
Abstract
An autopsy is a significant event and should not be undertaken for simply narrow purposes. Forensic pathology institutions, whether in coronial or medical examiner jurisdictions, should be actively engaged in research, either directly or by facilitating access to bodies, tissues and data. The challenge, assuming that resources are available, is to do this lawfully, ethically, and in accordance with community expectations. Failure in the challenge will be wrong and cause damage to the reputation of the institution. The risks associated with such research therefore need to be managed. An approach which is transparent and based on respect for the deceased and consent for the activity, while no guarantee of success, is likely to engender community confidence in the activity and in those undertaking it.
Introduction
Where is the starting point? Alan Greenspan and the U.S. Treasury is as good a place as any!
“Trust and reputation can vanish overnight.” (1)
So it proved at Arthur Andersen LLP, the huge multinational auditing firm, which collapsed following its breaches at Enron, breaches which were causally involved with Enron's demise. Arthur Andersen collapsed because the nature of its work required that it be trusted by clients and stakeholders to behave properly. As soon as Arthur Andersen acted improperly, the company lost that trust, and the business folded. So it is with the forensic sciences. We produce observations and opinions which, ultimately, have to be believed to have their impact. In forensic pathology, we are also trusted to look after deceased persons whose bodies have been compulsorily taken by the state from the care of their families. We cannot do our work unless we do it well AND people trust us. Without that trust we cannot fulfill our mission.
One of the sources of the community's trust in us is that we are medical professionals, people who take seriously the ethical obligations of being a doctor, and more specifically of being a forensic pathologist. Another source of trust is the reputation which attaches to the organization for which the forensic pathologist works. That reputation is not only of an academic or intellectual kind; it includes a reputation for how the organization and its staff deal with people, and especially the deceased.
A second starting point for the discussion about ethics and research in forensic pathology is the autopsy itself. The autopsy is a very significant event ethically, because it interferes with the body. Such a significant event should not be undertaken for only narrow purposes. The community might reasonably expect an institution responsible for autopsies to establish lawful and ethical procedures which would ensure that, to the greatest extent possible, the benefits of the autopsies are realized. If an autopsy is to take place, and there is no attempt by those responsible to inform families about what was found, to try and answer questions the family might have, to communicate the findings to the deceased's doctors, to make tissue available for transplantation or for research, or to use the opportunity of the autopsy for teaching medical students or pathology fellows, then it could be said, taking into account legal and resource constraints, that this is not good enough. The autopsy, an event of major ethical significance, has perhaps been undertaken for the relatively narrow administrative aim of “establishing” the cause of death and filing it.
So, the authors’ orientation in this paper is that research involving bodies coming into the jurisdiction of the coroners/medical examiners is desirable. The challenge is to do this ethically and legally, in a way which accords with community expectations and customs.
What is Research?
In Australia, The National Health and Medical Research Council (NHMRC) has published a National Statement on Ethical Conduct in Human Research (the National Statement) (2). It provides guidelines to Human Research Ethics Committees (HREC), comparable to the Institutional Review Boards in the U.S., on the ethical review of research and “also emphasizes institutions’ responsibilities for the quality, safety and ethical acceptability of research that they sponsor or permit to be carried out under their auspices” (3).
The National Statement acknowledges that there is no agreed definition of research but that it is “widely understood to include at least investigation undertaken to gain knowledge and understanding” (4). This definition is broader than that of the U.S. Code of Federal Regulations, Protection of Human Subjects that defines research as meaning “a systematic investigation, including research development, testing and evaluation, designed to develop or contribute to generalizable knowledge” (5). Further, the U.S. Belmont Report makes the distinction between research and practice, defining research as designating “an activity designed to test an hypothesis, permit conclusions to be drawn, and thereby to develop or contribute to generalizable knowledge” (6). There are “grey areas” that could be regarded as research or could be better described as quality assurance, case reviews, case reports, training and education. All of these activities must be undertaken legally and ethically – and meet broad community expectations of respect for the deceased, for human tissue (including fluids) removed from the deceased, and for data derived from the death investigation while respecting the privacy of the deceased individual. But these grey areas may not be subject to the requirements of ethical review by a Human Research Ethics Committee, which has been established under the auspices of the NHMRC National Statement, as technically, these activities centred on deceased individuals may not constitute human research. Significantly, the Belmont Report dictates that “the general rule is that if there is any element of research in an activity, that activity should undergo review for the protection of human subjects” (6).
What is Human Research Requiring Ethical Review?
In Australia and elsewhere, research involving humans must be reviewed and approved by a HREC established in accordance with ethical guidelines. The Australian guidelines define “human research” as research that is “conducted with or about people, or their data or tissue.” Human participation in research is therefore to be understood broadly, to include the involvement of human beings through taking part in surveys, being observed by researchers, access to their information, the collection and use of their body organs, tissues or fluids (7). Although the National Statement is mostly directed towards research involving live humans, it does contemplate the use of cadaveric tissue for a research purpose. It states that “any wish expressed by a person about the use of his or her post-mortem tissue for research should be respected” and “if no such wish is discovered, consent for the use of the tissue should be sought from the senior available next of kin” (8). The U.S. Code of Federal Regulation has a narrower application defining a “human subject” as “a living individual about whom an investigator conducting research obtains data through intervention or interaction with the individual or identifiable private information”, intervention including a physical procedure by which information is gathered such as venepuncture (5). Notwithstanding this ambiguity, the Victorian Institute of Forensic Medicine (VIFM) established an institutional HREC to specifically deal with its issues around cadaveric tissue and data use in research and related projects.
Law and Ethics
It is simple to say that research using human tissue and information must be both lawful and ethical. Law and ethics sometimes diverge, however, and it can be complicated to define and disentangle these frameworks. By its very nature, law can lag behind community expectations or ethical practice. The law may authorize practices that are no longer considered ethical because community expectations have changed. Governments are often reluctant to voluntarily revisit legislation regarding the use of human tissue as it provokes passionate debate on moral and religious issues about definitions of death, attitudes towards the human body following death and questions of informed consent. Sometimes such legislation is forged in response to acute public concern, as was the case in the United Kingdom. There, the Human Tissue Act (9) was completely overhauled following the Bristol Royal Infirmary (10) and Alder Hey (11) scandals involving the unlawful removal and retention of organs from infants and children undergoing autopsy.
Laws can also be considered to be unethical from their inception – for example, capital punishment or the detention of asylum seekers for indefinite periods. In these instances, ethical behaviour and legally sanctioned action may be viewed to be in direct opposition. In Victoria, Australia, current practice guiding the use of tissue removed from bodies within the coronial jurisdiction for research purposes generally applies a standard over and above the requirements of legislation. There is statutory provision to use tissue removed from a body under the authority of the Coroners Act (for example during autopsy) for scientific purposes without also obtaining the consent of next of kin. This makes a large range of organs and tissue legally available for research—as demonstrated in Table 1—without the legal requirement to go back to families to discuss the use of tissue for such purposes. Since the late 1990s, this provision has not been relied upon. Ethical requirements demand (8), and the community expects, that consent by the senior available next of kin should be obtained, unless specifically waived by a HREC. In practice waiver is only considered for stored tissue used anonymously: primarily blood samples and histology slides.
Tissue Available During the Medicolegal Death Investigation
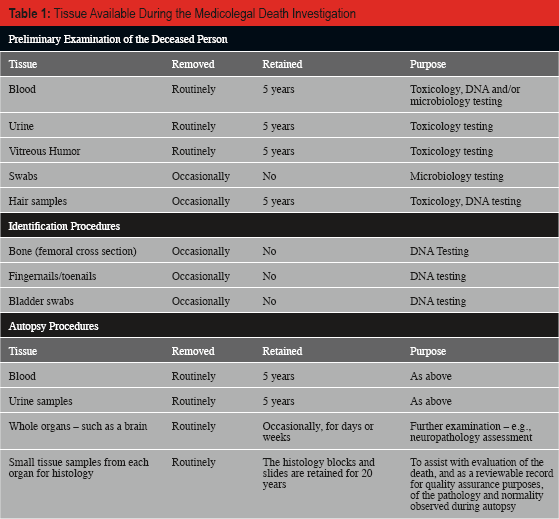
What Tissue and Data about Deceased Persons is Available?
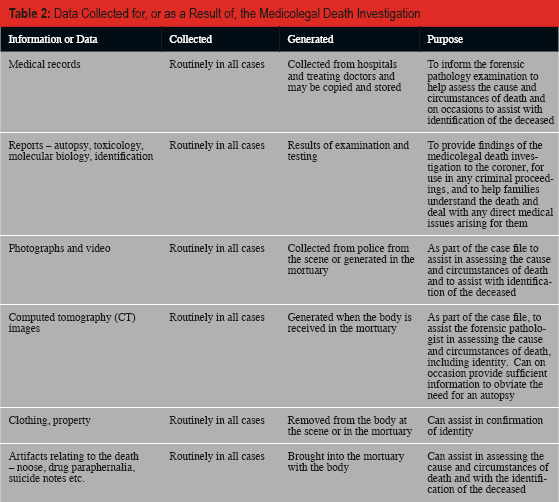
This is likely to be quite similar in many coronial and medical examiner jurisdictions around the world, although Tables 1 and 2 represent practice at the Victorian Institute of Forensic Medicine.
Data Collected for, or as a Result of, the Medicolegal Death Investigation
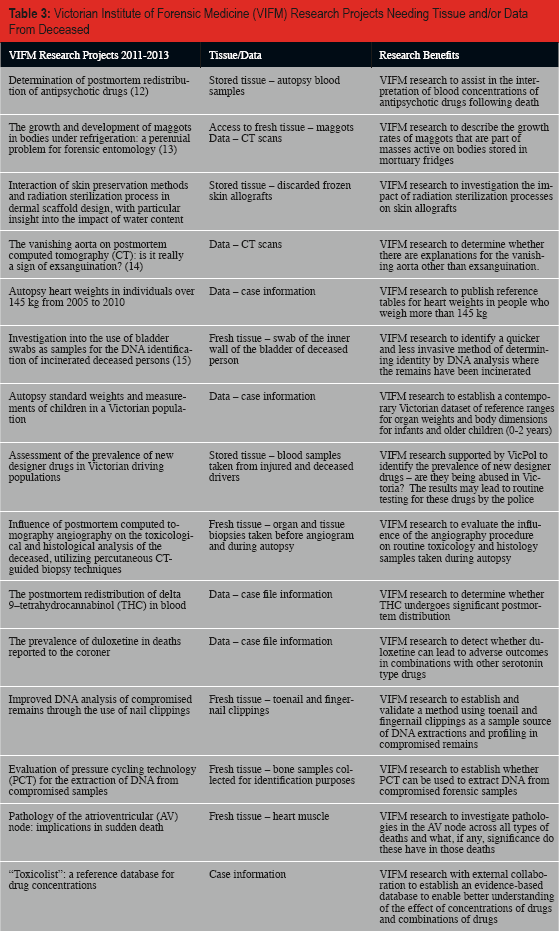
What Research Projects have Needed these Tissues and Data?
In the Victorian coronial jurisdiction, human research projects have been quite varied in their nature. They have involved access to fresh postmortem tissue and whole organs, access to the bodies of a deceased person to practice a surgical procedure, autopsy procedure or to test a device, access to maggot masses found on a deceased person, access to information about a person including the results of scientific testing or cause of death, use of computed tomography (CT) scans, DNA analysis of blood samples and interviews with family members.
Many research projects have been undertaken by staff members of the VIFM in order to improve the medicolegal death investigation. The research has led to greater understanding of the cause of death, less invasive procedures for establishing the cause of death, better analysis of toxicology results, quicker and less invasive provision of a DNA source for human identification, and improved methodologies for the retrieval and processing of tissue donated altruistically for therapeutic use. Beneficiaries of the research reach beyond the coroner to include the families of the deceased, the Victorian justice and health systems and the individual families of the deceased. Some references to publications arising from the research are included in Tables 3 and 4.
Victorian Institute of Forensic Medicine (VIFM) Research Projects Needing Tissue and/or Data From Deceased
Research Projects in which Victorian Institute of Forensic Medicine (VIFM) Facilitated Access by External Researchers to Tissue and/or Data from Deceased
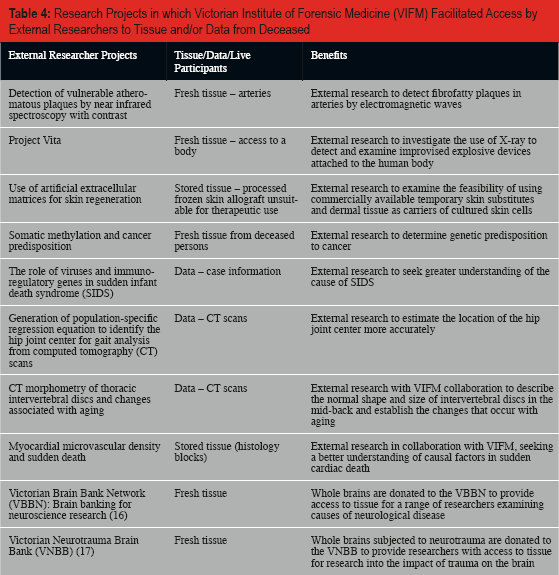
The VIFM also supports research undertaken by external researchers in the areas of public health, safety (including prevention of injury) and the administration of justice.
An Approach Based on Respect and Informed Consent
Respect
What constitutes respectful treatment of human remains? Whether a particular action is respectful or disrespectful is in part contextual and depends on the intent or motive accompanying the action and its objective. For example, the dissection of bodies and the removal of organs by forensic pathologists in a coronial or medical examiner jurisdiction may superficially appear similar to the removal of organs, for sale by the mortuary manager, from bodies donated to a major medical school, University of California Los Angeles (UCLA), in 2009 (18). From the perspective of whether these actions violate the principle of respect for human remains, there is a clear difference between the authorized dissection of bodies to determine cause of death and an illegal trade in organs.
As implicit in the above paragraph, we have approached the issues which are the subject of this paper, not only as issues of inherent academic interest, but also as issues that require management in the interests of all involved. We firmly believe forensic pathology institutions should undertake and participate in research, either directly themselves or by providing access to tissue and data for use by others. But undertaking this activity is a significant risk to reputation, and thus needs to be managed. Establishment of an HREC, with external community representation and in our case, also an external chairperson, has been a key component of our approach.
Are ethical guidelines needed? In the living, they protect the patient from any morbidity, mortality, pain, distress and suffering associated with the research. The principles of beneficence, non-maleficence and respect for the autonomy of patients, who are often in a vulnerable position in terms of knowledge, need and status compared to the doctor or researcher, help protect them from being harmed or wronged. None of these are applicable to the dead, as one cannot harm the dead. Although it has been suggested that “harm to the deceased may derive from further dissection and invasion which might be considered mutilation and desecration of the decedent's body, disturbance of quiet repose” (19). Be that as it may, one can, of course, harm the deceased's next of kin, their friends, and their community. One might argue that there is no ethical duty owed to those groups by the pathologist or the pathology institution; they are certainly not the pathologist's patients. But many pathologists and pathology institutions do feel they have duties to those groups arising indirectly through their “doctor-patient-like” association with the deceased. Certainly, when those groups believe they have not been respected, they will focus their displeasure on the pathologist and his or her institution, believing that both indeed had obligations to them that have been breached.
An approach based on respect includes the honoring of antemortem decisions or preferences of the deceased. Although U.S. law generally finds that rights of individuals are “extinguished” at death (19), there is specific legislation that extend them. For example, the U.S. Uniform Anatomical Gift Act authorizes the giving or withholding of consent by a person “for transplantation, therapy, medical or dental education, research, or advancement of medical or dental science” of their bodies after death (20). In other contexts the rights of people do not completely extinguish on their deaths. The trustee of an estate, the postmortem manifestation of the antemortem person, is obliged to carry out the will of the person. A promise made to a person is not necessarily extinguished with the death of the person. If we promise to look after a person's son when that person dies, this is a promise owed in the strongest moral sense, even though there may be no one to hold us to account. Insofar as a family might be harmed by breaches of the deceased's privacy, the family has rights. In Victoria, the health information of a deceased person is protected for 30 years following his or her death (21). In the case of Editions Plon v France, which concerned the publication of the book Le Grand Secret by Dr. Gubler following the death of former French President Mitterrand, the Paris Tribunal de Grande Instance held that by disclosing information about Mitterrand's medical treatment in breach of rules of medical confdentiality, Dr. Gubler (the author) and Plon (the publishing company) had committed a wrongful act incurring civil liability. It ordered the ban on publication of Le Grand Secret to remain in force and the defendants jointly to pay Mrs. Mitterrand FRF 100,000 and each of her three children FRF 80,000 in damages. The court order intended to “protect the deceased president's honor, his reputation and the intimacy of his private life” and found that the breach of legal confidentiality was capable of infringing the rights of others - Mitterrand's surviving wife and children (22).
Giving moral weight to antemortem preferences or decisions demonstrates respect for the living in the same way that honoring promises is respectful: it really does not matter whether the promisee dies; the promissor is still obliged by the promise. It also promotes the well being of the living. Reassurance that one's plans, preferences and values will be respected is a comfort to people while alive. This can only be sustained if they are indeed respected as a societal norm after death.
Respectful treatment does vary with time, culture, and groups. In the U.S., what constitutes abuse of corpses for the purposes of the model penal code refers to the family: “Except as authorized by law, a person who treats a corpse in a way that he knows would outrage ordinary family sensibilities commits a misdemeanor” (23). This formulation of the definition of “abuse” allows for that cultural, group and temporal variation in perception.
Other recognized ethical requirements for the conduct of research involving deceased people are based on the notion of respect. For example:
The research should address a significant, not a trivial, question; Invasiveness should be minimized and justified; The duration of the research should not be excessive; Confidentiality should be protected; Conflicts of interest should be avoided; and Costs should be borne by the research and not the family or deceased's estate (24).
We are facing a significant growth in the range of potential uses of the human body postmortem in therapeutics, research and teaching. The debate about whether, and if so to what extent, fundamental human rights apply to the dead will continue. Can a person make future binding decisions about his or her corpse against the interests of society or the interests of his/her family?
In Victoria, it is unlawful to remove tissue from a deceased person for transplantation or other therapeutic, medical or scientific purposes, where the medical practitioner has reason to believe that the deceased person has during his or her lifetime expressed an objection, orally (before two witnesses) or in writing, to the removal of tissue from his or her body following death (25). The next of kin cannot override that expressed wish of the deceased. And an HREC cannot waive the requirement for consent, but must respect the wishes of the deceased person (8). What if that tissue could save or enhance the life of the deceased's child? What if that tissue could assist in the research of the condition from which the deceased died?
In the absence of such decisions and available next of kin, is it right, and if so to what extent, for society to make decisions about what can happen to that body? (26) For example, would it be considered ethical to use tissue retrieved from unidentified bodies or unclaimed bodies, where there is no recorded wish of an objection to such use, for life saving tissue donation such as skin allografts for burns victims or heart valves for critically ill patients? What if the tissue is to be used for a second or third generation tissue product – for life enhancing rather than life saving objectives?
Informed Consent
Ensuring that participation in research is truly voluntary, that informed consent is obtained from participants, is a means of ensuring that they are treated respectfully. In the context of research on the deceased, the requirement to seek and obtain informed consent prevents use of the body in a way that is incompatible with the deceased's antemortem preferences and values. It protects the deceased's body from being dealt with disrespectfully (something which has individual aspects as well as cultural). The requirement for informed consent also protects and respects the deceased's family (27).
Voluntariness is the basis of most ethical codes for human research. The Nuremberg Code requires that “the voluntary consent of the human subject is absolutely essential” (28). The Belmont Report states that:
“Respect for persons requires that subjects, to the degree that they are capable, be given the opportunity to choose what shall and shall not happen to them. This opportunity is provided when adequate standards of informed consent are provided” (6).
The Australian National Statement on Ethical Conduct in Human Research also requires informed consent from human participants as a basis for all research. It states that “consent to participate in research must be voluntary, and based on sufficient information and adequate understanding of both the proposed research and the implications of participation in it” (29). This requirement does not always sit easily with research using tissue and information about deceased persons. We rarely, if ever, know whether the deceased has expressed an objection to the donation of tissue from his or her body after death. Our practice, in accordance with the National Statement (8), is to replace the base requirement for obtaining informed consent from a living participant, with obtaining informed consent from the next of kin. It can be difficult to assess notions of risk, which determine levels of ethical review and whether it is appropriate to waive the requirement for informed consent, where the participant in the research is dead. The VIFM HREC assesses the risk of harm to the next of kin in the context of seeking informed consent for the donation of tissue or information for research where that person has lost a relative unexpectedly and tragically, which is the usual situation in deaths reported to a coroner or medical examiner. The requirement to seek informed consent from the next of kin will be waived when the VIFM HREC considers that contacting a family who has lost a relative tragically – often some years prior to the research being undertaken – would cause greater harm that not consulting them at all. The research must have sufficient value and public benefit to warrant the waiver of the requirement to seek informed consent. The requirement for informed consent is routinely waived where the research is seeking the use of de-identified information (such as CT scans) or anonymized stored tissue that has been removed for the purposes of the autopsy some time previously. This is authorized in Victorian law, even where the deceased person has expressed a wish that his or her postmortem tissue is not used for research (30). Although, if we were aware of this express wish, the tissue would not be used for research on ethical grounds (8).
How should we approach the respectful treatment of unclaimed or unidentified bodies where it is not possible to seek the informed consent of next of kin or to know the antemortem wishes of the deceased? There is a long history of using unclaimed bodies for anatomical dissection or research purposes, a practice authorised by Anatomy Acts that Parliaments have enacted to shore up the legal supply of bodies to Anatomy Schools and to stamp out the black market in corpses (e.g., Anatomy Act 1832, England). In Victoria, there is legal authority for the removal of tissue or organs from a deceased person where the medical practitioner is unable to ascertain the whereabouts of the next of kin (after making reasonable inquiries) and he or she has no reason to believe that the deceased person had expressed an objection to the removal after his death of tissue from his body (31). In practice, this provision is not relied upon. For purely operational reasons, institutions such as the VIFM are unable to use tissue therapeutically where a medical and social history of the deceased person cannot be ascertained. In research, the use of an unidentified or “unclaimed” body is considered unethical, as it is not possible to meet the consent requirement, with the limited exception of unidentified skeletal remains where small samples are used for internal quality assurance research. Community debate in this area is needed.
Transparency
As a means of ensuring public confidence in medical and research institutions, and to reduce the possibility of abuse of the privilege of having access to human tissue and data, ethics governance of research demands levels of transparency. Ethics committees are generally required to have some non-institutional community-based membership to participate in the review and approval of proposed research projects. In Australia, the NHMRC National Statement requires HRECs to have at least one third of its membership from outside the institution, as well as the inclusion of at least two lay people (one man and one woman) who have no affiliation with the institute and do not currently engage in medical, scientific, legal or academic work (32). Scrutiny of research proposals by members of the community external to an organization should discourage institutional cultures that tolerate the misuse or abuse of human tissue and data. In practice, this depends on the culture of the HREC and the engagement in the process by the external members. Do the external lay members of the committee feel sufficiently confident to question research proposals and practices that are presented to them by the medical and research experts? At the VIFM we have tried to address this issue by ensuring that the number of external members of our HREC outweighs the number of internal members and by selecting the Chair from this group of external members.
The provision of annual reports by researchers to the HREC, the peer review of papers submitted arising from the research, minutes of meetings from the HREC provided to the governing body of the institution and annual reports from the HREC included in the annual report of the institution, are all means of ensuring transparency and accountability in research. Again, all of this can happen and unethical practices can still occur. How successful research governance proves to be is largely dependent on the culture of the organization in which the research is undertaken. For example, what behaviors are tolerated by colleagues and managers?
Where Respect and Consent does not form the Basis of Research
Unfortunately, there are many examples in the history of human research where consent from participants or next of kin has not been sought or obtained for research projects: the Tuskegee Syphilis Study, Nazi German scientific research on concentration camp prisoners, hepatitis experimentation on mentally disabled children at the Willowbrook State School, and Stanley Milgrim's electric shock experiments (33).
The scandals are not limited to the living. Between 1967 and 1985, pituitary hormones were officially supplied to 1,976 Australians as treatment for infertility and short stature. The program relied on pituitary glands removed at autopsies. Some of those in receipt of the hormones developed Creutzfeld Jakob Disease. In an independent Government inquiry into the program, it was concluded that pituitaries were not removed by pathologists generally, but by technicians. Most often the pathologists never got to see them or asked to see them, and the macroscopic and microscopic appearance of the gland did not form part of the evaluation of the pathology in virtually all cases. Thus, it was concluded that the glands were not removed for the purpose of the autopsy and therefore their use for therapeutic purposes was not authorized by the law (as described above). The glands were removed solely for therapeutic purposes and this required separate consent or authority. The removals were not lawful and those adversely affected were therefore entitled to recompense (34). (One of us [SC] recalls being a trainee pathologist aware that this was occurring, and thinking at the time what a good thing it was. We need to be alert to the significance of what is going on around us).
As mentioned earlier, the willed body program at UCLA was co-opted for a lucrative and illegal trade in body parts for personal gain. One article assumed readers would be disturbed to learn that corpses were “mangled in automobile crash tests, blown to bits by land mines or cut up with power saws be shipped in pieces around the country or even abroad” (35).
It is easy to see why such examples undermine public confidence in and the reputations of medical and research institutions. The effects can be broad and long lasting. In the U.S., with a population over 300 million, there are only about 20,000 body donations per year (36). Most organ and tissue donation agencies have observed that negative press coverage of a postmortem organ or tissue issue has an immediate downward impact on donation rates by next of kin.
Conclusion
Forensic pathology institutions, whether in coronial or medical examiner jurisdictions, should be actively engaged in research, either directly or by facilitating access to bodies, tissues and data. The challenge, assuming that resources are available, is to do this lawfully, ethically, and in accordance with community expectations. Failure in the challenge will be wrong and cause damage to the reputation of the institution. The risks associated with such research therefore need to be managed. An approach that is transparent and based on respect for the deceased and consent for the activity, while no guarantee of success, is likely to engender community confidence in the activity and those undertaking it.
Footnotes
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest.