
Abstract
Deaths due to internal obstructions of the airway (choking) are preventable injuries that are often associated with underlying risk factors including neurologic impairment by disease, intoxication, or very young or old age.
We reviewed 138 decedents with accidental internal obstruction of the airway. Records including autopsy, toxicology, and investigators’ reports were reviewed for a five-year period. There were 138 choking deaths and the age ranged from one to 96 years (mean = 57). Neurologic disease (e.g., remote cerebral vascular events, dementia, developmental disorders) was the most common risk factor for fatal choking (51%), followed by acute alcohol intoxication (13%), psychiatric illness (8%), and young age (8%). In 8% of decedents, there was no identifiable risk factor following investigation, autopsy, and toxicological examinations. The choking episode most commonly occurred in residences (62%), followed by nursing home/long-term care facilities (20%), streets/parks (6%), restaurants/bars (4%), and schools (1%, including one culinary school). Meat was the most commonly identified food object (14%); non-food objects included drug packets.
It is exceedingly rare for a neurologically intact adult to choke to death on a bolus of food without another underlying, identifiable risk factor. For death investigation, it is important to have a high index of suspicion for choking, and one must be careful not to confuse terminal aspiration of gastric contents with a fatal blockage of the airway by a swallowed bolus of food. A risk factor should be sought in each choking death, as it usually is the underlying cause of death.
Introduction
Choking, as defined by internal obstruction of the airway, is the fourth most common cause of unintentional injury mortality in the United States and is most commonly seen at the extremes of age, children younger than four years and the elderly (1). While extensive literature is available on choking deaths in children, there is less information regarding choking deaths in the adult population. Many advances have arisen in the management of airway obstruction, but there is little information with regard to the demographics, predisposing factors, and causes of choking fatalities specific to adults. This may partially be explained by the conventional forensic pathology dogma that it is exceedingly rare for a neurologically intact adult to choke to death on a bolus of food. It is important in death investigation to maintain a high index of suspicion for choking and one must be careful not to confuse terminal aspiration of gastric contents with a fatal blockage of the airway by a swallowed bolus of food. Furthermore, it is important for caregivers to be able to identify individuals at risk for choking to aid in the prevention, diagnosis, and treatment of choking.
In the following study, we reviewed 138 choking deaths during a five-year period with the primary aim to identify risk factors associated with choking in the adult population.
Materials and Methods
The New York City Office of Chief Medical Examiner (NYC OCME) investigates all unexpected, violent, and suspicious deaths in New York City. By statute, these deaths must be reported to the OCME. From medical examiner death certificates and toxicology records between January 1, 2006 and December 31, 2010, we identified 138 decedents whose death involved internal obstruction of the airway (choking). Medical examiners investigated and certified all 138 deaths. Of these, 96 (69%) underwent autopsy examination. The death certification data, toxicology results, and other relevant documents in the OCME file were reviewed for each case by one of the authors (JRG).
Postmortem blood was collected, preserved with sodium fluoride, and stored at 4°C. Toxicological analysis was performed on all decedents by the Forensic Toxicology Laboratory at the OCME. Ethanol concentrations were determined in blood using headspace gas chromatography. Specimens were routinely screened for opioids, barbiturates, amphetamines, benzoylecgonine (BE), and benzodiazepines by enzyme- or radioimmunoassay. Confirmation and quantitation of morphine, codeine, and benzoylecgonine were performed using gas chromatography/mass spectrometry (GC/MS). Urine or blood was also analyzed by gas chromatography for basic drugs, including cocaine, phencyclidine (PCP), and methadone with confirmation by GC/MS.
According to the policies of the New York City Office of Chief Medical Examiner and New York University School of Medicine, this research did not require institutional review board (IRB) approval; however, it was submitted to and approved by the OCME legal office to ensure that it complied with OCME policies and did not require IRB approval.
Results
During the five-year study period, the NYC OCME certified the causes and manners of 40,286 (15%) of the 269,113 deaths that occurred in New York City. Of these, 138 deaths were from choking (0.34%). The age ranged from one to 96 years (mean = 57) and there were 12 decedents younger than 18 years of age (9%). The racial/ethnic breakdown included 71 white (51%), 37 Hispanic (27%), 21 black (15%), and 9 Asian (7%). There were 82 males (59%) and 56 females (41%).
Risk factors for choking (typically the underlying cause of death) are listed in
Risk Factors/Proximate Cause of Death for Choking Fatalities
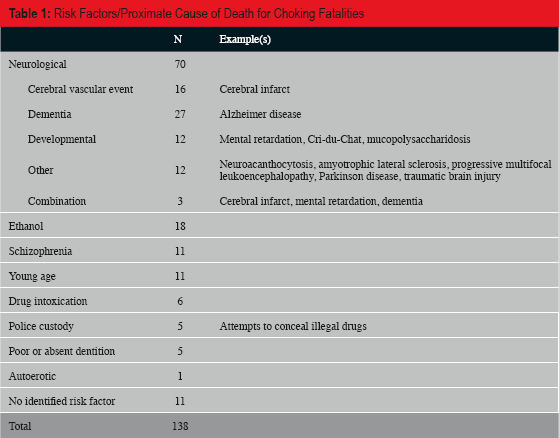
The location of the onset of choking included: 86 residences (62%), 28 nursing home/long-term care facilities (20%), nine streets/parks (6%), six restaurants/bars (4%), and two schools (1%, including one culinary school). In 113 instances, the choking episode occurred in the presence of another person (82%). The choking episode, however, was not always recognized by the other person. In some instances, the victim left the room or went to the bathroom. Of the 136 deaths in which the initial circumstances were known, there were 15 instances in which the pathologist was the first to diagnose choking; of these, eight were alone during the choking episode. In 24 other instances, the choking was first detected by emergency medical services (EMS) or in the emergency department when intubation was attempted in an unresponsive person (17%). One person managed to call 911 and somehow communicate the choking episode while another person wrote a note to a friend indicating that he was choking.
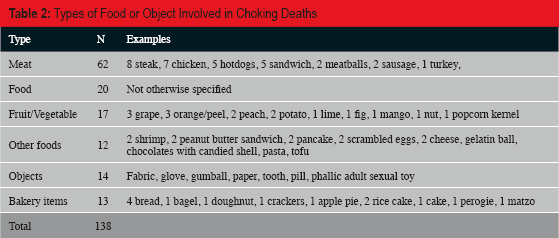
The types of food/objects involved are listed in

Plastic bag with cocaine lodged in trachea.
Types of Food or Object Involved in Choking Deaths
Discussion
An underlying risk factor was identified in 92% (127/138) of decedents who asphyxiated due to choking. Neurological impairment was the most common risk factor identified associated with choking deaths (51%), followed by ethanol intoxication (13%). Similar findings have been reported by others (1–3). Dolkas et al. reported ethanol or sedative drug use in 14% of choking deaths, and a neurological deficit or anatomic difficulty (i.e., laryngeal cancer) in 55% of cases (1). Swallowing requires neurologic coordination to move food through the oral, pharyngeal, and esophageal phases and to protect the airway in the process. Dysphagia can result from a wide variety of neurologic disorders (4). Ethanol has been shown to increase the natural pharyngeal threshold for triggering protective swallowing reflexes (5), making an intoxicated person more vulnerable to choking or aspiration. One of the earliest studies on choking deaths by Mittleman et al. stratified their analysis into institutionalized vs. free-roaming adults, and found that ethanol was implicated in 74% of the free-roaming adult group, although in subsequent studies this number has not been quite as high (2).
Young age and schizophrenia each accounted for 8% of the deaths. Vulnerability to choking in the otherwise healthy pediatric population is well documented and has been attributed to incomplete mastication preceding eruption of molars (<2 years of age), ineffective chewing and swallowing, and a propensity to distraction while eating (6). Likewise, choking in a person manifesting some psychiatric illnesses may be attributed to gulping food or inattentiveness during food consumption associated with temporary cognitive impairment. The use of sedatives was implicated as the underlying cause of the choking in only one death in this study, and the medication was administered to treat a psychiatric condition. While the use of sedative-hypnotics for both medical and recreational purposes has been reported with slightly higher frequencies in other studies and should certainly be considered an independent risk factor for choking, ethanol appears to be a much stronger risk factor for choking than sedating drugs (2, 7).
Inadequate dentition was listed on the death certificate as the underlying cause of choking or a significant contributing factor in 11.6% (16/138) of cases and was the only identified risk factor for choking in five deaths. Poor dentition, edentulousness, and defective or partial dentition has been previously linked with an increased risk for choking and shown to correlate with advanced age (8, 9). In one study of choking deaths, intact dentition described as “close alignment with a minimum of 24 teeth” was found in only 10% of decedents who died after choking (9), and all of the edentulous individuals in that study choked on semisolid food.
Private residences were the most common location in which the choking event occurred (62%), followed by nursing homes or long-term care facilities (20%). The event occurred in a restaurant or bar in only 4% of cases. In 1982, Mittleman et al. reported that 34% of choking deaths in non-institutionalized adults occurred in restaurants (2). Dolkas et al. (1997) reported that 14% of adult choking deaths occurred in restaurants, and noted that intervention measures in restaurants (i.e., Heimlich, 911 calls) were inadequate compared to other locations (1). The relatively few number of restaurant-related choking deaths observed in this study may reflect improved education of restaurant employees and general public awareness of appropriate intervention strategies for choking, although this study did not investigate these specific parameters.
Meat has consistently been reported as the most common food type identified in choking deaths, and the same holds true in this study. Meat was implicated in 14% of deaths with a variety of other food substances identified in much fewer numbers. While meat has been the most common food implicated in choking deaths in neurologically intact individuals, institutionalized persons with neurological impairment are at risk for choking with a wider variety of food substances (2).
Non-food foreign objects were the source of obstruction in 10% of the deaths. Of these, atypical events surrounding the death were implicated as the sole reason for ingestion of the foreign objects in 6/14 (43%). In five deaths, the decedent was being taken into police custody and choked while attempting to swallow and conceal one or more packets of illicit drugs. In another death, the airway was obstructed by a phallic object during an autoerotic asphyxia exercise.
There were only 11 deaths (8%) due to choking on food in which a risk factor could not be identified. Six of these deaths, however, were delayed deaths (greater than 12 hours of survival) and/or did not have toxicology performed. Due to prolonged survival times and the absence of toxicological analyses, the number of drug or alcohol-related choking deaths may be underestimated. For example, one decedent choked on corned beef in an Irish pub during St. Patrick's Day. Since he had a prolonged survival and toxicology was not performed, one cannot exclude the possibility that alcohol intoxication was a contributing factor.
Death investigators and medical personnel must be aware of the common mimickers of choking, such as terminal aspiration and aspiration pneumonia/pneumonitis, as well as diagnostic pitfalls (i.e., the café coronary syndrome). As previously stated, choking is defined as internal obstruction of the airway and should be differentiated from aspiration of gastric contents or foreign debris into the lower pulmonary airways. A common misinterpretation, particularly with first responders, is to confuse terminal aspiration with choking as the cause of death. Forensic pathologists commonly detect partially digested gastric contents in the esophagus, mouth, and airway of decedents who die from a wide range of disease and trauma. After death, with relaxation of muscles, gastric contents will travel where there is the least resistance. In many instances, particularly if the stomach is distended by its contents, fluid and/or partially digested gastric contents will track up the esophagus to the airway. With attempts at resuscitation (e.g., ventilation of the patient), these contents may be forced farther in the lungs. With this caveat in mind, acute or chronic aspiration of gastric contents or other substances may still result in death, but such deaths would not be attributed to choking.
Aspiration pneumonia may also be a complication of neurologically impaired individuals who are unable to “protect” their airway. Certain neurologic diseases or injuries as well as the use of sedative medicines place a person at risk for acute and chronic aspiration. Choking manifests as an impacted bolus of food/object in the airway that originated directly from the mouth as opposed to partially digested food from the stomach or oral secretions that are aspirated. In the latter instance, one would not expect a sudden death due to respiratory failure. Aspiration typically causes pneumonia or diffuse alveolar damage that may result in death over an extended period of time. This is in marked contrast to the sudden incapacitation associated with an acute occlusion of the airway by a bolus of food. Interestingly, while neurological impairment is a strong risk factor for both choking deaths and aspiration, the presence of aspiration itself is not considered an independent risk factor for death by choking (10).
Medical examiners and coroners, as well as their investigators, should maintain a high index of suspicion for choking deaths to prevent misdiagnoses. This is particularly true in instances in which the decedent has a history of advanced medical disease (e.g., coronary artery disease) and in those whose death was not witnessed. While witnessed choking symptoms preceding the death are the best indicator, any sudden death that occurs during a meal or a body found in close proximity to food should raise suspicion. Some choking victim may attempt to go to the bathroom to avoid the embarrassment of choking up a piece of meat, especially if they are in public places. If there is a suspicion of choking, an autopsy provides diagnostic certainty unless the airway has been manipulated by emergency responders. It is often necessary to question medical personnel about foreign objects observed and/or removed from the airway during resuscitative attempts. It may be particularly useful to speak directly with the first responders and witnesses instead of relying upon secondary sources of information. Removal and opening of the larynx and trachea followed by inspection of the oropharynx may diagnose or exclude an obstruction.
The manner of death in choking incidents also should be considered. In general, an inadvertent acute occlusion of the airway by food or a foreign object is certified as an accident. If the object is placed by another, the manner may be homicide. For instances of bronchopneumonia due to aspiration of gastric contents or oral secretion, the manner of death will be dictated by the underlying cause of the aspiration. For example, the manner would be natural in a patient with an aspiration bronchopneumonia due to amyotrophic lateral sclerosis. If the underlying neurologic impairment was caused by a remote injury such as a blunt impact of the head, the manner would depend upon the circumstances of the initial injury. Aspiration complicating anesthesia during elective surgery for a disease may be certified as a therapeutic complication (11).
The Heimlich maneuver is a well-established method to dislodge an airway obstructed by food or an object (12). A variation may be accomplished by a solitary choking person by using the back of a chair to cause the abdominal compression (13). The Heimlich maneuver has been shown to save lives (9); however, it also carries a risk of injury (10). We detected one decedent who died from complications of a laceration of the gastroesophageal junction following the Heimlich maneuver. Given that millions of people have had the Heimlich maneuver performed on them, one fatal complication over a five-year period is not unexpected. In addition, when balancing the risks, failure to remove a bolus of food lodged in the airway has a mortality rate approaching 100%.
Deaths due to internal obstructions of the airway by food (choking) are most commonly associated with an underlying condition without which the choking would have been unlikely to occur. The death investigation and postmortem examination should attempt to identify conditions that affect chewing, swallowing, gag reflex, or attention. These include diseases causing neurologic/cognitive impairment or intoxication. Since a competent cause of death includes the proximate (underlying) cause, defined as that which in a natural and continuous sequence, unbroken by any efficient intervening cause, produces the fatality and without which the end result would not occur, the underlying condition(s) that predispose(s) a person to choke on food should be included on the death certificate as the proximate cause(s) of death or contributing condition(s) when appropriate.
Footnotes
This work was presented at the 2013 Annual Meeting of the National Association of Medical Examiners. The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest.