
Abstract
The National Association of Medical Examiners convened a panel to create a position paper for recommendations for the investigation of infant deaths due to inflicted head trauma. The correct certification of both the cause and manner of death is dependent upon an evaluation of all available data including information derived from the investigation, scene, postmortem examination, and ancillary studies. This paper provides recommendations for the forensic pathologist on what constitutes the dataset to be produced during the postmortem examination of infants who have died of, or have apparently died of, inflicted head trauma. Specifically, this paper describes 1) procedures, 2) ancillary laboratory tests, and 3) forms of documentation that are important in the investigation of these deaths. The evaluation and documentation of such infant deaths involves the production of a detail oriented and thoroughly documented examination that is independently reviewable to support the multitude of inquiries that may follow from the public and the criminal justice system.
Introduction
The National Association of Medical Examiners (NAME) was founded with “the dual purposes of fostering the professional growth of physician death investigators and disseminating the professional and technical information vital to the continuing improvement of the medical investigation of violent, suspicious and unusual deaths” (1). One method of fulfilling this mission is the publication of autopsy standards and position papers (2–5). NAME has previously published position papers on recommendations for the investigation and certification of cocaine, heat-related, and opioid deaths (3–5).
Fatalities due to traumatic brain injury (TBI) among infants/young children, particularly homicides, are among the most challenging investigations for a forensic pathologist for many reasons: any death in this age group may elicit passionate responses even by trained professionals, the decedent may have been seen recently by a physician, a caregiver may be the perpetrator, and the wrong diagnosis may result in a wrongful prosecution, dissolution of families, and putting other children at risk. As such, NAME convened a panel to generate recommendations for the investigation of these deaths. Complementary to a thorough death investigation, the goal of the autopsy is not only to aid in the determination of the cause and manner of death, but also to produce an independently reviewable dataset that allows the original forensic pathologist (and others who follow) the best opportunity to review primary data and potentially answer unanticipated future questions. As Moritz stated, “If a negative or positive postmortem finding is so important that it may make the difference between the freedom or imprisonment, or the life and death of someone, every attempt should be made to protect, preserve, and record it for others to see and evaluate” (6).
Autopsy protocols have been developed for cardiac, metabolic, and sudden infant deaths (7–13) to ensure consistency and comprehensive examinations that look for a broad range of diseases. Similarly, this paper's aim is to describe an autopsy protocol to facilitate a thorough, independently reviewable investigation of pediatric head injury deaths. NAME has already published general autopsy standards that are applicable to infants/children with apparent head trauma. This traumatic brain injury protocol is not meant to replace those preexisting standards but to provide detailed techniques, procedures, and other recommendations for these investigations. Each case is unique, and this protocol is not meant as a substitute for professional judgment. The following protocol, however, may be considered practice recommendations for these investigations endorsed by the NAME Board of Directors.
Infants die suddenly and unexpectedly for a myriad of reasons that span the spectrum from natural disease to inflicted injury. Infant/childhood deaths due to TBI may have no history or external evidence of trauma; therefore, unexpected and unexplained infant/childhood deaths are thoroughly evaluated at the outset as they may be homicides or due to rare natural disease. As such, these deaths undergo a uniformly thorough investigation and documentation through the initial stages of the evaluation, documentation, and evisceration. As pathologic findings emerge during the course of the examination and prosection, the necessity and/or utility of ancillary dissections and studies will become apparent, and their selection can be tailored by the forensic pathologist.
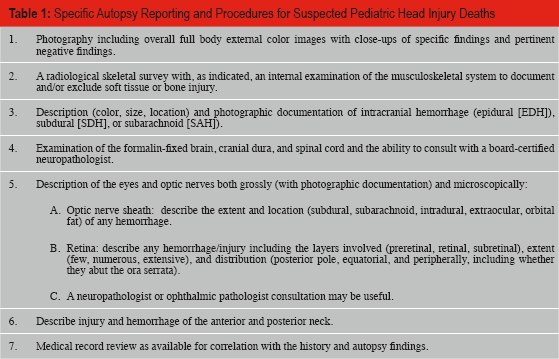
The subsequent protocol describes a progression of relevant examinations and processes for the thorough description and documentation of pertinent findings (
Specific Autopsy Reporting and Procedures for Suspected Pediatric Head Injury Deaths
Discussion
Initial Autopsy Investigation
The initial autopsy investigation includes digital photography and full body radiologic imaging performed prior to the internal examination.
Digital Photography
Integral to the development of a dataset that facilitates independent case review is high quality, color photography. Unlike film photography, digital imaging allows the prosector to know immediately if the image is properly captured (14). Therefore, digital photography is the preferred method for photographic documentation for these investigations. A core list of recommended photographs is included in
Core Photographs to be Obtained in Cases with Head Trauma or Suspected Head Trauma *
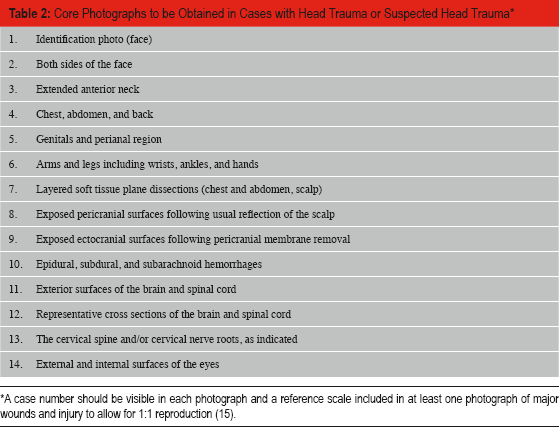
A case number should be visible in each photograph and a reference scale included in at least one photograph of major wounds and injury to allow for 1: 1 reproduction (15).
Plain Film Radiography
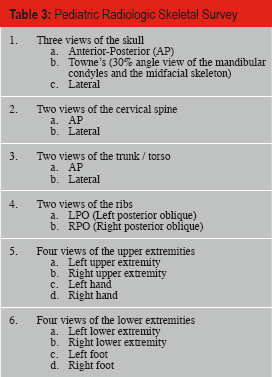
As skeletal injury may not be detected during a standard autopsy, healed and healing fractures may be missed (16). Therefore, full body radiographs, which may aid in the detection of these lesions, are indicated when investigating a death with potential inflicted trauma. A radiologic skeletal survey is necessary for the evaluation of unexplained infant/childhood deaths that come to the attention of the medical examiner/coroner (ME/C) (16,17). A pediatric skeletal survey protocol is provided in
Pediatric Radiologic Skeletal Survey
Advanced Radiologic Techniques
Postmortem computed tomography (CT) and magnetic resonance imaging (MRI) offer the ability to provide unobstructed and three-dimensional visualization of body lesions. Some offices have in-house scanners or have arranged access with local hospitals. While these procedures likely provide superior results for certain injuries over plain films, at the current time, the strengths and weaknesses of each modality have yet to be fully defined in the forensic autopsy setting. In addition, plain film radiographs continue to be the choice for the clinical evaluation for most fractures in children. The use of CT/MRI remains at the discretion of the forensic pathologist and subject to the availability of facilities and funding for such modalities (18). While postmortem CT/MRI currently may be a useful adjunct, the external and internal autopsy examination remains the best method for the postmortem diagnosis of injury (19). Since some infants or children who ultimately die from injuries may have a survival period in the hospital, antemortem advanced imaging often has been obtained. Admission imaging and other hospital CT and MR scans may provide valuable information and should be sought and reviewed.
External and Internal Examination
Depending on the age of the infant/young child, certain body measurements (e.g., head circumference) in addition to length and weight may be useful. A search for trace evidence and sexual assault evidence collection, if indicated, is done prior to washing the body to better visualize injuries. An external and internal examination is performed per the NAME Forensic Autopsy Performance Standards which also are followed when describing an injury (e.g., type, location size, shape, pattern) (15).
Specialized Autopsy Investigations When Suspicious Findings are Encountered
As the autopsy progresses, findings suspicious for inflicted traumatic brain injury (iTBI) may be detected. If so, the following specific examinations and documentation of particular findings are recommended. These are described by body region.
Head
Scalp/subscalpular: the number, location, and size of scalpular and subscalpular hemorrhages are best documented through a combination of the photograph(s) and narrative description(s). Correlation should be made between sites of hemorrhage and medical intervention (i.e., prior surgery). Other discrete areas of hemorrhage may occur, such as along cranial sutures from diastasis due to marked brain swelling. The documentation should convey the information necessary for users of the autopsy report to determine when hemorrhage is either due to a secondary process or a direct result of trauma. If there is concern for facial injury not apparent externally, a formal face dissection is possible (20). Detection of otherwise unknown or underappreciated impact sites of the face may change the context of the infant death from one of non-impact to one with demonstrable impact. Intraoral examinations may reveal frenulum, inner cheek, and tongue injuries. Shaving of hair allows for better evaluation and documentation of scalp injuries. Careful examination of the ears includes looking inside and behind the ears.
Skull: documentation of the location, dimension, type (e.g., linear, depressed, comminuted, diastatic) of fracture(s) is achieved through the narrative report, digital photography, and radiologic images; some forensic pathologists may choose to supplement their reports with diagrams. Skull fractures may be subtle in the young pediatric population and therefore removal of the pericranial membranous soft tissues along with the cranial dura allow them to be better identified and examined in detail. Microscopic sections help confirm and document gross findings and may be useful for assessment of the stage of healing.
Hemorrhage: the type [epidural (EDH), subdural (SDH), or subarachnoid (SAH)], location, size, color, and adherence are documented through appropriate use of narrative description and digital photography. The size of SDH and EDH, for example, may be documented by volume, weight, or three-dimensional measurements. The effects of the hemorrhage on the brain (e.g., compression, herniation, shift) are noted in the autopsy report. Microscopic sections help confirm and document gross findings and may be useful for assessment of the stage of healing (21,22).
Brain: for optimal results, the brain and cranial dura should be fixed in formalin (usually for a minimum of 10–14 days). Forensic pathologists are trained to diagnose and describe traumatic brain injuries. As some neuropathologic diseases may be subtle or mimic trauma, consultation with a board-certified neuropathologist may be warranted. Express mail delivery services, gross photography, tissue retention, and microscopic slides allow for consultation even after the initial brain dissection. Pertinent positive and negative gross and microscopic findings include: hypoxia-ischemia, contusion, contusion hematomas, diffuse axonal injury, presence/absence of brain swelling and herniation (type and extent), intracerebral hemorrhage (location and extent), vascular malformations, congenital anomalies, and other focal lesions. Examination of the cerebral dura includes description of any pathology (e.g., subdural blood, surgical defects) and evaluation (opening) of the sinuses (e.g., thrombosis). Microscopic examination of the dural sinus may help distinguish thrombus from postmortem congealed blood.
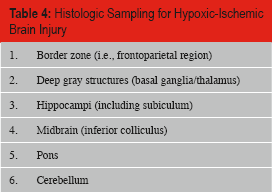
Microscopic sections for suspected inflicted traumatic brain injury include evaluations of pathology identified grossly and sampling that allows assessment of possible natural disease processes, hypoxic-ischemic brain injury, and traumatic axonal injury. Hypoxic-ischemic brain injury in infants/children has a characteristic distribution of injury, and those regions should be included in the evaluation in addition to regions typically involved in adults. A list of locations for histologic sampling is included in
Histologic Sampling for Hypoxic-Ischemic Brain Injury
Histologic Sampling for Diffuse Traumatic Axonal Injury (dTAI)
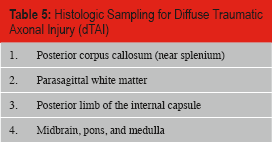
Histologic evaluation of the cerebral dura is useful to assess gross pathology and evaluate for more subtle processes. Evaluation for intracellular iron deposition may facilitate assessment of the stage of healing in SDH and EDH. The interface between sub/epidural blood and ongoing tissue healing is the best site for histologic evaluation. Although there are criteria for the stages of healing of a SDH, many variables affect this process (e.g., size of hematoma, source of blood, age of the individual), resulting in a somewhat predictable but potentially variable course (22). Retention of representative cortical regions, deep gray structures, brainstem, and cerebellum may prove useful. In addition, samples from contralateral white matter regions (e.g., parasagittal white, posterior limb of internal capsule) may be necessary to diagnose or exclude dTAI.
Spinal cord: the spinal cord is examined at all three levels (cervical, thoracic, and lumbar). Some have recommended removal of the brain with the spinal cord still attached (26), but it is unclear if this technically difficult dissection yields any diagnostic value.
Ocular examination: monocular indirect ophthalmoscopy is a noninvasive and nondestructive technique to view the retina prior to autopsy and the equipment is less expensive than that needed for ophthalmic endoscopy (27), however, it does require additional equipment and training. A gross dissection and microscopic examination of the eyes also is possible at autopsy. The interpretation of retinal hemorrhages is beyond the scope of this paper. Forensic pathologists, however, have a duty not only to diagnose and interpret, but also to document and preserve findings. As an autopsy is often the best and sometimes only chance to diagnose, confirm, or exclude certain findings, pathologists, as the independent documenters of facts, are best to err on the side of documentation. A recent prospective clinical study indicated that the assessment of retinal hemorrhages may be useful as a predictor of iTBI (28). Pending the publication of additional research, at a minimum, the ocular examination serves as a quality assurance measure that may confirm or refute clinically diagnosed retinal hemorrhages. Therefore, the removal and examination of the eyes in instances of inflicted or suspected-inflicted traumatic brain injury is recommended.
A technique for removal and examination of the eyes has previously been published (29). After removal, the eyes and periocular soft tissues are fixed in formalin prior to microscopic examination. For optic nerve sheath hemorrhage, the location (subdural, subarachnoid, intradural, extraocular, orbital fat) is documented in the autopsy report. For retinal hemorrhages, the involved layers (preretinal, retinal, subretinal), extent (few, numerous, extensive), and distribution (posterior pole, equatorial, and peripherally, including whether they abut the ora serrata) are described. Special stains, such as Prussian blue to identify hemosiderin, may be useful in some instances. Collection of vitreous will disturb the retina and should be postponed until adequate examination of the retina, the optic nerve, and brain is done and the value of the vitreous analysis for the specific case is considered. Photography with appropriate lighting can aid in the documentation of ocular findings.
Neck
Infants and children who die of inflicted injuries may have injuries of the anterior and posterior neck. In addition to the standard anterior neck dissection, a posterior neck dissection also may reveal internal injury. Injuries of the neck have been proposed to explain potential mechanisms of death and techniques have been described for the examination of the anterior and posterior neck intrinsic spine structures/nerve roots (30–37). If the prosector is concerned for intrinsic structural spinal/nerve root injury, then these structures may be evaluated by various methods. One method is an en bloc dissection of the cervical osseous and neural structures with formalin fixation (37). Another is an in situ method that removes the spinal cord and attached ganglia without the surrounding bone and soft tissues (38). In this technique, the laminae are cut and the spinous processes removed. The lateral aspects of the neural arches are then removed by cutting the articulating facets and pedicles of the vertebrae. The freed sections of bone are removed and the spinal cord is removed with the ganglia attached.
Trunk and Upper and Lower Extremities
The NAME autopsy performance standards include procedures and descriptions for trunk injuries. A subcutaneous examination of the arms, legs, and back and buttocks may improve detection of occult subcutaneous and deep hemorrhage (39).
Of particular importance in pediatric iTBI are the identification and description of rib and other skeletal fractures. In addition to radiographs, an in situ skeletal examination may be useful to further document or exclude injury. An in situ examination may include exposure of the shaft and epiphyseal cartilages of the ribs, clavicles, long bones, and scapulae (40). Traumatized or abnormal structures may be removed for additional analysis including gross (i.e., dry bone) or histologic examination (41–43). When possible, a description of the stage of healing (i.e., bone callus formation) is included in the autopsy report. Forensic pathologists are trained to examine plain film radiographs and bones. As some osseous findings may be unusual normal anatomic variants, consulting with a board-certified forensic anthropologist may be useful. Other useful techniques and examinations include: stripping the parietal pleural lining to better visualize rib fractures, resecting the spinal column with the medial ribs for further evaluation for posterior rib fractures, and histologic sections of cutaneous/subcutaneous injuries (Prussian blue can identify hemosiderin).
Ancillary Studies
Depending upon the circumstances and autopsy findings, ancillary studies for infectious (e.g., viral, bacterial cultures), hereditary, metabolic, or thrombophilic diseases may be indicated.
Records
Review of the medical records including antemortem CT/MRI reports should be done as they may provide relevant clinical information. Review of reports generated by other agencies such as child protective services and law enforcement investigation findings also may guide the forensic pathologist's investigation and therefore these should be requested.
Conclusion
The investigative value of each of the described studies is often unknown at the onset of the autopsy. Many procedures performed during an autopsy create irreversible changes to tissues and thus proactive documentation is critical. Ultimately, the forensic pathologist must use medical judgment on how to conduct each autopsy examination but would be wise to heed the admonition that “I would rather explain why I did an examination than why I did not.” In these instances, it may be stated that the examination was done in accordance with recommendations endorsed by the Board of Directors of the National Association of Medical Examiners.
Footnotes
The opinions and conclusions of this paper have been reviewed and approved by the National Association of Medical Examiners Board of Directors and as such are endorsed by NAME. These opinions and positions are based on a consensus of the current literature, knowledge, and prevailing theories on this topic. As Scientific knowledge and experience grow, NAME reserves the right to revise or update these opinions. The process by which NAME position papers are initiated, written, reviewed, and approved is publically available at ![]() . All scientific position papers endorsed by the National Association of Medical Examiners automatically expire five years after publication unless reaffirmed, revised, or retired at or before that time. This work is a product of NAME and as such, was not subjected to Academic Forensic Pathology Journal editorial review.
. All scientific position papers endorsed by the National Association of Medical Examiners automatically expire five years after publication unless reaffirmed, revised, or retired at or before that time. This work is a product of NAME and as such, was not subjected to Academic Forensic Pathology Journal editorial review.
The editors and publication staff do not report any relevant conflicts of interest.