
Abstract
Pheochromocytomas and paragangliomas are a rare cause of sudden death. We present the case of a 34-year-old male who died suddenly. He had been diagnosed as having diabetes mellitus five days previously and was hypertensive. At autopsy he had a 3.5 cm extra-adrenal mass. Histology of the tumor showed it to be a paraganglioma with the characteristic histological appearance. Postmortem biochemistry revealed a vitreous glucose of 5.9 mmol/L (106 mg/dL) with negative ketones. Urinary catecholamines were measured and revealed raised metanephrine:creatinine and normetanephrine:creatinine ratios. There may be genetic implications in patients with pheochromocytomas and paragangliomas as they are associated with a number of hereditary syndromes.
Introduction
Paraganglia are neuroendocrine cells associated with both the sympathetic and parasympathetic nervous systems. Parasympathetic paraganglia occur predominantly along the cervical and thoracic branches of the glossophrangeal and vagus nerves (1). Examples include the carotid body and the tympanic membrane. Sympathetic paraganglia are distributed in the paraxial regions of the trunk along the prevertebral and paravertebral sympatheic chains and in connective tissue in the pelvic organs (1). The most well-known location is the adrenal medulla and the other named paraganglion is the organ of Zukerkandl located at the origin of the inferior mesenteric artery. Paraganglia are present around the adrenal gland as well as the adrenal medulla. Paragangliomas are tumors of paraganglia tissue and are called pheochromocytomas when they involve the adrenal medulla, because they include chromaffin cells – they react with potassium dichromate and become a brown color due to oxidation of stored catecholamines (2). They are traditionally known as the 10% tumor: 10% being outside the adrenal gland, 10% secreting catecholamines, 10% being malignant, and 10% not associated with hypertension (2). They are also associated with hereditary syndromes including Multiple Endocrine Neoplasia (MEN) 2A and 2B and von Hippel-Lindau disease, neurofibromatosis type 1 and familial paraganglioma/pheochromocytoma syndromes. Pheochromocytomas and paragangliomas are associated with germline mutations that include NF1 (GTPase), RET (tyrosine kinase receptor), VHL (ubiquitin ligase activity), THEM127 (transmembrane protein), MAX (transcription factor) and in the succinate dehydrogenase complex (SDHA, SDHB, SDHC, SDHD and SDHAF2) (3). Histologically, the tumors are composed of cell nests—Zellballen—which stain with neuroendocrine markers and surrounding sustentacular cells, which are S100 and GFAP positive. Bizarre pleomorphic cells may be present in benign lesions and are not a predictor of malignant potential (4).
Pheochromocytomas and extra-adrenal paragangliomas are reported as a rare cause of sudden death (5-7). We present a case of a man recently diagnosed with hypertension and diabetes mellitus who collapsed and died suddenly.
Case Report
A 34-year-old male collapsed and died suddenly. He had been diagnosed as having diabetes mellitus five days previously and was hypertensive, though specific blood pressure recordings were not available for review. He was prescribed metformin, glyburide, atenolol and aspirin. His glucose concentration on the morning of his death was measured at 10 mmol/L (180 mg/dL).
At autopsy he weighed 59 kg and had a height of 163 cm. His heart weighed 410 g and there was no significant coronary artery disease. His liver weighed 2140 g and was normal on histology. Each kidney weighed 160 g and were normal on histology. The brain weighed 1350 g and was normal.
Both adrenal glands appeared normal, but on the right side there was an extra-adrenal mass, 3.5 cm in diameter, red-tan, and partially cystic with a well-defined capsule (
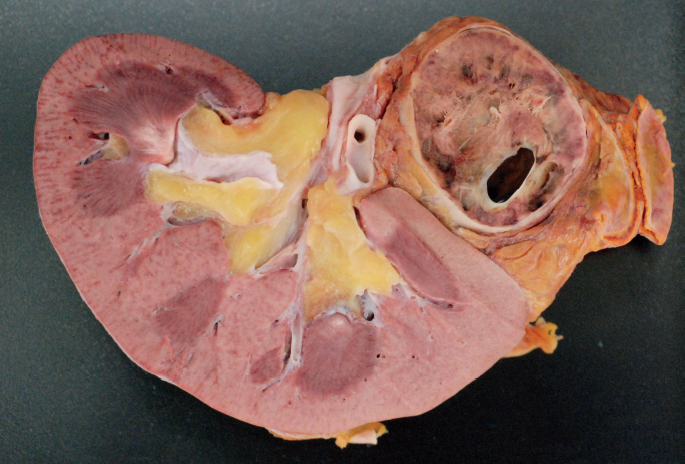
Gross appearance of extra-adrenal paraganglioma.
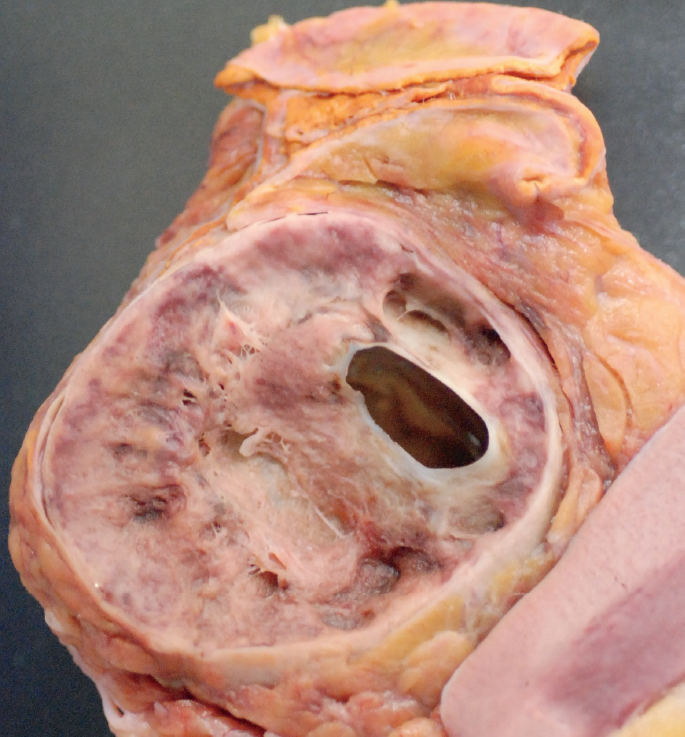
Close-up of gross appearance of extra-adrenal paraganglioma.
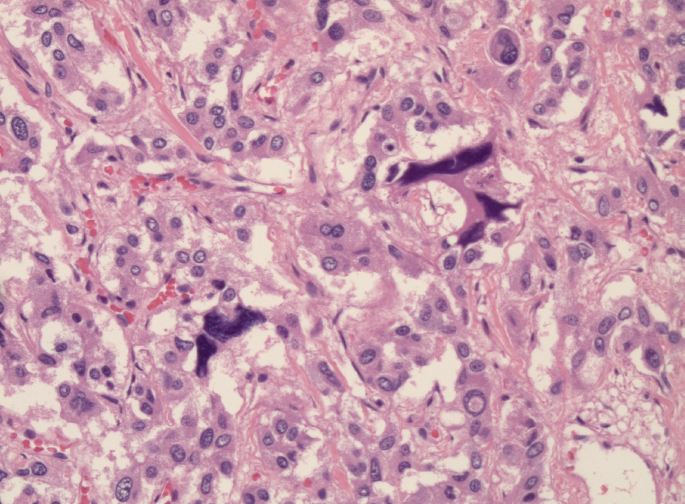
Cellular pleomorphism in a paraganglioma (H&E, x400).
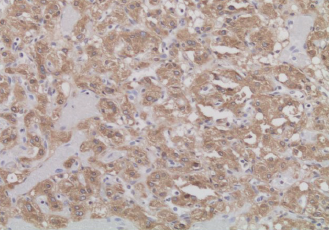
Chromogranin immunoreactivity in cells within Zellballen. (Chromogranin stain, x100).
The other endocrine organs were normal and there were no skin or subcutaneous changes.
Postmortem biochemistry revealed a vitreous glucose concentration of 5.9 mmol/L (106 mg/dL) and negative ketones. Random creatinine and urine catecholamine concentrations were examined and revealed raised ratios as follows: creatinine, 3.4 mmol/L; metanephrine, 3.49 μmol/L; normetanephrine, 11.03 μmol/L; metanephrine:creatinine ratio, 1.03 (upper limit of normal clinically 0.18); normetanephrine:creatinine ratio, 3.24 (upper limit of normal clinically 0.23).
Death was ascribed to a catecholamine secreting extra-adrenal abdominal paraganglioma.
Discussion
Adrenal pheochromoctyomas and extra-adrenal paragangliomas are rare tumors and presentation as sudden death is extremely uncommon. The mechanism of death is associated with the release of catecholamines and associated hypertension. Two thirds of catecholamine secreting tumors have paroxysmal episodes of hypertension with sudden increases in blood pressure and palpitations (2). Increased catecholamines also account for the impaired glucose tolerance and the diagnosis of diabetes mellitus.
The catecholamine secreting tumors are characteristically derived from sympathetic paraganglia, which are situated outside the head and neck in contrast to head and neck paraganglioma, which are derived from parasympathetic paraganglia and typically do not secrete catecholamines (3). Pathologic diagnosis is by the characteristic histological appearance supplemented with immunohistochemistry. It is also possible to perform urinary catecholamines. These are based upon ratios of the catecholamines metanephrine and normetanephrine compared with urinary creatinines and is a well-recognized test. At autopsy, urinary catecholamines have been measured to identify stress reactions in such deaths as hypothermia (8, 9), Clinically, urinary catecholamines are measured on a 24-hour urine analysis, but a single urine analysis has also been shown to have value and can show raised concentrations sufficient to be diagnostic (10). Urinary catecholamines in this case showed raised concentrations based upon clinical values, proving that the paraganglioma was functional in this case, accounting for the raised glucose concentration, the history of hypertension, and sudden death.