
Abstract
Forensic pathologists frequently encounter foreign pigments and fillers in the tissues of intravenous drug users. Titanium dioxide or rutile (derived from rutilus, the Latin term for red) particles are highly stable, poorly soluble, bright white pigments that are widely used in manufacturing, including as a whitening agent in the production of medicines and pharmaceuticals. Humans may be exposed to titanium during its manufacturing or use and the typical routes of documented exposure are inhalational, dermal, and oral (1). Intravenous exposure is also possible, and rare autopsy studies have identified titanium pigment in the tissues of intravenous drug users (2, 3).
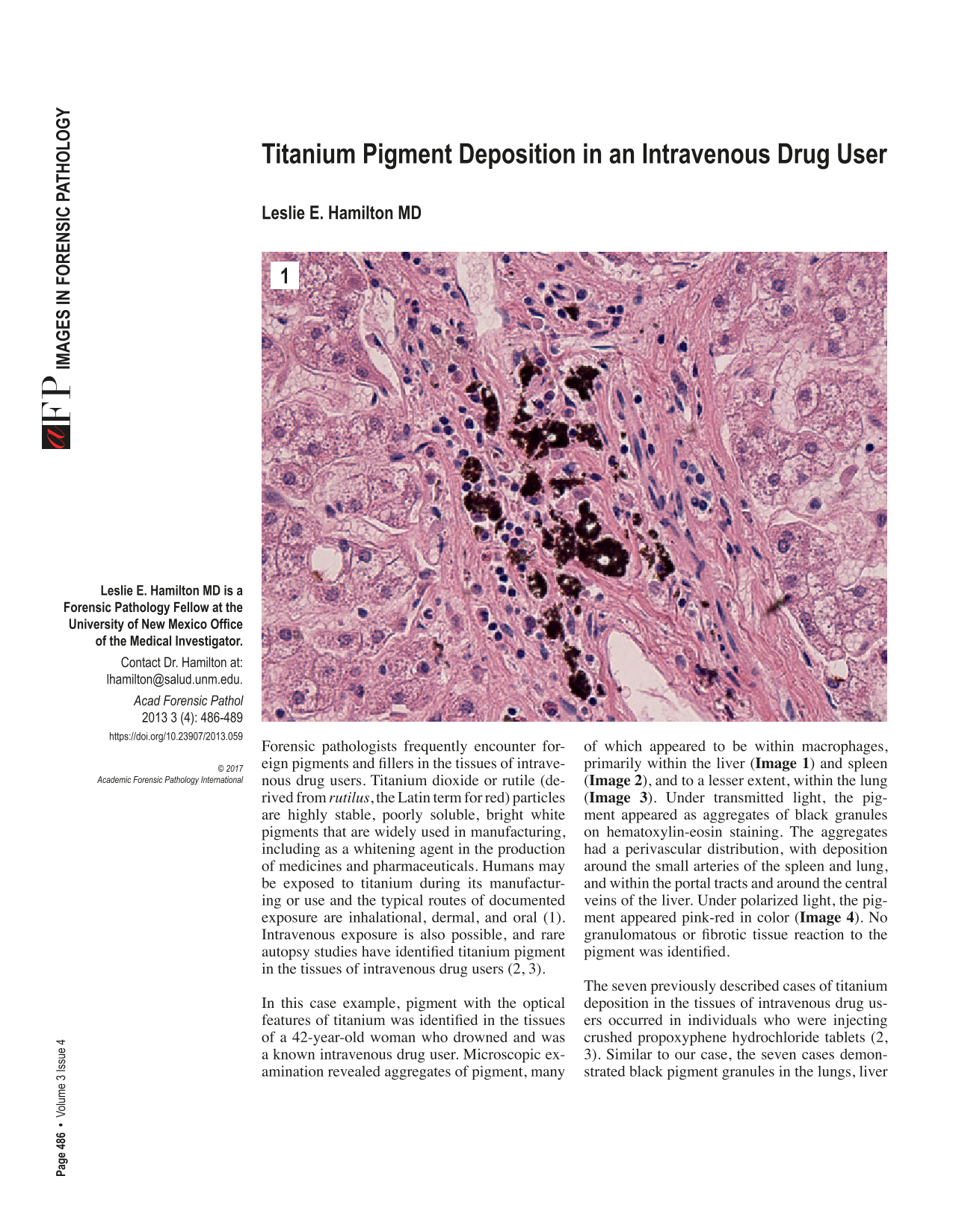
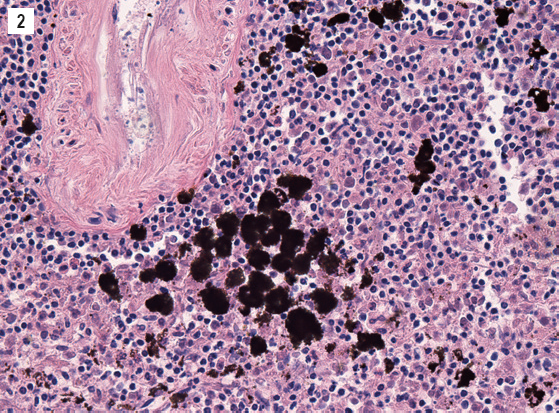
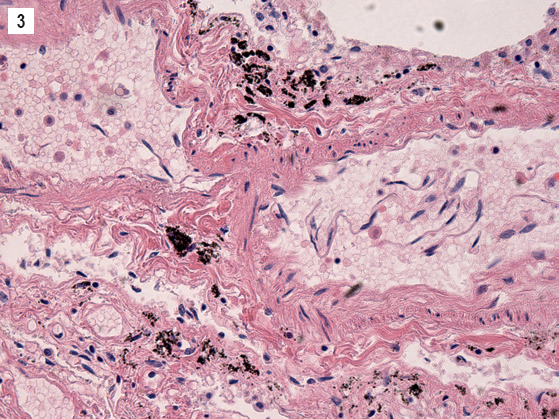
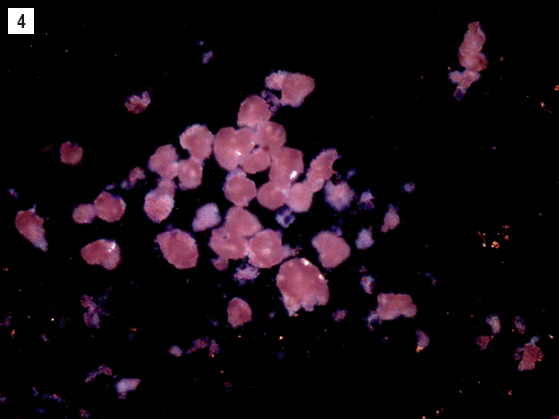
In this case example, pigment with the optical features of titanium was identified in the tissues of a 42-year-old woman who drowned and was a known intravenous drug user. Microscopic examination revealed aggregates of pigment, many of which appeared to be within macrophages, primarily within the liver (

The seven previously described cases of titanium deposition in the tissues of intravenous drug users occurred in individuals who were injecting crushed propoxyphene hydrochloride tablets (2, 3). Similar to our case, the seven cases demonstrated black pigment granules in the lungs, liver and spleen, which appeared pink under polarized light. In addition, titanium pigment also occurred in the lymph nodes and bone marrow. In five of the cases, the pigment was seen macroscopically as chalky streaks and dots (3). In two of the cases, the pigment was confirmed to be titanium by scanning electron microscopy with X-ray energy dispersive spectroscopy (2).
Although historically titanium pigment was thought to be inert, there have been cases of fibrotic, necrotic, xanthomatous and granulomatous reactions to titanium pigment deposition within the lungs, skin and synovium (4, 5). Titanium has also recently been classified by the International Agency for Research on Cancer as a Group 2B carcinogen (possibly carcinogenic to humans) (6), and given its widespread use in manufacturing and in nanomedicine, there is renewed interest in evaluating its toxicity when administered intravenously. Similar to the above described autopsy findings in humans, animal studies have demonstrated titanium accumulation after intravenous injection in the liver, spleen and lungs, with long-term retention in the macrophages of the liver and spleen (7–10). It is thought that the retention occurs due to limited degradation of titanium by macrophages due to its inherent chemical stability (8).
Other potential sources of titanium pigment include joint replacement prostheses, implants in dental and cardiovascular therapy and restorative and plastic surgery (11), and occupational exposure to titanium dioxide dusts (12, 13). Titanium dioxide has long been used in the manufacturing of articulating prosthetic implants (1), and it is well known that wear and corrosion of the implant can lead to widespread dissemination of metal particles to tissues, including the liver, spleen, bone marrow, lymph nodes, and skin (14–16).
The differential diagnosis of black pigment encountered during histopathologic evaluation includes carbon, gold, mercuric sulphide deposits, and artifacts of fixation such as formalin pigment, mercury pigment and osmium dioxide. Although carbon is typically encountered in the lungs and regional lymph nodes within smokers and those living in urban environments, carbon may also be deposited within the lungs, liver, and spleen of coal workers (17). Gold deposits have been described in the mononuclear phagocytes of the liver of individuals treated with gold salts for rheumatoid arthritis (18). Chronic inorganic mercury poisoning from laxative abuse or occupational exposure has also led to the occurrence of black pigments due to the deposition of mercuric sulphide (19). The use of polarizing microscopy is useful to differentiate these pigments from titanium, as carbon and inorganic mercury are non-polarizable, and gold has a golden birefringence.
Although the source of the titanium pigment in this case is not known, it is likely related to intravenous drug use. Forensic pathologists should be aware that titanium dioxide is another source of black pigment in tissues, its pink appearance under polarizing microscopy is characteristic, and its presence can indicate intravenous usage of drugs that contain titanium pigment filler.
Footnotes
The author, reviewers, editors, and publication staff do not report any relevant conflicts of interest.