
Abstract
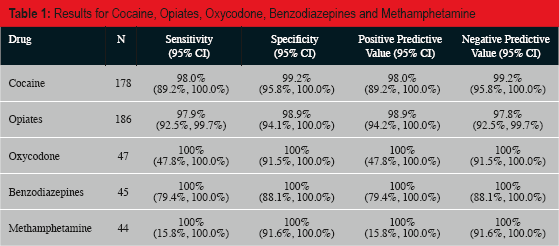
Urine dipsticks are an inexpensive, rapid tool for detecting common drugs of abuse (e.g., cocaine, oxycodone, methamphetamine, opiates, and benzodiazepines) in postmortem urine samples. For urine dipsticks to be useful as a triage modality, it is important that dipsticks have high diagnostic accuracy. We tested the performance of urine dipsticks as compared with toxicological analysis of postmortem blood as the gold standard for 198 cases for at least one of five common drugs of abuse during a six-month period at the Office of the Medical Examiner of Cook County, Illinois. Toxicological screening with enzyme-linked immunosorbent assay (ELISA) and confirmation with gas chromatography/mass spectrometry (GC/MS) were then performed on postmortem blood samples. The results were compared to calculate the sensitivity, specificity, positive predictive value, and negative predictive value of the urine dipstick screens. For cocaine (n=178), opiates (n=186), oxycodone (n=47), benzodiazepines (n=45), and methamphetamine (n=44), the sensitivity, specificity, positive predictive value, and negative predictive value of the urine dipsticks all exceeded 97%. Urine dipsticks are an accurate and reliable screening tool for drugs of abuse. This inexpensive screen may be used to triage cases to autopsy or external examination in cases where the differential includes natural disease versus drug-related death.
Introduction
Dipstick drug screens are tests used to screen for common drugs of abuse (e.g., cocaine, oxycodone, methamphetamine, opiates, and benzodiazepines) in urine samples. Dipsticks are used in workplace, hospital, emergency room, and forensic settings. They are inexpensive, easy to use, and give results within minutes. They were developed specifically for use with urine samples but may also be used on a limited number of other specimens (1). The dipstick technology consists of a competitive immunoassay chromatographic absorbent device in which drugs or drug metabolites within a sample compete with a drug/protein conjugate for a limited number of antibody/dye conjugate binding sites.
Although dipsticks have advantages as a screening test, they also have limitations. A positive screening test on urine is not enough to prove very recent drug use or drug overdose (2). Urine dipsticks are qualitative tests that do not provide concentrations of drug detected. Immunoassays have been shown to be subject to false positive results due to cross reactivity with numerous other drugs (3, 4). Conversely, dipsticks may provide false negative results due to high cutoff sensitivities. In addition, dipsticks provide a limited range of drugs detected. For these reasons, death due to drug toxicity cannot be determined based on dipstick results alone.
However, despite these limitations, dipsticks can be of use when triaging cases to autopsy or external examination when the differential diagnosis includes natural disease and drug toxicity. For urine dipsticks to be useful as a triage modality in a forensic pathology setting, it is important that the outcomes of the dipsticks have high concordance with the toxicological analysis subsequently performed on tissue specimens, specifically blood. We tested the performance of urine dipsticks as compared with toxicological analysis by gas chromatography/mass spectroscopy of postmortem blood as the gold standard.
Methods
We conducted a prospective study on 198 cases during a six-month period (March of 2013 to August of 2013) at the Office of the Medical Examiner of Cook County, Illinois. The rate of drug-related deaths during this five-month period was 10.1% (300 of 2970 total cases). Of these 300 drug-related deaths, 97% (290 of 300) were due to drugs of abuse and 3% (10 of 300) were due to non-narcotic prescription and over-the-counter drugs.
Cases were included in the study if the differential diagnosis included drug toxicity versus natural death. Cases were nonsequential and based on the participation of the staff physicians. Dipsticks were performed on all cases in the study for at least one of five drugs of abuse by 13 attending pathologists at the office. The specimens were obtained via percutaneous needle puncture and aspiration or via direct visualization and needle puncture (i.e., of the bladder after the body had been opened) and aspiration. Cases were not excluded based on special circumstances (e.g., decomposition). The dipsticks were performed on urine (183 specimens), cerebrospinal fluid (9 specimens), peritoneal fluid (1 specimen), cavity fluid (1 specimen), vitreous fluid (1 specimen), and unknown (3 specimens). These results were then correlated with the final toxicology report once available and tabulated.
The dipsticks used were Discover Drug Test Cards manufactured by American Screening Corporation, Shreveport, Louisiana. The unit price was $0.55 per dipstick. The cutoff sensitivities for the Discover Drug Test Cards were as follows: cocaine, 150 ng/mL; opiates, 300 ng/mL; oxycodone, 100 ng/mL; benzodiazepines, 300 ng/mL; and methamphetamine, 500 ng/mL. The cocaine dipstick (as well as the subsequent enzyme-linked immunosorbent assay or ELISA screen) tests for the cocaine metabolite benzoylecgonine. The opiate dipstick tests for multiple opiates including morphine, heroin, and codeine, but does not test for methadone.
Toxicological screening by standard ELISA technology was performed with confirmation by gas chromatography/mass spectrometry (GC/MS) on postmortem blood samples (using peripheral blood when available). The ELISA screening was performed on an Immunalysis Tecan Sunrise Manual Kit Reader. The cutoff sensitivities for ELISA were as follows: cocaine, 50 ng/mL; opiates, 30 ng/mL; benzodiazepines, 15 ng/mL; and methamphetamine, 250 ng/mL. The GC/MS toxicology was performed using a tandem technique on an Agilent Technologies 6890 GC coupled with a 5973 mass selective detector (MSD) and an Agilent Technologies 7890 GC coupled with a 5875 MSD. The cutoff sensitivities for GC/MS were as follows: cocaine, 50 ng/mL; benzoylecgonine, 120 ng/mL; opiates, 20 ng/mL; oxycodone, 100 ng/mL; benzodiazepines, 100 ng/mL; and methamphetamine, 75 ng/mL.
We recognize that the dipstick screens were performed on body fluids other than blood, predominantly urine, and that the toxicology tests were performed on blood. It is therefore not possible to determine a true false positive or false negative rate for the rapidly screened specimens from the results. We approached this study from a clinical perspective and attempted to determine whether a dipstick screen result is a good indicator of the presence of the same drug in the blood. The outcomes of the rapid screens and final assays were compared to calculate the sensitivities, specificities, positive predictive values, negative predictive values, and 95% confidence intervals of the urine dipstick screens using Statistical Analysis Software (SAS) version 9.4.
Results
Urine dipsticks were performed for cocaine (n=178)
Results for Cocaine, Opiates, Oxycodone, Benzodiazepines and Methamphetamine
Test Results for Cocaine, Opiates, Oxycodone, Benzodiazepines and Methamphetamine
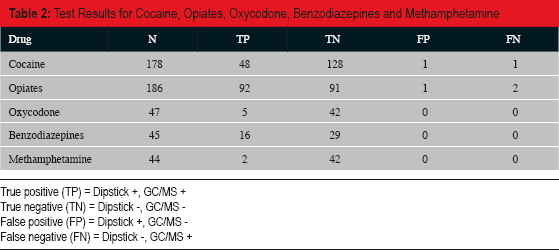
True positive (TP) = Dipstick +, GC/MS +
True negative (TN) = Dipstick −, GC/MS −
False positive (FP) = Dipstick +, GC/MS −
False negative (FN) = Dipstick −, GC/MS +
Urine dipsticks were also performed for opiates (n=186)
Urine dipsticks were also performed for oxycodone (n=47), benzodiazepines (n=45), and methamphetamine (n=44)
No toxicities from non-narcotic prescription drugs or over-the-counter drugs were found during the course of this study.
Discussion
Dipstick tests are occasionally performed in medical examiner's offices to triage cases to autopsy or external examination. To be well-suited for this use, it is important that the results of urine dipsticks highly correlate with the results of the gold standard test, toxicological analysis using GC/MS. The goal of this study was to determine how closely these results match.
For five common drugs of abuse (cocaine, opiates, oxycodone, benzodiazepines, and methamphetamine), the sensitivities, specificities, positive predictive values, and negative predictive values of the urine dipsticks all exceeded 97%. These results show a lower rate of discrepant results between dipstick screens and toxicology than similar studies (5, 6). This may be due to differences in study design, in the drug use of the population studied, or in the dipstick technology used. Our results show that dipsticks are an accurate and reliable screening tool for drugs of abuse; however, small sample sizes for several drugs produced fairly wide confidence intervals.
We recognize that, because the dipstick tests were performed on urine and GC/MS was performed on peripheral blood, discrepant results between the two tests cannot be considered true false positives or false negatives. However, by comparing the results of these two tests, we were able to show that urine dipsticks may be used with confidence to triage cases to autopsy or external examination. This is of use in cases in which the differential diagnosis includes natural disease versus drug-related death (e.g., a 55-year-old with history of hypertension and remote cocaine use). They may also be useful in signing out cases immediately following the autopsy rather than pending for toxicology (e.g., a 35-year-old with ruptured aortic dissection and screens negative for cocaine and methamphetamine). Occasionally, dipstick results may lead the pathologist to an autopsy or a pending status on a seemingly natural death (e.g., a 55-year-old woman with heart disease and screens positive for opiates and benzodiazepines).
Areas for further inquiry include gathering larger numbers of cases of dipstick screens of benzodiazepines, oxycodone, and methamphetamine to produce narrower confidence intervals. Additionally, this preliminary study included fifteen specimens other than urine (cerebrospinal fluid, peritoneal fluid, cavity fluid, and vitreous fluid) on which dipsticks were performed. Further studies will need to be conducted that evaluate these specimens in terms of their utility for drug detection. This would include determining the limits of detection (LOD), limits of quantification (LOQ), background matrix effects, and drug tissue dispositions of these matrices.
It is clear that death due to overdose cannot be determined based on dipstick results; toxicological analysis on blood and correlation with the circumstances of death is required prior to rendering this opinion (7). Dipsticks can be used to triage some cases to autopsy or more comprehensive toxicological analysis; to document the lack of involvement of drugs in cases of catastrophic natural disease (e.g., cerebrovascular accidents, ruptured aneurysms, or acute myocardial infarcts) detected at autopsy or to rule out recent drug use in individuals with a history of both natural disease and substance abuse. Rapid screening may also be used to direct the pathologist toward additional adjunctive testing (e.g., cardiac or neuropathology consultation, histology, microbiology) if a negative result is obtained for a young individual who dies suddenly. In high profile cases, such as potential excited delirium syndrome while in custody, rapid screens may be useful in identifying potential drug involvement.
While additional dipstick drug screens are available, we only screened for the substances indicated above in this limited study. When combined drug toxicity was in the differential, comprehensive toxicological analysis was ordered. There is significant variation in the extent of toxicological analysis performed between offices based on policies and resources. The Cook County Medical Examiner's Office performs comprehensive toxicology when indicated but will often start with a limited panel (cocaine, opiates, and ethanol) prior to additional testing, as these substances account for the vast majority of our toxicity-related deaths. Ethanol screening and quantification was performed on peripheral blood and/or vitreous fluid in all cases in this study. If ethanol was suspected to contribute to death, stat analysis on vitreous fluid was completed the day of the autopsy.
Although dipstick drug screen results are accurate and reliable predictors of the subsequent toxicology results, it is important to keep in mind that dipsticks offer a limited range of drugs detected. All available information must be taken into account when selecting cases to triage using dipsticks so that potential cases of over-the-counter drug, non-narcotic prescription drug, or synthetic drug toxicity are not missed. In many cases, dipstick drug screens are not an adequate alternative to a more comprehensive toxicology panel.
Conclusions
Both positive and negative rapid drug screens utilizing dipsticks on postmortem body fluids correlate highly with results obtained from analysis of postmortem blood in the toxicology laboratory. Dipsticks cannot be used to confirm death due to drug toxicity; they can confirm drug use over hours/days leading up to death depending on the drug subjected to rapid screening. Dipsticks can be used as a triage tool in the autopsy room to suggest autopsy versus external examination in some cases, to exclude drug involvement in the setting of catastrophic natural disease encountered at autopsy, or to lead to other adjunctive studies in the setting of negative results.
Footnotes
This work was presented at the 2014 Annual Meeting of the National Association of Medical Examiners.
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest.