
Abstract
Sudden natural asphyxial death in adults due to airway obstruction is an unusual cause of death. A variety of etiologies can cause airway obstruction, including benign or malignant tumors and soft tissue swelling from asthma, infections, or anaphylaxis.
Malignant tracheal neoplasms are exceedingly rare with a reported incidence of approximately 2/1 000 000 and the small cell carcinoma subtype accounts for <10% of these tumors.
We present a case of a 55-year-old female smoker who was found dead at home. At autopsy an obstructing lesion of the proximal trachea was identified that showed the characteristic cytomorphology of small cell carcinoma. No primary pulmonary lesions were identified. The cause of death was determined to be obstruction of the trachea by small cell carcinoma and the manner, natural.
Introduction
Sudden death in adults is a common scenario encountered by forensic pathologists. A thorough scene investigation, history, and external and internal exam with toxicology testing are necessary in order to properly identify and classify the cause and manner of death. Cardiovascular causes are by far the most common causes of sudden death in adults, while respiratory causes, including acute obstruction from trachea-laryngeal tumors, are uncommon (1, 2).
Primary tracheal malignancies are uncommon tumors with an estimated incidence of 0.2/100 000 new cases per year. Of those, the squamous cell carcinoma subtype predominates, representing approximately 50%, while small cell carcinoma makes up less than 10% (3).
Asphyxia is most simply defined as the lack of uptake or utilization of oxygen (1). Asphyxial deaths may arise from a variety of etiologies, and can be broadly placed into two categories: intrinsic and extrinsic. Intrinsic factors include those that cause obstruction of the airway from within, such as soft tissue swelling from infections, asthma, or anaphylaxis, and benign or malignant tumors of the upper airway. Extrinsic factors include those that cause external compression of the neck or chest that interfere with airflow into and out of the lungs. These include strangulation, hanging, smothering, or positional asphyxia. A final category is inadequate availability of oxygen. This can be via displacement in the environment by an inert gas such as helium, displacement of oxygen from hemoglobin such as with carbon monoxide, or exposure to high altitude and its accompanying low oxygen tension. The manner of death in any of the above scenarios may be natural, accident, suicide, or homicide.
We report a case of a primary tracheal small cell carcinoma causing sudden asphyxial death in a 55-year-old female. This case is remarkable for the rareness of the tumor combined with an unusual, if not entirely unseen, cause of sudden death in an adult.
Case Report
The decedent was a 55-year-old female smoker with a history of depression. She had recently visited the hospital with complaints of wheezing. She was found unresponsive in her home with her head deviated to the right against a closed closet door. There was no evidence of foul play.
At autopsy the body was a noted to be a normally developed obese female. There was no evidence of external trauma. Tardieu spots were present over the upper face, anterior thorax, and anterior proximal right upper arm. Internal examination showed a 3 x 2.5 x 1.5 cm nodular lesion obstructing the proximal trachea
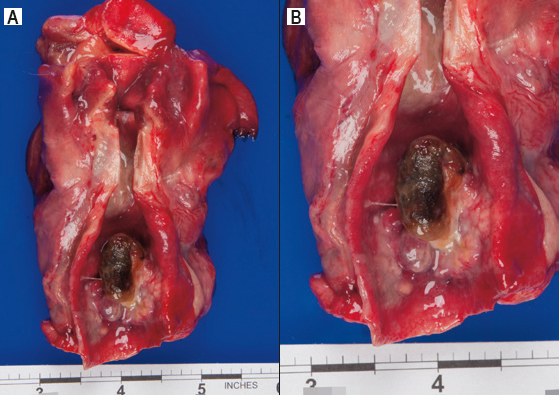
(A) and (B) The 3 x 2.5 x 1.5 cm proximal tracheal mass.
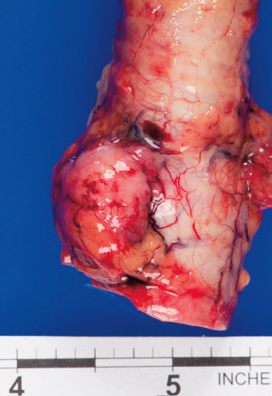
Enlarged paratracheal lymph node.
Microscopic examination of the tracheal mass revealed small-to medium-sized pleomorphic and discohesive cells with hyperchromatic nuclei, salt-and-pepper chromatin and scant cytoplasm
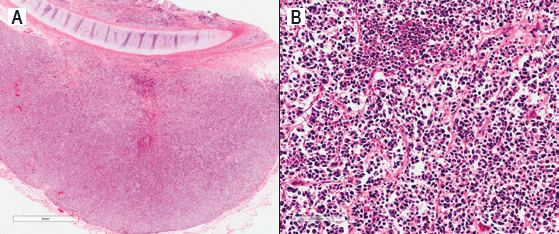
(A) Low power view showing overall nodular growth of the tracheal tumor (H&E, x10). (B) High power view showing discohesive tumor cells with hyperchromatic nuclei in a nested growth pattern (H&E, x200). There is necrosis present (upper, center).
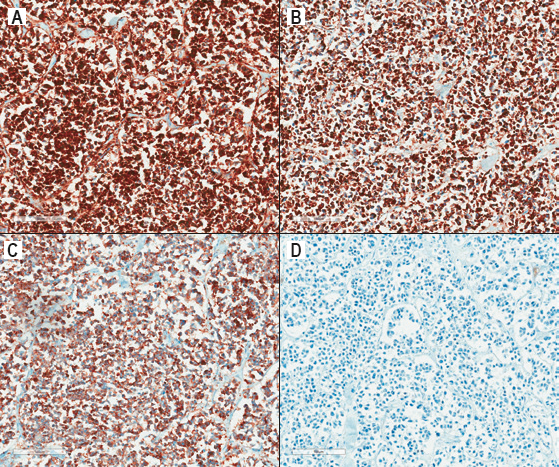
Immunohistochemical stains show the tumor cells are diffusely positive for CD56 (A), chromogranin (B), and synaptophysin (C), and are negative for TTF-1 (D) (all magnifications are 200x).
A toxicology screen was positive for low concentrations of cyclobenzaprine (0.11 mg/L), morphine (62 ng/mL), and venlafaxine (0.19 mg/L).
The cause of death was determined to be obstruction of the trachea by small cell carcinoma and the manner, natural.
Discussion
Primary small cell carcinomas of the trachea are uncommon neoplasms. It is difficult to estimate the annual incidence due to their rarity and the fact that they are often lumped in the literature under the category of “other” or “neuroendocrine” tumors when classifying primary tracheal malignancies. A recent review by Heikel found a total of 1747 cases of primary tracheal malignancies reported in the English literature, of which 71 (4%) were small cell carcinoma (3).
Classically, small cell carcinomas are associated with a smoking history, are found centrally in the lung, and metastasize readily. Histologically, they are composed of sheets, trabeculae, nests, or rosettes of small tumor cells with finely stippled chromatin, scant cytoplasm, indistinct cell borders, and inconspicuous to absent nucleoli. Mitoses, apoptosis, and geographic necrosis are common. The presence of nuclear molding and crush artifact are helpful, if not entirely specific, features (4).
Immunohistochemistry is generally unnecessary if well-preserved material is available for examination with routine hematoxalin and eosin stained slides. If performed, the tumors demonstrate reactivity for CD56, synaptophysin, and chromogranin in the majority of cases. TTF-1 is typically positive in pulmonary small cell carcinoma (>90% of cases) (4), but the staining pattern of primary extrapulmonary small cell carcinomas is variably reported as between 20–80% positivity (5). Of note, none of the series examining extrapulmonary TTF-1 staining had a tracheal primary in their series (6–8). A single case report showed weak positivity for TTF-1 staining in a primary tracheal small cell carcinoma causing acute respiratory failure (9).
The differential diagnosis of small cell carcinoma includes other neuroendocrine malignancies such as typical or atypical carcinoid tumors, large cell neuroendocrine tumors, basaloid squamous cell carcinoma, and other tumors demonstrating small round blue cell morphology (4).
Laryngopharyngeal and esophageal tumors, both benign and malignant, have been shown to cause sudden asphyxial death (10–23). However, asphyxia due to an obstructing tracheal small cell carcinoma has been previously unreported.
Tracheal tumors are often slow growing with an insidious onset of a variety of symptoms such as cough, dyspnea, stridor, wheezing, hemoptysis, or hoarseness. These are nonspecific and may lead to a delay in diagnosis, or misdiagnosis by a benign etiology such as asthma. This can allow the tumor to become large and obstructive before coming to clinical attention (24).
Although the tumor may be large enough to cause symptoms, airflow through the trachea is still possible. A terminal increase in size of the tumor leading to complete exclusion of the trachea or additional external stressor exacerbating the lack of oxygen is necessary before death occurs due to asphyxia. In the present case, a dark discoloration is visible on the surface of the tumor
Autopsy findings in asphyxial deaths can include visceral congestion, petechiae, cyanosis, and fluidity (decreased viscosity) of blood (1), however, these findings are nonspecific and can be seen in deaths from other causes, and be absent in deaths due to asphyxia. Therefore, in cases of space-occupying tracheal lesions, a careful in situ examination of the neck block with documentation of the position, size, and percent circumference of the trachea occupied by the mass is critical to support assigning an obstructing tracheal tumor as the cause of death.
Conclusion
In conclusion, the present case highlights the intersection of two unusual circumstances: sudden death in an adult with a respiratory etiology by an exceedingly rare primary small cell carcinoma of the trachea. Forensic pathologists should be aware of the possibility of an obstructing tracheal mass as the cause of death and consider small cell carcinoma subtype when confronted with the classic histomorphology. In addition, to the authors knowledge, this is the first report of TTF-1 negativity in a primary tracheal small cell carcinoma, and the first report of a primary tracheal small cell carcinoma causing an acute obstructive asphyxial death in an adult.
Footnotes
Acknowledgements
The authors would like to thank Dr. Mukhopadhyay for his helpful advice in researching this paper.
This work was presented at the 2014 Annual Meeting of the National Association of Medical Examiners.
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest.