
Abstract
Prescription drug abuse has increased in the United States in part because of the relative ease of acquisition. Some drug abusers resort to the injection of crushed tablets for rapid onset and increased euphoria. Adolescents and young adults with chronic pain disorders and intravenous access ports are particularly susceptible to this practice. Clinically, those who inject tablets may develop dyspnea, hypoxemia, pulmonary hypertension, and are at an increased risk of sudden death. In addition to the active ingredient(s), pharmaceutical tablets contain inert excipients such as talc, starch, microcrystalline cellulose and crospovidone. Angiothrombosis and foreign body granulomatosis induced by particulate emboli are the major pathological findings identified. Tablet excipients can be discerned by their morphological and histochemical attributes. Microanalytic techniques may be required for definitive identification. Inhalational exposures, aspiration, endogenously formed crystals, and hyperalimentation are potential mimickers of tablet-induced foreign body emboli and granulomatosis.
Keywords
Introduction
In 2010, an estimated 22.6 million Americans aged 12 or older were current illicit drug users, of whom seven million used prescribed drugs for nonmedical purposes (1). The nonmedical use of prescribed drugs is second only to marijuana as the most common form of illicit drug use. Prescribed drugs are relatively easy to obtain, with more than 50% of American drug users receiving them free of charge from a friend or relative who may have received the drugs by prescription from a licensed physician (1).
A relatively common practice in this setting is the intravenous (IV) injection of aqueous suspensions of pharmaceutical tablets for the purposes of rapid drug delivery and heightened euphoric effect. Pulmonary foreign body embolism and granulomatosis due to inert and insoluble tablet components are the principal pulmonary vascular complication of IV drug abuse (2–5). Medications used in this manner include methadone, hydrocodone, oxycodone, methylphenidate, amphetamine sulfate, codeine, propoxyphene, tripelennamine, phenmetrazine, and pentazocine (5–11). The intravenous injection of pentazocine tablets, for example, was so widespread in the 1970's that the manufacturer added the opiate antagonist naloxone to the formulation to interfere with the narcotic effect (4).
Adolescents and young adults with chronic illnesses like cystic fibrosis, sickle cell disease, inflammatory bowel disease, and malignancy may be at a higher risk of this practice because of indwelling vascular access ports and prescription pain medications (9, 12, 13). Additionally, there have been cases that describe foreign body embolism and granulomatosis in psychiatric patients attempting to create factitious disorders, or as a modus operandi for murder (14, 15).
Tablet Production and Components
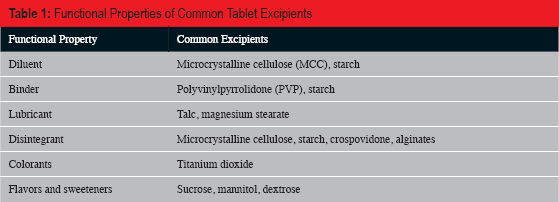
Pharmaceutical tablets are the most common vehicle for the administration of drugs. Tablets are produced under pressure in tableting machines in which the active ingredient(s) is admixed with inert, soluble or insoluble substances called excipients and compressed in a tablet mold (16, 17). The most common categories of excipients and the materials most likely to be encountered in the lung following intravenous injection of tablets include diluents, binders (which render the tablet more cohesive), lubricants (which minimize adherence of the tablet to the mold), disintegrants (which promote the dispersion of the tablet active ingredients), colorants, flavors and sweeteners. Many excipients serve multiple functions in tablets. Important materials in each of these categories are listed in
Functional Properties of Common Tablet Excipients
Tablet Excipients and their Staining Properties
The most frequently encountered and widely recognized excipients in the lung following intravenous injection of pharmaceutical tablets are talc, cornstarch, microcrystalline cellulose, and crospovidone (2). Usually, a mixture of excipients is present in the same lung. Tablet excipients may have distinctive histochemical staining properties and /or characteristic birefringent appearances when viewed under polarized light, which facilitate their recognition in histological sections (
Characteristics of Common Tablet Excipients
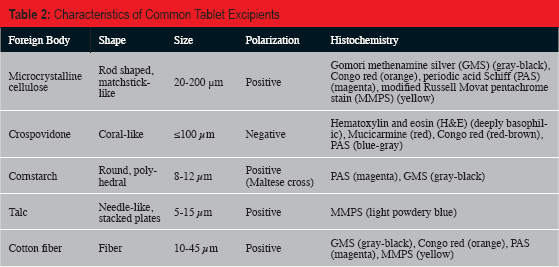
Talc, a hydrous magnesium silicate (Mg6(Si2O5) 4(OH)4), has been the most frequently reported embolized tablet excipient (19, 20). However, since most studies have not used microanalytical techniques for the identification of foreign materials, and due to the great overlap in the appearance of particles observed using polarized light microscopy, it is likely that talc has been over-reported. In our experience, microcrystalline cellulose is encountered more frequently than talc. The presence of talc can be suspected upon observation of short (5–15 μm in length), refractile, highly birefringent, needle-like crystals appearing in aggregate as “stacked plates” (
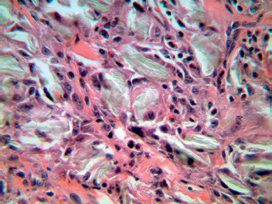
Talc. Refractile, needle-like particles, aggregating as “stacked plates,” with foreign body reaction (talc pleurodesis; H&E, x400).
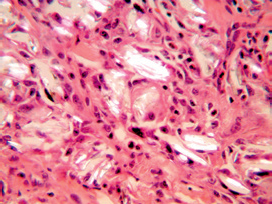
Talc. Brightly birefringent talc crystals (talc pleurodesis, polarized light; H&E, x400).
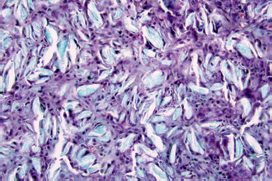
Talc. Crystals stain light blue with Movat pentachrome stain (talc pleurodesis, x200).
Cornstarch is a round or polyhedral particle which measures roughly 8–12 μm. Under polarized light microscopy, starch particles show central “Maltese cross” birefringence, and are associated with poorly developed microgranulomas (
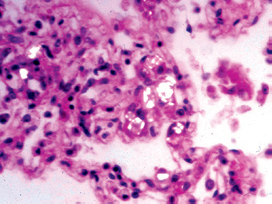
Starch. Brightly birefringent starch particles with central “Maltese cross,” within a poorly formed alveolar septal granuloma (polarized light; H&E, x400).
Microcrystalline cellulose (MCC) is a partially depolymerized, fiber-like form of cellulose that is produced by acid hydrolysis of α-purified wood cellulose (25). MCC fibers are rod-shaped or “matchstick-like” structures that measure from 20 to 200 μm in length (
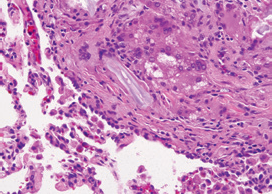
Microcrystalline cellulose. Large gray fibers with foreign body giant cell reaction within an obliterated pulmonary artery (H&E, x400).
Microcrystalline cellulose. Bright birefringence of broad, “matchstick-like” cellulose fibers (polarized light, H&E, x400).
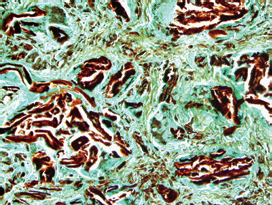
Microcrystalline cellulose. Intense brown-black staining with Gomori methenamine silver (GMS, x200).
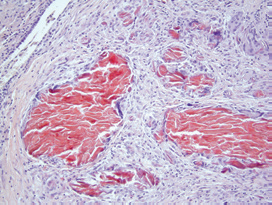
Microcrystalline cellulose. Orange staining with Congo red (x200).
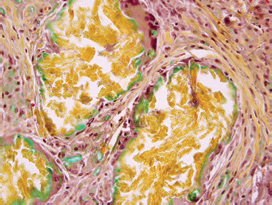
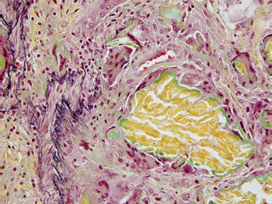
Microcrystalline cellulose. Yellow staining with Movat pentachrome (x400). Peripheral green tint is a common artifact.
Crospovidone, a polymer of vinyl-2-pyrrolidone, is a non-birefringent, irregular, convoluted corallike structure measuring ≤100 μm that is deeply basophilic on hematoxylin and eosin staining (
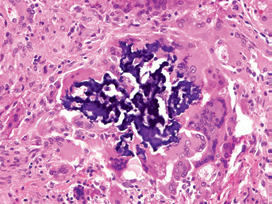
Crospovidone. Deeply basophilic staining and convoluted “coral-like” appearance of crospovidone encased in a foreign body granuloma (H&E, x400).
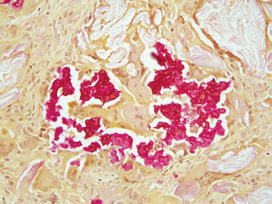
Crospovidone. Brilliant red staining with mucicarmine (x400).
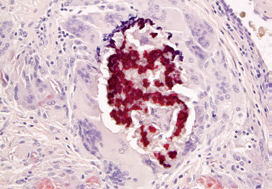
Crospovidone. Deep red-brown staining with Congo red (x400). Note orange microcrystalline cellulose fibers at lower edge of image.
There are numerous other tablet excipients which may potentially embolize to the lung, the majority of which have not been well characterized histologically. Magnesium stearate is described as an irregular rounded particle measuring 5 – 10 μm, and siliciumoxid (silica) has an elongated structure measuring 10–20 μm (2). Both are birefringent without other distinguishing histochemical staining properties. We have recently observed variable amounts of an unidentified myxoid substance or hyalinized material, having variable staining features, associated with micro-crystalline cellulose and crospovidone (
Unidentified hyaline/myxoid material adjacent to microcrystalline cellulose in an intravascular granuloma (H&E, x400).
Unidentified material showing variable staining contrasted with vivid yellow microcrystalline cellulose. Note focal destruction of vascular elastica (Movat pentachrome stain, x200).
Cotton fiber emboli may result from attempts by the user to filter the tablet suspension through gauze or cotton balls. Cotton fibers are birefringent under polarized light and have similar histochemical staining properties as microcrystalline cellulose, but lack the rigid rod-like shape of MCC (5, 24, 28). Cotton fibers, when present, are usually sparse within the lung.
Clinical Features
Pulmonary foreign body embolism and granulomatosis may cause dyspnea, hypoxemia and chest computed tomography (CT) imaging findings of diffuse bilateral micronodules (
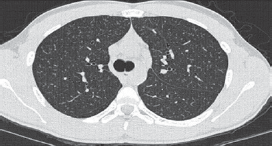
Chest computed tomography (CT) scan showing diffuse bilateral micronodules in a miliary pattern.
Pathologic Features
Angiothrombosis and foreign body granulomatosis represent the major histopathologic reactions to embolized tablet excipients. In heavy users, the lung parenchyma has a macroscopic finely granular appearance with a sandpaper-like texture due to obliterated small vessels (
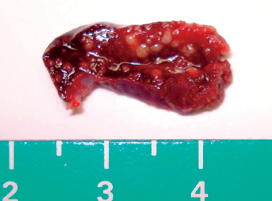
Lung wedge biopsy specimen from patient depicted in Image 15. Tan micronodules present in a background of congested lung parenchyma (scale in cm).
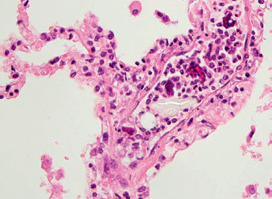
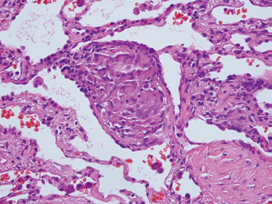
Acute foreign body embolism. Microcrystalline cellulose and crospovidone associated with a neutrophilic response (H&E, x400).
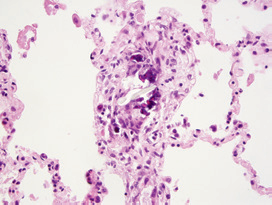
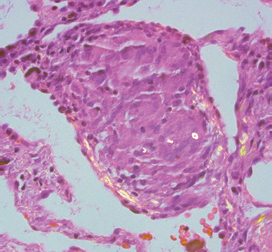
Subacute foreign body embolism. Histiocytic response with early granuloma formation (H&E, x200).
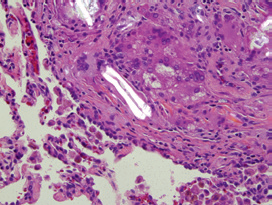
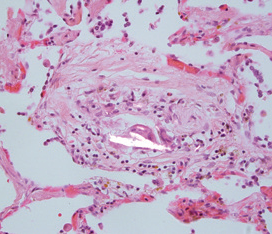
Late-stage foreign body embolism. Well developed microcrystalline cellulose granuloma. Note disruption of vascular wall elastica and extension of granulomatous reaction through the vascular wall (upper left) (Movat pentachrome, x400).
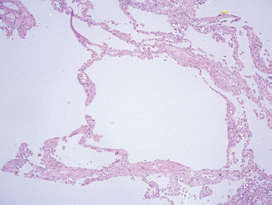
End-stage lesion. Fibrous obliteration of arterial lumens with minimal giant cell reaction to microcrystalline cellulose and crospovidone (H&E, x40).
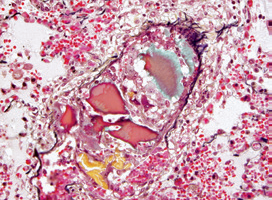
Additionally, endothelial hyperplasia in association with foreign material may give rise to plexiform lesions of severe pulmonary hypertension (
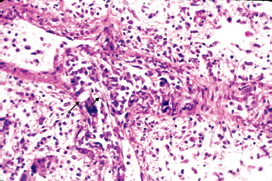
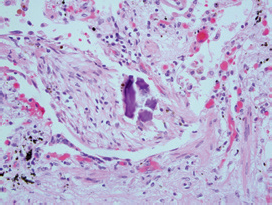
Arterial plexiform lesion. Endothelial hyperplasia and foreign body reaction to crystalline particles (arrows; H&E, x400).
A unique form of emphysema occurs in association with the chronic injection of talc particles. Numerous birefringent particles are associated with small granulomas and perivascular fibrosis in a setting of panacinar emphysema (

Lung with talc-induced panacinar emphysema and mild interstitial fibrosis (scale in centimeters/millimeters).
Talc-induced panacinar emphysema, from specimen depicted in Image 22. Note interstitial talc crystals (partially polarized light; H&E, x40).
A rare parenchymal response to embolized foreign material is progressive massive fibrosis similar to that seen in complicated mineral dust pneumoconiosis (31). Irregular fibrotic mass lesions are associated with lung contraction, volume loss and regional hyperinflation. Histologically, a mixed cellular reaction of macrophages, multinucleated giant cells, lymphocytes and mesenchymal cells are associated with numerous birefringent particles (31).
Differential Diagnosis
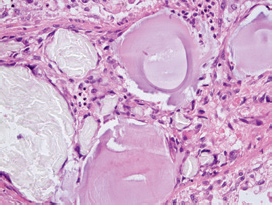
Endogenously formed crystals associated with granulomas in sarcoidosis or other granulomatous disorders can pose a difficult differential diagnosis for foreign body embolization (36, 37). Crystals within sarcoidal non-necrotizing granulomas consist primarily of calcium oxalate and calcium carbonate and are brightly birefringent (38–40). They vary in shape from small ovoid bodies (3–5 μm) to laminated or amorphous crystals up to 20 μm in diameter (
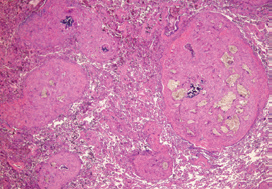
Sarcoidosis. Non-necrotizing epithelioid granuloma within the interstitium (H&E, x200).
Sarcoidosis. Non-necrotizing granuloma containing small birefringent crystals, including ovoid body with central opacity (polarized light; H&E, x400).
Inhaled minerals or other birefringent materials as may occur in the mineral dust pneumoconioses or through snorting drugs such as cocaine can be distinguished from injected materials mainly by their location within airspaces or the interstitium, frequently around small airways, rather than in an angiocentric distribution (41, 42). Inhalational talcosis can be further separated from injectional talcosis by particle size. Injected talc particles tend to be larger (>5 μm in length) than inhaled particles (<5 μm) (43). Inhaled mineral particles, including sheet silicates, may occasionally undergo iron encrustation to form ferruginous bodies (44). To our knowledge, ferruginous body formation is not known to occur with injected tablet filler materials.
Aspiration in drug users can occur from the combination of depressed cough reflex, decreased level of consciousness, and retained bronchial secretions (45). Aspirated tablet fillers can be differentiated from those delivered intravenously by their typical location within bronchioles and alveoli accompanied by intra-alveolar exudate, organizing pneumonia, and a foreign body reaction (
Aspiration pneumonia. Foreign body reaction to microcrystalline cellulose surrounded by a “Masson body” of organizing pneumonia located in alveolar duct lumen (partially polarized light; H&E, x200).
Aspiration pneumonia. Glassy, basophilic, angulated, Kayexalate particles within a “Masson body” residing in a respiratory bronchiole (H&E, x200).
Parenteral nutrition is used for nutritional support for patients having various conditions. While on hyperalimentation, patients have rarely been reported to develop intravascular calcium phosphate crystals (49–52). Calcium phosphate crystals are birefringent and may be confused with microcrystalline cellulose or talc. Patients on hyperalimentation frequently may also have indwelling vascular access ports. A careful examination to exclude IV drug abuse and foreign body embolization should be made in cases of purported fatal crystallized hyperalimentation fluid.
Microanalytic Techniques
In the evaluation of embolized particulates, knowledge of the clinical setting and the drugs which were injected, as well as the histological and histochemical properties of the material may afford a definitive identification of the embolized particles (e.g., crospovidone or microcrystalline cellulose). However, identification of a previously undescribed material or a material having non-specific features will require reliance on micro-analytic techniques. Three useful methodologies for the identification of particles in tissue include transmission or scanning electron microscopy with energy dispersive X-ray analysis (EDXA), infrared spectroscopy, and Raman laser spectroscopy.
The use of electron microscopy with EDXA allows for high definition and identification of particles invisible by light microscopy down to a size range of 0.1 μm in diameter. Bombardment of a particle with an electron beam produces X-rays having energies that are characteristic of the elements which form the particle. The energies emitted are then analyzed with a silicon lithium semiconductor detector and portrayed as a spectrum showing the relative abundance of all elements with anatomic number of 11 (sodium) or greater. Electron microscopy with EDXA is especially useful in defining inorganic particulates or fibers (53). The major limitation of EDXA is its inability to define the full composition of organic compounds.
Infrared spectroscopy is another common technique used by organic and inorganic chemists for the identification of substances (54). This methodology measures the absorption of different infrared frequencies by a sample in the path of an infrared beam. Different functional groups in a material absorb a characteristic frequency of infrared radiation. Infrared absorption may be measured by a Fourier transform spectrometer and a spectra characteristic of the analyte is produced (54). To analyze small forensic samples, infrared microspectroscopy in which the spectrometer is attached to an infrared microscope is utilized. This technique enables the infrared light to be focused on the particle of interest in a 5 μm thick paraffin embedded tissue section using a light microscopic. The infrared spectra obtained are then compared with the spectra of known materials in a spectral library (27). Infrared spectroscopy has been previously used to identify embolized crospovidone, microcrystalline cellulose, and silicone in lung tissue samples (27, 55).
Raman laser spectroscopy is another powerful spectroscopic technique for the identification of organic and inorganic compounds. It is a nondestructive method which requires no sample preparation and can be used to identify materials in paraffin-embedded tissue sections using a light microscope (56, 57). The basic principle entails illumination of the material in question with monochromatic light via a laser beam, and using a spectrometer to examine the light scattered by the sample (Raman spectrum). Every compound has a unique Raman spectrum that can be used for sample identification (58). Raman spectroscopy is a rapidly advancing field in which new forensic and biomedical applications are being discovered (58). Raman spectroscopy has been previously used to identify microcrystalline cellulose in a case of Munchausen syndrome due to tablet injection (59).
Conclusion
Pulmonary foreign body embolism and granulomatosis are the major pathological findings in an injectional user of prescription drugs. Morphology and histochemical staining properties can be used to identify many of the common excipients used in pharmaceutical pill manufacturing. Definitive diagnosis can be made using various analytical techniques when needed. There are many possible mimickers of foreign body embolism and granulomatosis. Recognition of the pathological findings and foreign body properties is important in forensic pathology to establish a correct cause and manner of death.
Footnotes
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest.