
Abstract
Sudden cardiac death (SCD) often falls under the jurisdiction of the medical examiner (ME). A recent expert consensus statement recommends cardiac evaluation for all first degree blood relatives of an individual with SCD and supports the referral of these family members to a multidisciplinary inherited arrhythmia clinic; however, most MEs lack the appropriate clinical network for a specific referral and family members are often not followed up. In 2010, Minnesota MEs and cardiovascular pathologists began collaborating with a cardiology referral center specializing in familial cardiac conditions to form a regional Sudden Death Network (SDN). The cardiac pathologists and MEs have established protocols for appropriate specimen retention in accordance with the National Association of Medical Examiners position paper on postmortem deoxyribonucleic acid (DNA) collection and for referring families for clinical evaluation. The expertise of a genetic counselor has been essential to the evaluation of these families in coordinating appropriate genetic testing and assisting with the identification of at-risk family members in extended pedigrees. This SDN uses a multidisciplinary approach for referral of family members for screening and treatment of SCD risk and represents an important resource for MEs. Development of SDNs across the country would lead to a more uniform approach to SCD follow-up and a more efficient use of clinical resources. The ME's role is essential in consulting cardiac pathologists when needed, establishing the correct diagnosis, collecting and retaining appropriate specimens, and initiating the referral of at-risk family members to specialists.
Introduction
In recent years, we have gained more knowledge about heritable causes of sudden cardiac death (SCD), many of which frequently present as sudden unexpected death without prior symptoms and/or without a prior definite clinical diagnosis. Most of these sudden, unexpected deaths fall under the jurisdiction of the medical examiner (ME). MEs and coroners often struggle with how to advise surviving family members when the diagnosis of a familial disease has been made or suspected after sudden cardiac death.
In Minnesota, there has been a longstanding collaboration between ME offices and cardiac pathologists, resulting in strong diagnostics and consistency in practice. While we were consistent in our postmortem examinations and ability to recognize heritable cardiac conditions and need for additional molecular testing, we struggled with the best way to relay this important information to families. For many years, the follow-up consisted of a letter sent to the legal next of kin informing them of the cause of death, noting that the condition may be genetic, and advising them to seek care from “a cardiologist.” This approach was often unsatisfying, and we were frequently left not knowing if the family followed up at all, much less found a cardiologist equipped to work up an entire family for a potential heritable disease.
In 2010, one Minnesota ME office was approached by a large, well-respected cardiology group interested in evaluating, screening, and providing clinical care for such families following the sudden cardiac death of their relative. This group had established the Genetic Arrhythmia Center (GAC) at the Minneapolis Heart Institute, a collaborative specialty cardiology clinic with all the resources necessary to investigate and manage familial cardiac conditions, including channelopathies and cardiomyopathies. They had already recognized the necessity of evaluating family members of their patients with recognized heritable cardiac disease, but soon realized that they were missing an entire population: families of those whose heritable cardiac disease presented with sudden death, who died without prior contact with physicians or with an incomplete or inconclusive diagnosis. The GAC aims to help these families achieve a diagnosis and provide a screening strategy for family members, including referral to other cardiology centers (including out-of-state referrals) when convenient and/or requested. With this partnership with GAC, MEs can ensure that families receive the appropriate workup. This sudden death network (SDN) began with just one office, but was so beneficial to both parties that it quickly expanded to include multiple Minnesota ME offices. Our simple, low-cost protocol for sudden cardiac death follow up is presented below.
Discussion
Medical Examiner Protocol for Collection and Retention of Specimens
The SDN established protocol is as follows
Medical Examiner Sudden Cardiac Death Protocol
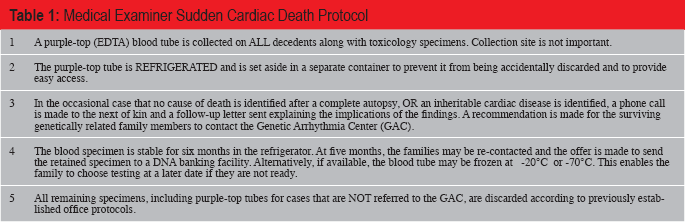
A purple-top ethylenediaminetetraacetic acid (EDTA) blood tube is collected on ALL decedents along with toxicology specimens. Collection site (peripheral versus central/cardiac) is not important.
The purple-top tube is refrigerated in a container separate from routine toxicology specimens to prevent it from being accidentally discarded and to provide easy access. It is retained there until we receive a request from the genetic testing laboratory for the specimen to be sent.
If no cause of death is identified after a complete autopsy, OR a heritable cardiac disease is identified, a phone call is made to the next of kin and a follow-up letter is sent explaining the potential implications of the findings for family members. A recommendation is made for the surviving genetically related family members (children, parents, and siblings) to contact the clinic coordinator for the Genetic Arrhythmia Center (GAC) in order to schedule clinical evaluations.
The blood specimen is stable for potentially many months in the refrigerator at 4°C (1). Individual laboratories may have different standards for storage, but our group was advised that the GAC's laboratory of choice recommended a maximum of six months in the refrigerator. After six months, if available, the blood tube may alternatively be frozen at −20°C or −70°C. If freezing is not an option, the families are recontacted and the offer is made to send the retained specimen to a clinical deoxyribonucleic acid (DNA) banking facility. This enables the family to pursue genetic testing at a later date.
All remaining specimens, including purple-top tubes for cases that are not referred to the GAC, are discarded according to previously established office protocols.
This protocol has been implemented at the Hennepin County Medical Examiner's office. A purple-top EDTA blood tube is collected at the time of all postmortem examinations
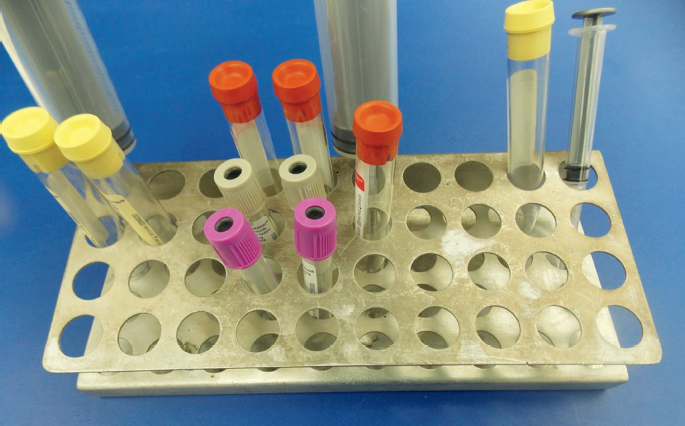
The addition of a single purple-top blood tube is part of the office's regular collection of fluids for potential toxicology and chemistry testing (yellow-top tubes for urine; yellow-top tube for vitreous; and red-, grey-, and purple-top tubes for blood).
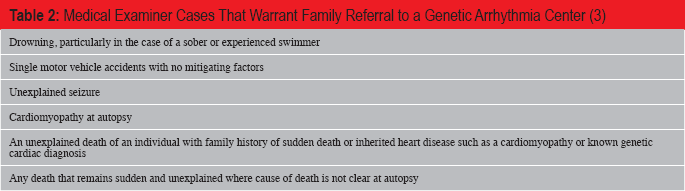
In cases where the history, scene investigation, and negative gross autopsy raise the concern of a possible sudden cardiac death with no morphological findings (such as a cardiac channelopathy), the heart is often referred to the Jesse Edwards Registry for expert cardiovascular pathology consultation. If such consultation also fails to establish a cause of death, then the protocol outlined in this paper is activated and the purple-top tube of blood is saved indefinitely for possible genetic testing. Similarly, if a morphological and potentially heritable disease (such as hypertrophic cardiomyopathy or arrhythmogenic cardiomyopathy) is established by the postmortem or cardiac pathology examination, then the purple-top tube of blood is saved and the family is referred for genetic counseling. According to NAME guidelines, sudden death cases with factors such as drowning of an experienced swimmer, single motor vehicle accidents with no mitigating factors, unexplained seizures, and/or known family history of cardiomyopathy or heritable channelopathy also warrant specimen collection and retention
Medical Examiner Cases That Warrant Family Referral to a Genetic Arrhythmia Center (3)
Medical examiner communication with the family throughout the process is key. When a heritable cardiac cause of death is a strongly suspected—whether a channelopathy or a cardiomyopathy—beginning the conversations with the family about cardiac pathology consultation and possible follow up testing can be very helpful. When the autopsy is complete and the death certified, telephone communication with the family, followed by a clearly written letter
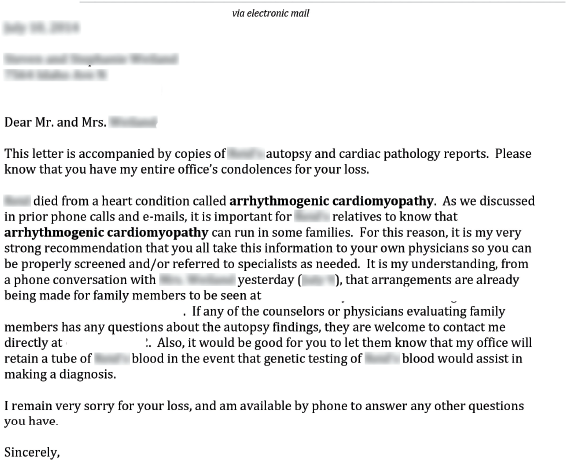
An example of a cover letter sent in follow-up to phone conversations and meant to accompany the autopsy report sent to family members.
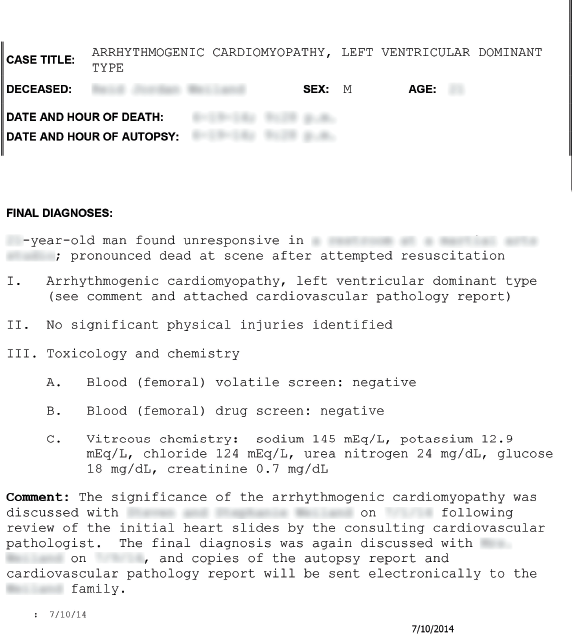
An example of an autopsy report (cover sheet) in a sudden cardiac death case with a comment.
The Hennepin County Medical Examiner's office performed 4472 autopsies between January 2010 and February 2015. Among these, there were a total of 36 cases in which either no anatomic cause of death was found, or an inheritable cardiomyopathy was diagnosed. The age range was two to 53 years (average 31 years old), with 25 males and 11 females. There were six hypertrophic cardiomyopathy cases (19 to 53 years old; average 34 years old; five male and one female), nine arrhythmogenic cardiomyopathy cases (18 to 50 years-old; average 36 years old; nine male and zero female), and one case (32 year old male) with features of both ARC and HCM. Twenty cases were suspicious for a channelopathy—these ranged from two to 53 years old, average 29 years old, with ten males and nine females. In three instances, the retained blood tube was released for DNA banking and four specimens were released for genetic testing. In all but two of the 36 cases, it was documented that a family member was apprised of the heritable nature of the condition and was provided with a copy of the autopsy to accompany them to any subsequent evaluation. The GAC has seen over 500 patients, and although the clinic is not able to track every patient screened, diagnosed, and treated from a single SDN referral, it is estimated that dozens of family members of decedents have been seen in that clinic alone. Of those, many have been diagnosed with inheritable cardiac conditions (some by clinical workup, others via genetic testing for channelopathies) which were able to be treated. It is not possible to know the disposition of all of the families, as they may seek care at any number of institutions and usually do not choose to provide feedback to the medical examiner. Many families choose to not seek the recommended follow-up care at all.
Even in a large medical examiner's office, the collection and storage of one additional purple-top tube of blood in every case imposes little additional burden on the office's storage space

An entire month of purple-top tubes (generally 90 to 100 per month) is easily stored in a small amount of space.
An entire year of purple-top tubes is easily stored in a small amount of space.
Role of the Genetic Arrhythmia Center
Families may benefit from optimal counseling, screening, and consolidated care for heritable cardiac conditions in a multidisciplinary GAC. Potentially lethal familial cardiac conditions are often missed in the community for various reasons. To begin with, these uncommon diseases often involve family members receiving scattered medical care for similar cardiac presentations. Reaching a specific diagnosis becomes a challenge under these conditions. This is further complicated by the fact that familial conditions can have various expressions among family members even with the same genetic mutation. Even when properly diagnosed, screening of family members is often uncoordinated and nonuniform. A specialized GAC can alleviate many of these issues, as its intent is to provide comprehensive consolidated care for patients with familial cardiac conditions as well as appropriate screening for their families.
A comprehensive GAC requires the involvement of multiple cardiac subspecialties including adult and pediatric cardiac electrophysiologists, advanced cardiac imaging (to provide clinical screening), and advanced heart failure specialists who can help to manage patients with familial cardiomyopathy. This requires a dedicated group of physicians as well as an infrastructure that can support this model and facilitate communication and screening for these families.
When a patient is referred to the GAC, each family member is initially seen by an electrophysiologist. If the family came to the clinic via the SDN, autopsy and cardiac pathology results are incorporated with the clinical and family history to provide appropriate counseling for these family members, including guidance with regard to screening. GAC cardiologists employ tailored screening and follow-up protocols specific to the diagnosis. Some screening, such as imaging, may be completed prior to the initial visit. Both the initial workup of family members and the subsequent long term care and follow-up may be complex and time-consuming. Heart failure and/or cardiac transplant specialists may become involved as required. Genetic counseling plays a crucial role in clinical decision making. Complex care protocols are organized by dedicated nurses, a clinic coordinator and research coordinator.
Based on this evaluation and counseling, the GAC physician and the family can determine the potential benefit from genetic testing on the deceased relative using a stored specimen. The discussion and counseling provided by the evaluating physician and genetic counselor then forms the basis of an informed decision on whether or not to proceed with genetic testing.
Role of the Genetic Counselor
Genetic counselors are master's level healthcare providers trained in medical genetics and psychosocial counseling. In the setting of sudden cardiac death, genetic counselors function in a collaborative role with medical examiners and cardiologists to ensure the proper approach to the molecular autopsy for a decedent.
In cases of sudden cardiac death, the involvement of a genetic counselor allows the provision of genetic counseling to the family members of the decedent. Genetic counseling is optimally provided prior to the initiation of postmortem genetic testing, allowing the family to decide which approach to genetic testing best suits them. For some families, this involves immediate genetic testing of DNA from the decedent. For others, it may involve delaying testing and instead proceeding with clinical DNA banking to ensure the potential for genetic testing in the future.
Postmortem Genetic Counseling Session
Genetic counseling sessions in the postmortem setting are uniquely challenging and typically involve the following five components:
Review of the decedent's medical history (specifically inquiring about a history of syncope, seizures, prior cardiac arrest, prior cardiac evaluations, any known cardiac abnormalities, and the circumstances surrounding the death).
Construction of a detailed four-generation, cardiac-targeted pedigree specifically documenting any individuals with sudden death
Family history assessment is essential to the genetic testing process, and enables the most informative approach to genetic testing. The gold standard in genetics is to initiate genetic testing with an affected individual, as such individuals offer the greatest likelihood of demonstrating a disease-causing mutation that can then be used to clarify the risk for family members. In some cases, genetic testing may be best initiated for the decedent with pathologic evidence of disease or with a negative autopsy, as careful family history assessment may not reveal any living family members with disease. It is important to note, however, that most inherited channelopathies and cardiomyopathies are not fully penetrant, meaning that there may be family members who carry a familial pathogenic mutation but do not express disease (either due to reduced penetrance or because not all family members may have undergone careful cardiac assessment). These are important factors to consider in assessment of the decedent's pedigree.
In other cases, pedigree assessment may reveal a living family member who is symptomatic or has evidence of disease. It may then be possible to initiate the genetic testing process with the living, affected family member as opposed to starting with the decedent. This approach may be equally informative and may offer significant cost savings to the family of the decedent, as third-party payers seldom provide reimbursement for a molecular autopsy. Genetic testing in a living, affected family member, however, is frequently reimbursed by third-party payers.
Confirmation with the medical examiner's office that an appropriate DNA specimen is available from the decedent (preferably five to ten mL of blood collected at autopsy that is preserved with EDTA, usually a purple-top tube) (3). DNA extracted from fixed tissue specimens that are routinely saved during autopsy does not have a reliably high quality to be utilized for comprehensive postmortem genetic testing. Similarly, blood specimens collected in tubes that contain sodium fluoride (gray-top) or tubes lacking a preservative (red-top) are less likely to allow extraction of adequate DNA for genetic testing. Blood spot cards, while space-saving and convenient, are not accepted by all clinical laboratories for the next generation sequencing methods that are used to identify disease-causing mutations. This may become more widely available in the future.
Discussion of genetic testing options (and associated costs) available to the family with regard to genetic testing. This may include testing the decedent or testing a living affected family member. Genetic counseling also includes a discussion of the various types of genetic test results that may be found, including positive results, negative results, and variants of unknown significance (in which a DNA variant is identified in one of the genes that are tested, but its clinical significance is currently unknown). When variants of unknown significance are identified, genetic counseling is important to provide the family with recommendations related to follow-up and clarification of the variant.
Psychosocial support is of paramount importance in the postmortem genetic counseling session. Families suffering the loss of their spouses, children, siblings or other relatives are frequently overwhelmed and struggling with their grief. In such cases, it is apparent that the lack of explanation for the sudden death of their family member causes near equivalent distress when compared with the loss of the family member from their lives. Families in the midst of such grief require careful, skilled genetic counseling.
Families undergoing genetic testing frequently raise concerns about how the results may affect their ability to obtain insurance in the future. Life insurance eligibility may certainly be affected by the presence of a disease-causing genetic mutation of any kind; however, under the Affordable Care Act, health insurance plans may no longer deny coverage due to a pre-existing condition (4). Additionally, the Genetic Information Nondiscrimination Act of 2008 (GINA) is a federal law that prohibits discrimination in health coverage based on genetic information (5). Title II of GINA took effect in 2009. “Under GINA, it is illegal to discriminate against employees or applicants because of genetic information” (6). GINAs protections do not apply to life insurance, disability insurance or long term care insurance.
Evolving Nature of Postmortem Genetic Testing
Genetic testing in the postmortem setting is rapidly evolving. Historically, postmortem genetic testing has been performed by pursuing testing for the most likely clinical condition based on circumstances of death. For example, a young person experiencing sudden death while running may have been suspected of having long QT syndrome (LQTS), and a panel of genes specific to this condition was tested. If the panel of LQTS genes did not reveal a mutation, testing may have then been initiated for catecholaminergic polymorphic ventricular tachycardia (CPVT). This stepwise approach required adequate DNA to run multiple tests, which is challenging in a postmortem setting with a limited amount of blood typically collected from the decedent. Further, such a stepwise approach to testing involved considerable cost to the family, with each test having its own associated fees that were seldom, if ever, covered by third-party payers. Recent advances in genetic testing have led to the emergence of large multigene panel tests for cardiomyopathy and arrhythmia genes, which encompass many cardiac conditions that are tested simultaneously. The advantage of such testing is the cost savings as well as the opportunity to evaluate a larger number of genes for multiple cardiac conditions that may have clinical overlap. The disadvantage of such testing is the larger number of variants of unknown significance that may be identified, leaving a family with ambiguity regarding the result and how it may (or may not) be applied to surviving family members. Future testing in the postmortem arena will likely evolve to include whole exome or whole genome testing. In fact, such testing is already being used to identify disease-causing mutations in some families (7, 8). Given the dynamic nature of postmortem genetic testing, referral of the family for genetic counseling is recommended to ensure discussion of testing options, adequate informed consent for testing and optimal communication about test results. The role of the medical examiner is crucial to ensure collection and retention of an adequate specimen. The willingness of the medical examiner to send the specimen (with proper consent) to the genetic testing laboratory selected by the family, cardiologist, and genetic counselor is also imperative to the success of the postmortem genetic testing endeavor.
In considering the grieving family members of a decedent, the role of postmortem genetic testing in clarifying the cause of death cannot be underestimated. Of equal importance, however, is the clarification of risk for sudden death that is provided by predictive testing in at-risk family members. Once a disease-causing mutation is identified, genetic testing for that specific mutation in at-risk family members is recommended by societal guidelines (9). In order to realize the benefit of postmortem genetic testing, communication of genetic information among family members must be optimized. Genetic counselors play a central role in facilitating this communication among individuals in the postmortem setting. Return of genetic test results to the decedent's family members is often performed by the genetic counselor in collaboration with the cardiologist caring for the family. When a disease-causing mutation is identified, the genetic counselor will review the test result with the immediate family members, ensuring the proper identification of at-risk relatives for whom genetic testing is recommended. The genetic counselor can also assist in providing the family with written information, appropriate websites, and local genetic counseling resources to assist family members with the process of genetic testing. In the absence of a disease-causing mutation, at-risk family members are typically advised to undergo continuous cardiac surveillance. The option of clinical DNA banking for any remaining DNA specimen is also an important element of the posttest genetic counseling session, whether or not a mutation is identified. Gene discovery and genetic testing are expanding rapidly. Clinical DNA banking of any remaining DNA specimen may afford the ability to perform future genetic testing either related or unrelated to the decedent's cause of death. These important tasks are well suited to the genetic counselor, who is expertly positioned to assist the family of the decedent with these important elements of care. With proper permissions, the genetic counselor can also ensure that genetic test results are available to the decedent's family members, to the cardiologist (who is most often the ordering physician), and to the medical examiner, whose careful diligence in identifying hereditary cardiac conditions and collecting and retaining an appropriate specimen is the cornerstone of making postmortem genetic testing available for families.
Medical Examiner Considerations for Initiating a Regional Sudden Death Network
The formation of this multidisciplinary team has dramatically improved our comfort level as medical examiners and cardiac pathologists, providing us with a place to refer grief-stricken families, who now have the added stress of a potentially serious medical condition in other family members. This collaboration has also helped the ME community fully understand that the complex screening and genetic counseling process goes far beyond easily selecting a genetic test and receiving a result, and that the process of genetic screening is beyond the scope of ME practice. This relationship works well the other way around: we are occasionally contacted by the GAC to review autopsy reports and slides of decedents that are related to family members they are seeing in consultation. They are comfortable with our diagnoses and with our approach to these difficult cases as it essentially provides them a second review.
It is important to stress that this collaboration has no financial motive or significant burden for the parties involved. In this model, the ME offices do not bear the cost of genetic testing. As discussed above, the clinical workup of these cases may be quite complex and expensive, requiring significant resources and time commitment, which may present a challenge in initiating a local network. Our group was fortunate in that the cardiologists contacted us to form the SDN; however, this type of network could be replicated. Regional centers with established genetic arrhythmia programs do exist throughout the country, mostly in large referral hospitals. Patients may be required to travel, but in our experience, most are willing to do so if they know the care will be thorough and appropriate. If such a program does not exist in your region, it has been our experience that cardiac electrophysiologists would be the best initial contact, either pediatric or adult, as they are often familiar with the many forms of heritable cardiomyopathies and channelopathies. General cardiologists might not be as familiar with these types of conditions and the complexities of the required screening. The cardiac electrophysiologist will in turn utilize local expertise in cardiac imaging and establish relationships with genetic counselors. Electrophysiologists may be located by referencing the Heart Rhythm Society website: http://www.hrsonline.org/?gclid=CMet7KbUv8UCFVKDf-god-64AUg. Genetic counselors may be contacted at the National Society of Genetic Counselors homepage: http://nsgc.org/.
Conclusion
Resources for counseling and screening are often limited for family members of sudden cardiac death victims. These challenges can best be approached by a collaborative effort among the local medical examiners, cardiac pathologists, genetic counselors, and a specialized medical center that can provide clinical context and appropriate screening. This collaborative approach capitalizes on the strength of its component parts, where the roles are well defined among members of this network.
The medical examiner's role should be limited to recognizing potentially heritable cardiac conditions in decedents, obtaining and storing appropriate specimens and referring the family to a specialized genetic arrhythmia center or a cardiac electrophysiologist if such a program does not exist in their region. Cardiac pathology specialty referral may be of assistance in full workup and diagnosis of cardiac conditions. Choosing genetic testing panels, interpreting results, and counseling families on the meaning of genetic testing results is a complex endeavor that is best handled by genetic counselors in conjunction with specialty cardiologists.