examined during this time period. The average age of the decedent was 42.8 years (range 16–90 years), and the average body mass index was 29.80 kg/m2 (range 12–90 kg/m2). Deaths from illicit drugs and deaths from a combination of illicit drugs and prescription drugs peaked in the third decade of life, whereas deaths solely from prescription drugs peaked in the sixth decade of life (
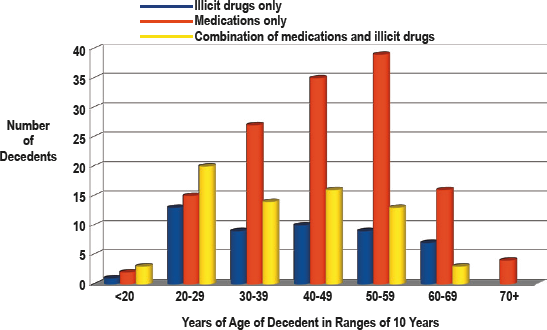
Age distibution of decedents by type of drug.
Cases in which only prescription drugs were detected (no illicit drugs detected) made up the largest category of drug deaths (138, 54%), followed by a combination of prescription drugs and illicit drugs (69, 27%) and illicit drugs only (49, 19%). Multiple drug toxicity made up the vast majority of all prescription drug-related deaths. Only 4/138 (3%) of the prescription drug-only deaths resulted from a single drug (one each of methadone, fentanyl, alprazolam, and hydrocodone).
Alcohol
Alcohol (ethanol) was detected in 55/256 (21%) of all drug-related deaths. Alcohol was detected in 13 (26%) of deaths from illicit drugs, 15 (22%) of deaths from combination illicit and prescription drug deaths, and 27 (19%) of all deaths from prescription drugs without illicit drugs detected. The most frequent prescription drugs detected in combination with alcohol were hydrocodone (13 cases), followed by diazepam (six cases), methadone, diphenhydramine, and morphine (five cases each), and zolpidem (four cases).
Illicit Drugs
The most common illicit drugs detected were cocaine (53 cases) followed by heroin (52 cases) and methamphetamine (18 cases). Two cases had 3,4-methylenedioxy-N-methylamphetamine (MDMA or “ecstasy”), and there was one case each of methylenedioxypyrovalerone (MDPV) and phencyclidine (PCP). Marijuana was detected in 32 cases and was regarded as an illicit drug for case classification purposes.
Prescription Drugs
The most common class of prescription drug detected was opioids, which was detected in 156 (61%) of the 256 cases, followed by benzodiazepines in 120 (47%) of cases, psychiatric medications in 87 (34%) of cases, relaxants (defined as sleep medications or muscle relaxants) in 51 (20%) of cases, and over-the-counter medications in 48 (19%) of cases. The combination of opioid and benzodiazepine medication was present in 89 (35%) of cases.
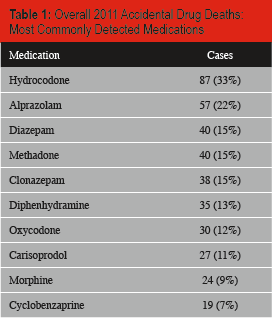
The most common prescribed drug detected was hydrocodone, which was detected in 87 (33%) of the 256 cases. Hydrocodone was followed by alprazolam, which was detected in 57 (22%) of the cases, and diazepam and methadone, which were each detected in 40 (15%) of the cases. Additional commonly detected prescription drugs were clonazepam, which was detected in 38 (15%) of cases), followed by diphenhydramine in 35 (13%), oxycodone in 30 (12%), carisoprodol in 27 (11%), morphine in 24 (9%), citalopram in 21 (7%), and cyclobenzaprine in 19 (7%) of cases (
Overall 2011 Accidental Drug Deaths: Most Commonly Detected Medications
Respiratory Depressants
Of particular interest was the large number of cases that had prescribed drugs which are capable of causing or contributing to significant respiratory insufficiency. Opioids, benzodiazepines, relaxants, or alcohol were detected in 197 (77%) of all 256 drug-related deaths. Excluding the 49 drug deaths in which only illicit drugs were detected, at least one respiratory depressant (prescribed drug or alcohol) was detected in 197/207 (95%) drug deaths that were due at least in part to prescription drug toxicity. Of these 197 cases, 63 (32%) involved any one of the four classes of drug (opioids, benzodiazepines, relaxants, ethanol), 91 (46%) involved any two of the four classes of drug, 39 (20%) involved any three of the four classes of drug, and four (2%) involved all four of the drug classes. Further, 90/207 (43%) of the cases with prescribed drugs detected had greater than one prescribed drug of the same class detected. Fifty-six (27%) of the 207 cases had greater than one opioid detected, 29 (14%) had greater than one benzodiazepine detected, and 13 (6%) had greater than one relaxant detected. Sixteen cases (7%) had greater than one prescribed drug detected in more than one category of medication.
Excluding cases in which illicit drugs were detected, 132/138 (95%) of all deaths related to prescription drugs involved at least one respiratory depressant (including alcohol, which was detected in 30 of the cases). In only six (4%) of the cases were no respiratory depressants detected. Alcohol was the only respiratory depressant detected in four (3%) of the cases. In the other 128 cases, the respiratory depressant was either an opioid (114 cases), a benzodiazepine (77 cases), a relaxant (33 cases), or alcohol in combination with an opioid, a benzodiazepine, or a relaxant (26 cases). Opioids, benzodiazepines, relaxants, and ethanol were often detected in some combination. Of these 132 cases, 108 had at least two of the described respiratory depressants detected, 64 had at least three detected, 24 had at least four detected, 12 had at least five detected, and one case had six detected.
Thirty-one cases (22% of all prescription drug-only deaths) had a pure combination of respiratory depressants (opioid, benzodiazepine, and relaxant with no illicit drugs or ethanol detected). In these cases, the most frequently detected opioid was hydrocodone (23 cases) followed by oxycodone (five cases). The most frequently detected benzodiazepine was alprazolam (15 cases), followed by diazepam (12 cases), clonazepam (10 cases), and temazepam (four cases). The most frequently detected relaxant was carisoprodol (16 cases), followed by cyclobenzaprine (11 cases), zolpidem (nine cases) and butalbital (two cases). In 28 (90%) of these cases, the medications were prescribed to the decedent. In three cases (10%), they were not prescribed to the decedent (diverted medications).
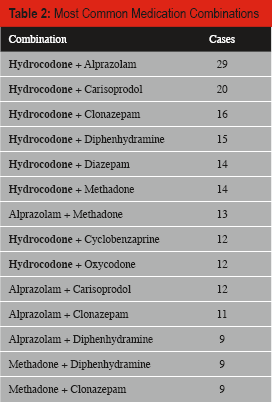
Eight of the nine most common prescription drug combinations involved hydrocodone, with the most common co-ingestants being alprazolam (29 cases), carisoprodol (20 cases), clonazepam (16 cases), diphenhydramine (15 cases), diazepam and methadone (14 cases each), and cyclobenzaprine and oxycodone (12 cases each). The dominance of hydrocodone was interrupted only by the combination of alprazolam and methadone, which was detected in 13 cases
Most Common Medication Combinations
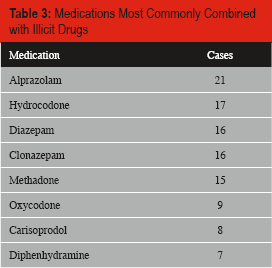
The prescription drugs most commonly combined with illicit drugs were alprazolam (21 cases), hydrocodone (17 cases), diazepam and clonazepam (16 cases each), methadone (15 cases), oxycodone (nine cases), carisoprodol (eight cases), and diphenhydramine (seven cases)
Medications Most Commonly Combined with Illicit Drugs
Discussion
A review of drug-related deaths investigated at a medical examiner's office over a one-year time frame revealed a large influence of prescription drugs, particularly drugs capable of causing or contributing to significant respiratory insufficiency. Opioids, benzodiazepines, or relaxants (defined as sleep medications or skeletal muscle relaxants) were detected in 128 (92%) of all deaths that were due to prescription drugs (deaths that were exclusive of illicit drugs). More than one opioid, benzodiazepine, or relaxant was often detected in an individual case. In addition, the prescription drugs were often combined with alcohol.
Adequate respiration depends upon, among other things, an adequate respiratory drive, an adequate state of arousal, and appropriately functioning pharyngeal dilating muscles. Various combinations of prescription opioids, benzodiazepines, and other hypnosedatives or relaxants such as zolpidem, carisoprodol, and cyclobenzaprine, and alcohol are capable of causing or contributing to significant sedation and respiratory impairment (9) and are frequently found in combination in drug fatalities (11–16). Respiratory impairment may occur with over sedation, and may result from centrally-induced respiratory depression causing decreased respiratory drive, a decreased level of consciousness, and a loss of tone in upper airway muscles which can result in upper airway obstruction (17). The degree of respiratory impairment is likely to be cumulative among these prescriptions drugs when they are consumed in combination and exaggerated when they are combined with alcohol. The respiratory impairment may at first be mild, but become more pronounced as absorption of the substances continues, eventually resulting in apnea (18, 19).
Opioids, benzodiazepines, relaxants, and ethanol can individually and in combination cause a significant degree of sedation, and along with it, some degree of upper airway obstruction, which is more likely to occur in the obese, and in individuals with sleep apnea or obesity hypoventilation syndrome (20–24). At higher doses, opioids can depress all aspects of respiratory activity, including respiratory rate, minute volume, and tidal exchange, resulting in irregular and periodic breathing (25–34). The decrease in respiratory activity is in large part due to opioid-induced decrease in medullary-generated respiratory pattern (central apnea) (35–37). However, opioids can also cause a decrease in hypercapnic and hypoxic respiratory drive (36, 38–41), and can cause an impaired respiratory effort in the setting of increased airway resistance (42, 43). Additionally, if an individual's PaCO2 acutely becomes high enough, central nervous system depression may be exacerbated by the effects of carbon dioxide narcosis.
Although benzodiazepines are generally considered relatively safe from an overdose standpoint (13, 44, 45), they can contribute to significant toxicity when combined with other drugs. In addition to their sedative effects, benzodiazepines can worsen respiratory impairment by causing an increase in upper airway resistance, due in part to depressed activity of the genioglossus muscle, which allows the tongue to relax posteriorly into the hypopharynx (46–49). The genioglossus muscle is the primary airway dilator, and relaxation of the muscle potentiates upper airway obstruction. Benzodiazepines can also attenuate the normal increase in ventilatory response to hypercarbia in a dose-dependent manner, and the normal response to hypoxemia (36, 50–52).
Benzodiazepines, opioids, and prescription drugs that aid sleep such as zolpidem and zopiclone can all cause or contribute to excessive sedation and somnolence when consumed in excess, in combination, or with ethanol (9). The resultant over sedation may cause severe respiratory impairment manifest as central respiratory depression and upper airway obstruction, and prove to be fatal (3, 11, 13–16, 18, 31, 53–59).
Sleep may be a factor in deaths due to prescription drugs that can cause respiratory depression. During sleep, there is no active voluntary control of respirations, which depend upon automatic breathing stimulation and regulation. Normal physiological changes that occur during sleep include decreased minute ventilation, a decrease in PaO2, an increase in PaCO2, decreased response to hypoxia and to hypercarbia, decreased upper airway muscle tone causing increased airway resistance, and decreased intercostal muscle activity (60–64). All of these potentially deleterious respiratory effects may be augmented by similar effects induced by opioids, benzodiazepines, relaxants, or ethanol, either individually or in combination, possibly resulting in apnea (21, 22, 65–72).
Obesity may be an additional factor in deaths due to prescription drugs that can cause respiratory depression. The average body mass index (BMI) of all drug-related cases in this study was 29.80 kg/m2 which borders on obesity (generally defined as a BMI of 30 kg/m2). An abundant amount of adipose tissue mass about the chest and abdomen can hinder expansion of the rib cage during inspiration. Additional abdominal and mesenteric adipose tissue mass can hinder excursion of the diaphragm during inspiration. Additional adipose tissue bulk about the pharynx and hypopharynx can predispose to upper airway obstruction. All of these factors can cumulatively result in significant impairment of an individual's ability to adequately breathe. Up to 30% of obese individuals have been shown to have isolated hypoxemia, which intensifies as the degree of obesity increases (73).
Only four of 207 prescription drug-related fatalities had only a single medication detected. The large number and extent of multi-drug intoxications is reflective of the potential hazards of the cumulative effects of multiple prescription drugs. It is also likely reflective, at least to some extent, of the willingness of individuals to explore various effects from different combinations of medications or to self-treat with certain medications if an ill effect is achieved. Such drug mixing has been reported elsewhere. In a study of 70 oxycodone toxicity deaths, psychoactive substances other than oxycodone were detected in all cases, with the most common classes being hypnosedatives (68%-most commonly diazepam), other opioids (54%-most commonly codeine and morphine), antidepressants (41%-most commonly tricyclic medications), and ethanol (33%) (74). The combination of opioids and benzodiazepines can be particularly able to induce significant sedation, respiratory insufficiency, and apnea in humans (36, 75).
Scene examination often finds the decedent who has succumbed to the effects of prescription drug toxicity in bed, or on a sofa, chair, or other resting/sleeping situation. The decedent is frequently found prone, sometimes with their face resting on a soft pillow, blanket, cushion, or other surface that could potentially impair adequate respiration. Suffocation, smothering, or positional asphyxia may be evident, enhancing the importance of scene investigation in cases of suspected drug toxicity. Foamy fluid is frequently observed at the mouth and/or nose, reflective of pulmonary edema and congestion. Autopsy findings in these cases often include heavy lungs due to edema and congestion. The pulmonary edema and congestion are likely, at least in part, due to over-sedation resulting in 1) hypoxia with resultant cardiovascular depression and 2) upper airway obstruction with resultant negative pressure pulmonary edema (20, 76–78). The lungs may have early acute pneumonia and the urinary bladder may contain a large amount of urine, reflective of a prolonged agonal/comatose time period preceding the death (79). Aspiration of oral secretions and/or food material is likely to precipitate a mild acute inflammatory reaction if survival time is long enough.
The drug concentrations may be less than impressive, particularly if the agonal period had been prolonged, allowing for significant metabolism of drugs, often to therapeutic, less-than-therapeutic, or seemingly insignificant concentrations if considered in isolation (79). However, when considered within the context of the complete case investigation, and with consideration of prolonged opportunity for drug metabolism, the significance of less-than-impressive drug concentrations often achieves greater importance.
Study Limitations
During the study period, there were 19 suicidal deaths resulting from drug and/or ethanol toxicity. Distinguishing between accidental and suicidal drug toxicity can be difficult in some cases, but was made upon consideration of all the information available on the case. When a sufficient amount of information needed to classify a case as a suicide was absent, the default was to classify the death as accident. It is possible that some of the deaths classified as accidents were in fact suicides. Some of the cases classified as accidental drug-related deaths had a significant amount of cardiac pathology and other natural disease. The diagnosis of toxicologic drug death and cardiac death are to a large extent diagnoses of exclusion. The effects of the two conditions may be combinatory in some cases. It is possible that some of the individuals with a significant amount of natural disease could have died with the prescription drugs, rather than from them.
Conclusion
Drugs capable of causing or contributing to a significant degree of respiratory insufficiency are a leading cause of drug-related death. Opioids, benzodiazepines, relaxants, and alcohol (or some combination thereof) was detected in 197 out of 256 (77%) of all accidental drug deaths examined at a medical examiner's office in 2011, and were detected in 132 out of 138 (95%) of all prescription drug-related deaths (cases without any illicit drugs detected). One should be aware of the ability of opioids, benzodiazepines, relaxants, and alcohol both individually and in various combinations, to impair respiration to the extent of resulting in apnea and death. These drugs are most often found in combination, and their similar respiratory depressant effects can be cumulative and deadly.
Footnotes
The author, reviewers, editors, and publication staff do not report any relevant conflicts of interest.