
Abstract
The maltreatment of elders aged 60 years and older is a worldwide problem with an increasing frequency. Individuals are living longer, resulting in a larger elder segment of populations. Furthermore, as medicolegal investigative and epidemiologic research progresses, more cases are recognized and reported. Elders are a vulnerable population not only because of advanced age and acquired diseases and frailty, but also because of a lack of education in the realm of overall elder healthcare and pathophysiology. Therefore, when investigating an elder death, the challenge is even greater as the medicolegal death investigator and forensic pathologist/medical examiner attempt to separate normal or expected findings from maltreatment. A methodical approach starting with the initial death and scene investigation, followed by a complete elder autopsy and concluding with an organized elder death review, will allow proper classification of cause and manner of death as well of prevention of future cases of elder maltreatment.
Keywords
Introduction
Depending on the medical, scientific, and epidemiological sources as well as geographic location, an elder is an individual 60 or 65 years of age and older. The nation's 65-and-older population is projected to double in size (1) and comprise 20% of the total U.S. population by 2050 (2). As this segment of the population increases, the medicolegal community needs to ensure that complete and thorough elder death investigations are conducted in order to detect deaths resulting from unnatural causes.
The vast majority of deaths occurring in the elderly population are from natural diseases. Natural physiological changes and diseases attributed to aging such as cardiovascular disease, cancer, susceptibility to falls and adverse reactions to medications (3) can cause or lead to conditions that hasten death, such as hip fractures, subdural hematomas, dementia, untreated decubitus ulcers, sepsis, malnourishment, and improper medication. Such conditions may obscure indicators of abuse, neglect, and exploitation. In a younger decedent, these indicators would likely increase the index of suspicion of abuse, resulting in a thorough medicolegal investigation; however, this is not the norm in the elder decedent (4). This article seeks to emphasize the need for complete and detailed medicolegal death investigations in the elderly.
Discussion
Elder Abuse and Maltreatment
Elder abuse, also known as elder maltreatment, includes physical abuse, psychological abuse, sexual abuse, financial exploitation, and neglect. Research suggests at least one in ten elders experience some type of abuse (5). However, according to the National Center on Elder Abuse, “only one in twenty-three cases will be reported” (6).
Cases of potential elder abuse necessitate a thorough medicolegal death investigation, to include a scene investigation, ancillary studies including toxicology screening, review of medical records, and, when warranted, imaging and autopsy, in order to properly determine the cause and manner of death.
Jurisdiction
Unattended deaths or those occurring outside of a medical facility are typically reported to the medical examiner or coroner. However, medicolegal offices often decline jurisdiction in elder death cases or take a brief report of basic demographic information. Many states allow a non-physician or the primary care physician to sign the death certificate, simply assuming the death is due to the documented medical history, without any type of investigation to determine the circumstances surrounding the death.
Only two states (Arkansas and Missouri) have laws that mandate notifying the medical examiner or coroner upon the death of any resident of a residential care facility, assisted living facility, intermediate care facility, or skilled nursing facility (7, 8) regardless of whether the death was due to natural causes. In 2010, approximately 6% of the population over 65 years of age lived in one of the 18 000 nursing homes in the United States (9). In 2010, 33% of nursing home residents died there (9). As the average age of U.S. citizens increases, the number of deaths occurring in these facilities will likely increase.
A review of mandatory reporting statutes for all states and territories revealed that 18 states require medical examiners to report suspected abuse (CT, FL, GA, Guam, HI, ID, IL, KY, ME, MI, MO, MT, NV, SC, TN and VT), 13 states require coroners to report suspected abuse (AR, GA, HI, IL, KY, MA, MN, MO, MT, NV, OH, SC, and TN), and two states (IL, MN) require persons who perform the duties of medical examiners and coroners to report suspected abuse (IL and MN) (10). This leaves 31 states with no mandatory reporting.
Medicolegal Investigation
The investigation begins with an initial telephone interview by a trained medicolegal death investigator to elicit information and determine the extent of investigation needed. Training and experience of individuals who attend these deaths (i.e., investigate and document the deaths) becomes essential. Accidents and subsequent accidental deaths in the elder population are not uncommon. Elders commit suicide, often with a history of chronic illness or loss of a spouse. From the standpoint of a perpetrator of a homicide, fewer suspicions are raised when the victim is already expected to die. Therefore, it is incumbent upon the medicolegal death investigator to obtain in-depth information to determine that the death was indeed natural.
History
Queries about living conditions, social/medical/financial history, circumstances surrounding recent trauma (such as falls), marks or injuries to the body, care providers, medications, functional and nutritional status, physical appearance of the body, presence and stage of wounds (e.g., decubitus ulcers), and neurological status need to be answered. All medical and resuscitative efforts by first responders should be noted as they can introduce artifacts and/or injuries to the body.
Falls
The incidence of fatal falls in the elderly is increasing at a rate even higher than the growing proportion of older adults in the population (11). As people age, natural physiological changes can occur that increase the risk of falling. Such changes include decreased proprioception, decreased motor strength, and impaired gait. The use of certain medications can alter the elder's mental status, such as antidepressants, sedatives, and hypnotics, and contribute to falling. Within a single year, approximately 30% of people aged 65 years or older and approximately 50% of people aged 80 years or older experience a fall (11). Many of these falls have significant morbidity. Between 38% and 47% of falls in the elderly are eventually fatal (11). Questions and observations by the medicolegal death investigator should include time and date of fall, witnesses to the fall, location of the fall, landing surface, use of throw rugs, and the possibility of striking an intermediary object during the fall (e.g., nearby furniture). Most of these falls are accidental; however, homicidal falls from pushing or tripping can and do occur. Common histories provided for a homicidal fall are medication use and frailty; the same as for accidental falls. The totality of circumstances must be evaluated when conducting elder death investigations.
Medications
Polypharmacy is common in older adults and may play a role in death. At the scene, a complete inventory of medications should be documented along with names of those responsible for administering the medications to the elder. Pharmacy records need to be evaluated and compared with the inventoried medications. Absent medication or medication not administered as directed must be explained. Overmedication is often encountered in maltreatment cases to keep the elder unaware, incapacitated, and thus manageable. Undermedication is also seen when care takers consume or sell the elder's medications.
Investigative reports should be completed in a timely manner and contain detailed descriptions of the incident, witness accounts, medical/social/financial history, person last seeing/in contact with the decedent, and person discovering the body. Often, follow-up information must be obtained from the treating physicians and family members. Adult Protective Services should be notified if elder abuse is suspected.
Standardizing Elder Death Investigations
Properly identifying and decreasing preventable deaths in the elderly cannot be addressed without standard, complete, and accurate collection of data. The sudden unexpected infant death investigation (SUIDI) model serves as an example. A comprehensive data collection form for elder deaths could ensure that information is recorded in a concise, systematic, and thorough manner. Critical data to collect include injuries such as contusions, lacerations, abrasions, burns, and fractures, nutritional status or dehydration not consistent with the reported natural disease, presence and staging of decubitus ulcers, evidence of restraint use, and personal and environmental hygiene (
Scene Investigation
A scene investigation is essential in any suspicious circumstance. The medicolegal death investigator should obtain statements from the last person to see the elder alive as well as the person who discovered the body and the time of discovery. The overall health of the elder should be noted, including any recent complaints and psychiatric history. The exact position the body was discovered should be documented, since first responders often move the body in life saving attempts. Medications should be inventoried and documented. All discrepancies should be documented and any observations by the medicolegal death investigator that may alert the pathologist of red flags. If the reporting party does not have a medical or social history, family members or caregivers should be contacted who can provide this information. Treating physicians may be contacted from the scene to confirm information provided by caregivers.
Photography
Photographs document the scene and body and assist the medical examiner or coroner in visualizing the circumstances. Photographs of the scene should be obtained prior to taking photographs of the body. A wide-angle shot is important as well as many different angles to recreate the scene. Videography of the scene may be provided if needed or required by office policy. Materials introduced to the scene (first responder artifacts) should be explained in the medicolegal death investigator report. All marks or injuries should be photographed with a scale for comparison. It is customary to leave the body intact, without wiping or disrobing the decedent. Further examination will be performed by the forensic pathologist once the body arrives in the morgue
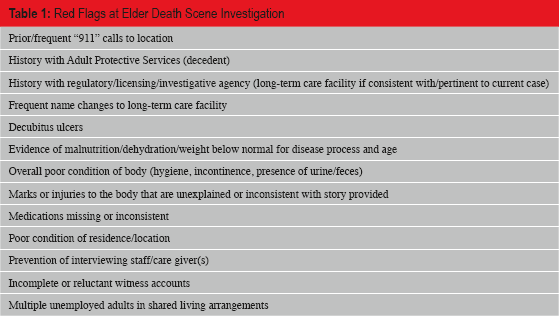
Red Flags at the Scene Investigation
The medicolegal death investigator will typically only respond to an elder death scene that is suspicious, has inconsistent information reported or is due to unnatural death (
Red Flags at Elder Death Scene Investigation
Scene Recreation
The reporting party may not be adept to adequately describe how the elder was found. A scene recreation is an essential part of a thorough medicolegal death investigation and would provide a visual depiction of the position in which the elder was found. Caregivers who have knowledge of the scene should assist in the recreation, but it is critical that the caregiver who found the elder partake in the reenactment so that accurate information is provided. Individuals of the same size and stature would be ideal for the recreation but if not available, a pillow may be used to show the body position at discovery when found. Photographic documentation and descriptions of the position or circumstances are essential. This information will demonstrate the scene to clarify details if the medical examiner or coroner is unable to attend the scene. For example, if an elder is found between the bedrail and mattress, a scene recreation will assist the medical examiner's evaluation, especially if no visible marks or injuries are to the body. The height and material/composition of the bedrail should be measured and all bedding noted. Photographs will depict the exact location of the elder as described by the person discovering the body. If any marks or patterned injuries are identified, documentation of potential implements should be measured and photographed as well.
The Autopsy
The autopsy of the elder decedent begins with a thorough review of the scene investigation, medicolegal death investigator's report, and the medical records. Often the past medical history including psychiatric history is very extensive. However, a summary including organic diseases, disabilities, recent hospitalizations, recent trauma, diet, and medications should be obtained (12–16).
The social history with relevant details regarding the elder's residence, independence, and competency is also important.
Upon arrival to the morgue, the body is examined as well as any photographs depicting the body at the scene. An accurate unclad weight of the body is obtained to correlate with medical records and calculate the body mass index. All positive and pertinent negative findings are photographed. It is important to understand the pathophysiology of aging in order to accurately evaluate findings on the body (12, 17–20).
Normal or Common Changes of Aging
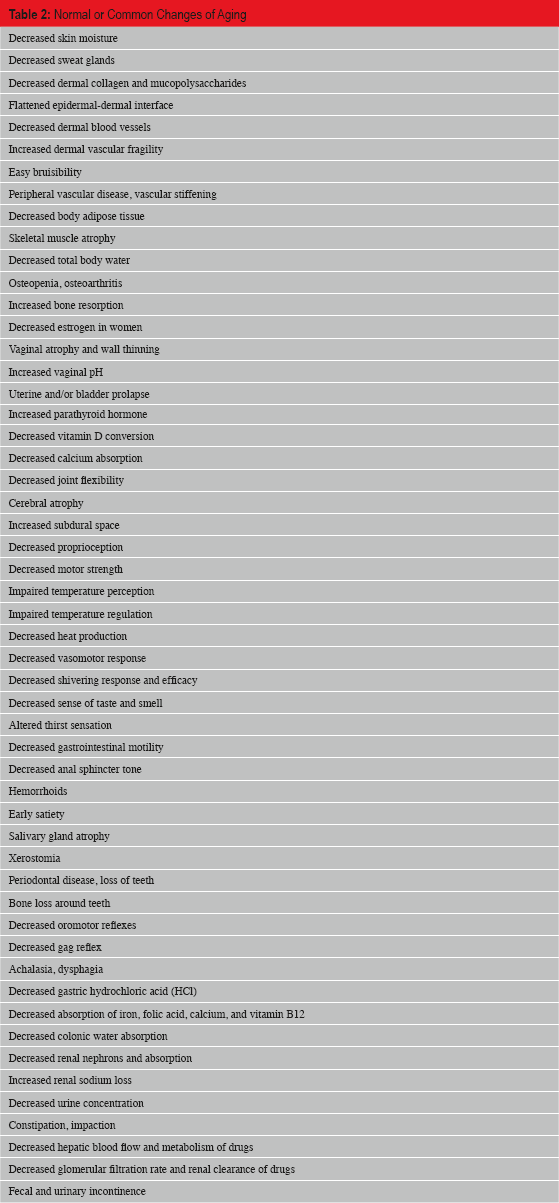
Postmortem radiology can be very useful in not only detecting bony dislocations and acute or poorly healed fractures, but also documenting demineralization and osteomyelitis (14, 15). In cases of suspected maltreatment, a full body skeletal survey is valuable.
Physical and Sexual Abuse
Elder physical abuse is usually in the form of blunt force trauma, especially to the head. Other forms include burns, bites, kicks, traumatic alopecia, and improper restraint use. Numerous injuries, injuries of varying ages, injuries to different areas of the body, and injuries to different planes of the body are especially worrisome for abuse (14, 15). Sections of the injuries can be taken for microscopic examination. The elder may also be a victim of sexual assault with both anogenital and extragenital injuries. A sexual assault examination should be performed on all suspect cases including collection of swabs and preparation of smears from the mouth, anorectal, and genital areas. A saline wet mount can be immediately prepared to assess spermatozoa motility. Swabs should be air-dried for DNA and semen analysis. The smears should be stained with the Papanicolaou stain to look for intact spermatozoa or spermatozoan heads. Blood for a DNA control specimen should be collected in a purple-top vacutainer (ethylenediaminetetraacetic acid [EDTA]) or on an appropriate DNA saver card or filter paper. Spermatozoa, prostatic acid phosphatase, P30 glycoprotein, and DNA can be detected in specimens taken from a female elder victim despite the changes of aging. However, with the barrier of decreased mental status, delayed reporting, defecation, urination, bathing, and/or fear of retribution, the evidence is often lacking (15). A posterior “Y”-incision and extremity cut-downs should be made at the conclusion of the autopsy, especially in those cases suspicious for physical or sexual abuse, to evaluate any occult blunt force trauma.
Physical Findings Suspicious for Physical and Sexual Abuse
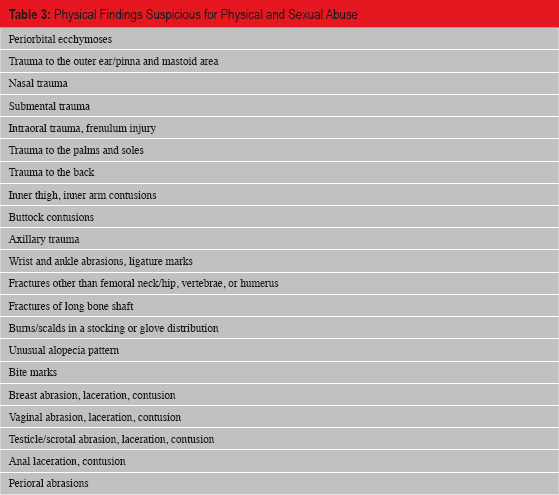
Decubitus Ulcers
One condition that is often associated with and is a red flag for elder maltreatment is the decubitus ulcer, also called pressure ulcer, pressure sore, or bedsore (14, 21). In fact, it has been reported that 95% of neglect victims have decubitus ulcers (14, 21). A decubitus ulcer is a lesion of degenerating skin caused by pressure and decreased circulation resulting in hypoxia and ischemia of the tissues. The pressure pushes the blood out of the soft tissues and prevents the return of the blood supply. The tissues are not only under pressure but are not receiving nutrients from the blood stream. Peripheral vascular stiffening, a natural change of aging, also results in poor perfusion. As a result, tissues breakdown and ulcerate. The skin may break down especially when an elder is bedridden or nonambulatory, lying supine or seated in a wheel chair respectively. Certain diseases can predispose to the formation and poor healing of decubitus ulcers and need to be addressed when correlating the ulcers to a neglect situation. Such diseases include diabetes mellitus, anemia, incontinence, and poor circulation such as peripheral vascular disease.
Many clinicians will grade decubitus ulcers on a scale of 1–4: Grade 1 = non-blanchable erythema without a break in the skin; Grade 2 = superficial epidermal and dermal loss, partial thickness loss no deeper than the dermis, intact subcutaneous tissue; Grade 3 = full thickness involving the subcutaneous tissue; and Grade 4 = ulceration, full thickness with loss of the skin and subcutaneous tissue and exposure of the skeletal muscle, tendon, and/or bone (21).
Sepsis, pneumonia, osteomyelitis, and death can result from decubitus ulcers (14, 15, 21). At autopsy, the blood and lungs should be cultured as well as the decubitus ulcer for correlation. Sections of the ulcer, underlying tissue, and bone should be taken for histology.
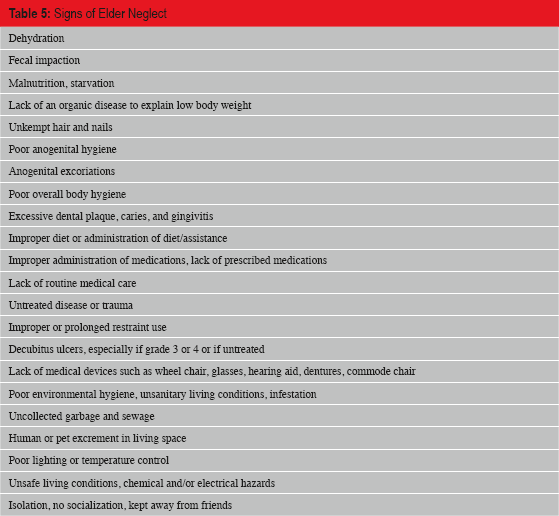
Neglect
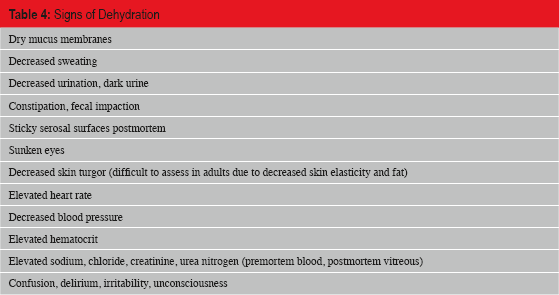
Neglect is the most common type of elder maltreatment. Neglect is defined as failure to provide basic care, goods, and/or services which are necessary to insure physical and psychological/emotional comfort (14). When an elder is physically neglected, findings may include dehydration, starvation, malnutrition, poor hygiene, unsafe living conditions and environment, or lack of medical care. Dehydration secondary to neglect is due to inaccessibility to water, intentional withholding of water, forced salt intake, or hyperthermic exposure. Physical and laboratory findings antemortem and at autopsy can indicate dehydration (
Signs of Dehydration
Signs of Elder Neglect
Restraints
According to the Centers for Medicare and Medicaid Services (CMS), “a restraint is any manual method, physical or mechanical device, material, or equipment that immobilizes the ability of a patient to move his or her arms, legs, body, or head freely…or a drug or medication when it is used as a restriction to manage the patient's freedom of movement and is not a standard treatment of dosage for the patient's condition”(22). Prolonged or improper use of restraints can cause abrasions, contusions, ulcers, injuries, chemical obtundation, or even death (23–26). Restraints limit an elder's movements and can lead to poor circulation, deep venous thrombosis, and pulmonary thromboembolism. At autopsy, special attention should be paid to the wrists, ankles, and axillae for marks of a restraint. Prolonged use may also present with decubitus ulcers of areas exposed to pressure such as the back, lumbar sacral area, heels, and elbows. Toxicology can detect psychotropic drugs used as chemical restraints (26).
Ancillary Studies
Various ancillary studies can be conducted on autopsy material for completeness of the elder death investigation. Postmortem radiology has already been discussed. Utilization of the pathology laboratories includes microbiology cultures for bacteria, fungi, and viruses, serum viral antibodies and enzymes vitreous chemistry for electrolytes, glucose, and ketones, toxicology of urine and peripheral blood, cytology and DNA analysis for sexual assault examinations, and histology of tissues including the use of special stains.
Elder Death Review Teams
Because disease and death are more common in older adults, current scientific research on elder abuse is limited, deaths of older adults are rarely questioned and because elder abuse is a growing problem, an increasing number of state and local jurisdictions have instituted interdisciplinary efforts and formed Elder Death Review Teams (EDRT) (27–31). EDRTs were initially developed in response to a 1998 Department of Justice focus group in an effort to “foster examination of and improvement in the responses” to elder abuse (30).
A review of the literature reveals existing EDRTs vary in size, scope and venue. EDRTs convene regularly on a weekly, monthly or quarterly basis to “focus on systemic issues raised by the cases” while others “determine the feasibility of prosecution” (6, 29–31). EDRTs improve interagency collaboration, coordination, and communication while raising awareness about the lethality of elder abuse to member agencies. EDRTs also identify data to be collected and compared, risk and protective factors and trends. Information identified through EDRTs provides objective data to improve systems, reporting and prevent similar deaths (3). EDRT findings also inform program administrators, policymakers and the public about the seriousness of elder abuse. EDRT findings can and have brought about changes in policy, law, response and funding (29). EDRTs are not intended as mechanisms to investigate mistakes, rather, EDRTs provide private, local, state and federal entities opportunities to analyze gaps in inter-agency practices, policies, and procedures.
Teams are typically comprised of medical examiner/coroner or their designee, law enforcement, emergency medical personnel, protective and regulatory services, district or prosecuting attorney, geriatrician, probate court, public health, Social Security Administration, psychologists and personnel from financial institutions since financial exploitation is the leading cause of elder abuse. EDRTs are often comprised of departments, agencies - entities designated by state law to investigate allegations of abuse, neglect and exploitation (A/N/E) followed by other primary and secondary responders and by departments, agencies, entities identified by the needs and resources of the respective EDRTs.
Elder Death Review Team Members (30)
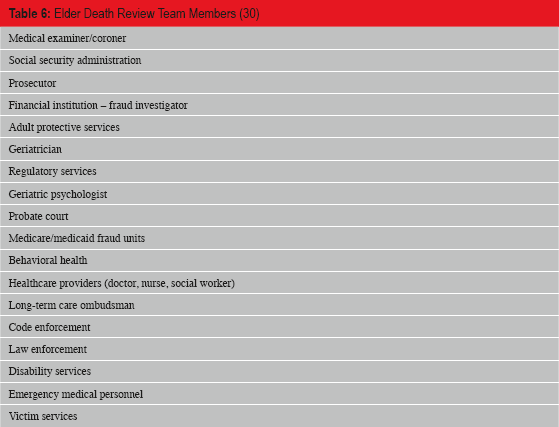
The needs of respective teams, including focus and scope of reviews, will determine the departments, agencies and entities to be included on EDRTs. The American Bar Association published the Elder Abuse Fatality Review Team Replication Manual in 2005 providing detailed instructions on developing, deploying and sustaining EDRTs. The replication manual is available online (30).
It is important to note “victim services” refers to programs providing a variety of direct services to victims of crime that may receive funding through the federal Victims of Crime Act and are separate from Adult Protective Services (30). Representatives of victim services are critical to EDRTs to ensure victim service programs understand the nature of elder abuse so more emphasis can be placed on the need for victim services for older adults prior to a lethal event.
Criteria for Case Review
Generally, review criteria includes cases in which an older adult, as defined by state law, has died due to questionable circumstances, unnatural causes such as abuse, neglect, and exploitation. Virginia's EDRT (31) includes cases in which at least one of the following factors is present: murder by family member, caregiver, or employee of a facility for aged individuals, suicide or assisted suicide, certain bruising, fractures or other injuries are present, inconsistencies in reporting information, unexpected or unattended deaths, drug overdose, previous or current Adult Protective Services report, forensic findings suggestive of abuse, neglect and/or exploitation, criminal investigations suggestive of A/N/E as cause/contributing factor, dehydration or malnourishment, and other lethality indicators.
Johnson County IA, inclusion criteria includes cases with the following factors: accidents, undetermined manner of death, and questionable circumstances such as poor living conditions and other factors leading to the consideration the death was preventable (27).
Fulton County Medical Examiner Project inclusion criteria also includes the following factors: shared living situations (unlicensed personal care homes), previous history with Regulatory Services (facility), previous history with law enforcement and emergency medical services at location, and previous reports to Adult Protective Services and law enforcement - especially those involving financial exploitation.
Case review criteria will be perfected as a condition of the EDRT review process over time for each EDRT based on resources. The case review criteria from the above EDRT's provide excellent factors to consider for case review selection.
In June 2014, a joint project of the Georgia Department of Human Services Division of Aging Services and the Fulton County (Atlanta) Medical Examiner's Office (FCMEO) was initiated after months of preparation to develop the database. The goal of the project is to develop and sustain a comprehensive database documenting demographics and risk factors regarding elder abuse, neglect, and exploitation for all deaths in Fulton County of adults age 65 years and older. This project addresses several gaps in the detection and reporting of elder abuse, neglect, and exploitation by combining the sources of the medical examiner's office, Adult Protective Services, and Health Facility Regulation (HFR). The medical examiner's office keeps an electronic metadata base of all death cases in Fulton County from 2006 to the present. Information in the database includes investigation details and scene photographs, next of kin relationships, autopsy results and photographs, medication and medical history, and lab results. They also have included an extra screen for any case in a nursing facility to document standardized additional information specific to those cases.
Adult Protective Services has records of any past complaints and cases with information about the case situations, victims, and perpetrators including household situations, and income amount and sources. Healthcare Facility Regulation is tasked with the licensing and oversight of all long-term care facilities in the state of Georgia. Their data include information on locations, number of beds, inspection reports, and types of violations for all nursing homes, personal care homes, assisted living communities, and community living arrangements.
Combining these sources provides a full picture of the risk factors known to be associated with abuse, neglect, and exploitation specific to each case. Outcomes for this project include an aging specific protocol for investigators and medical examiners, an evaluation of the prevalence of deaths associated with abuse, neglect, and exploitation with support of already identified risk factors, identification of new factors, and identification of unsafe environments for the current and future aging population in Georgia.
The FCMEO reviews are conducted weekly and provide real-time opportunities to impact medical examiner/coroner decision making. During the case review process, if positive findings of possible A/N/E are detected, the medical examiner can be notified, and based on the information, an autopsy can be performed or some further investigation pursued that otherwise might not have taken place.
The next step in the Georgia project will be to develop criteria for FCMEO cases with positive findings for A/N/E to be reviewed by an EDRT and the development of such a county EDRT.
Outcomes
As noted by American Bar Association (ABA), since there is an expectation older adults will die, one of the many benefits of EDRTs is raising the awareness of and thus, questions as to whether older adults “should have died in that manner or at that particular time” (30). As awareness from EDRT reviews increases, so will the knowledge that premature and unexplained deaths of older adults with be taken as seriously as those of children and younger adults (30).
As a result of death reviews, data collection and analysis, EDRTs “improve interagency case management, identify gaps in services, clarify data to be collected and suggest protocols and policy” (31). The following overview (
Overview of the Virginia Elder Death Review Team (EDRT) Process (31)
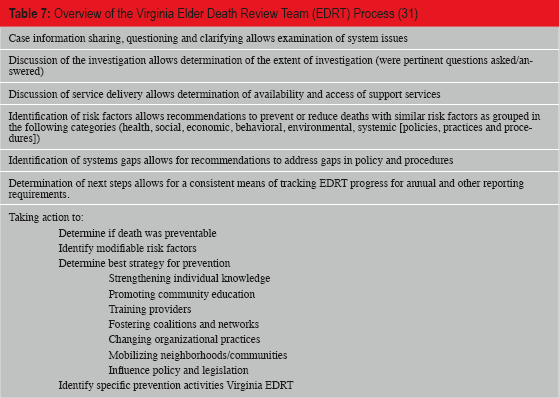
Goals of the initial ABA project were to “foster examination of and improvement in the responses” of primary and secondary responders to the growing number of A/N/E cases (30). A review of the literature suggests EDRTs are advancing knowledge related to fatal cases A/N/E. The final component related to EDRT outcomes is to ensure the involvement of or access to a policymaker with clout and credibility or the involvement of an entity that includes policymakers and others with influence who can act on the recommendations of the EDRT (30).
Conclusion
As the average age of the U.S. population continues to increase, the care of the elder segment is a growing concern. A collaborative effort between treating healthcare workers and postmortem investigators and medical examiners, law enforcement, and the judicial system is necessary to improve both the quality of life and the outcomes for all elders. The postmortem contribution to such collaboration requires that medical examiners, coroners, and medicolegal death investigators thoroughly investigate the deaths of elders. No elder death should be automatically assumed to have a natural manner based solely on age and past medical history (32, 33). Accidents, suicides, and homicides occur in this age group and will be overlooked with such an assumption (32, 33). As we protect our pediatric populations so we should protect our elders. A designation of elder should not be the basis for lack of thoroughness in a medicolegal death investigation.
Footnotes
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest.