
Abstract
According to many published reports, testimonials, research studies, and data collected, there are not enough forensic pathologists to serve the United States. Forensic pathologists are responsible for the medicolegal investigation of death. Such investigation includes death scene, history, autopsy, and determining the cause and manner of death. To get an idea of the workload of the forensic pathologist, retrospective data can be examined. The numbers alone reveal that there has been and remains a shortage in the forensic pathologist workforce. If the overall goal is to remedy this forensic pathologist shortage, strategies must be broad and long-term. Also, not all goals will have concrete metrics that can be quantified, such as to increase and improve public image. Some of the underlying problems, trends, future predictions, and possible solutions are discussed.
Keywords
Introduction
Pathologists bridge the basic sciences with the practice of medicine, saving and improving the quality of lives. Forensic pathologists use the foundation of pathology not only to determine the cause and manner of death, but also to improve public safety, identify individuals, detect genetic and hereditary disorders, prevent diseases through reporting of postmortem findings, discover undiagnosed malignancies, assist law enforcement and the judicial system, and prevent crime. Such contributions need to be understood and recognized by others in order to improve the practice of forensic pathologist and ensure the quality and quantity of its workforce. Too often the public neither knows what pathology is nor that a pathologist is a physician. Pathologists, then, must be responsible to communicate and demonstrate that the autopsy is a medical procedure, an empowering resource to longer life, better quality of life, and public health and epidemiology (1). Public education encompasses elementary, high school, college, and medical school as well as funeral directors, chaplains, civic, and church and religious groups. Medicolegal death investigation and the autopsy are also important components to publicly link forensic pathologists with saving lives, advancing healthcare, and providing families with information to support health and wellness. The scientific and medical advancements attributed to the autopsy, both hospital-based and forensic, need to be conveyed to the public, hospital administration, other physicians, patients, and governmental leaders.
As of October 2015, the U.S. population was approximately 326 million (2). National data show that there is a shortage of forensic pathologists. It is up to the forensic pathologist to convey the importance of this shortage. In 2005, Congress directed the National Institute of Justice of the United States Department of Justice to contract with the National Academy of Sciences to investigate the status of forensic science in the United States. According to the National Academy of Sciences report, the U.S. has a shortage of forensic pathologist (3). Approximately 400-500 physicians practice forensic pathology full-time with an estimated need of 1000 (4-6). About 10% of available positions are vacant due to lack of available forensic pathologists or lack of funding. Major organizations such as the Consortium of Forensic Science Organizations and the National Association of Medical Examiners (NAME) have recognized this and have been working to solve the problem.
In 2013, the Department of Justice in partnership with the National Institute of Standards and Technology (NIST) established the National Commission on Forensic Science (NCFS) to enhance the practice and improved the reliability of forensic science. NIST developed the Organization for Scientific Area Committees (OSAC) to address standards and quality in specific areas. Forensic pathology falls within the Crime Scene/Death Investigation Scientific Area Committee (SAC). This SAC is the group that can address forensic pathologist supply and investigate the root and origin of this national problem.
Salaries, compensation, and funding are crucial areas that need to be addressed. Although many forensic pathologists earn $150 000-$180 000 annually, this range is much lower than the average income of more hospital-based pathologists starting at entry level (7). As of 2014, medical graduates finish school with an average debt near $180 000 (8,9). This does not include up to $30 000 of other debt such as premedical education debt. Interested physicians are less likely to choose forensic pathology as a career with low salaries and debt burden. The United States Senate and House of Representatives are drafting bills to introduce forensic science reform legislation. Such proposals could address areas such as forensic pathologist certification, accreditation, standards, needs assessment, training, operations funding, funding for continuing education, loan forgiveness, and research. There are several reasons for the forensic pathologist shortage and some will not be resolved through the government.
Discussion
Medical School
Pathology is a core subject in the training of physicians – the link between basic science and clinical medicine (10-13). Traditionally, pathology was taught as a single course in the basic science block of medical school. Since Flexner's report, “Medical Education in the United States and Canada” in 1910, the U.S. had adopted the 2+2 curriculum structure in which two years of basic science are followed by two years of clinical science (14-16). However, now many medical schools are changing their approach to the teaching of pathology. Pathology curricula include: 1) pathology taught as a stand-alone basic science course during the first two years; 2) partially integrated with other courses and taught by organ system; 3) partially integrated with other courses and taught by age, “birth to death”; 4) partially integrated with other courses and taught by disease approach; and 5) fully integrated with no stand-alone pathology course or identified pathology component. Such partial or full integration is thought to help students see the clinical relevance of the basic sciences. The goal is to break down barriers between the basic and clinical sciences currently in place as a result of traditional curricular structures (16). Unfortunately, a common flaw is that insufficient attention has been paid to the balanced integration of basic science content such as pathology especially in the third and fourth years (8,16). Pathology has gone from a foundation of medical education to a poorly understood specialty of medicine. Furthermore, with the drop in the required minimal Joint Commission on Accreditation of Healthcare Organizations hospital autopsy rate of 20%, many medical students and residents lack exposure to the autopsy (17-19). The microscope has already disappeared from most of medical education, replaced by computer images (19).
As with the lack of visibility and recognition of pathology in medical school, there is an even more dramatic lack of awareness of forensic pathology. There are 144 medical schools (2014) in the U.S., and the majority of these have little or no exposure to forensic pathology. As pathology is losing visibility and identity in medical education, forensic pathology rarely has a role in the traditional or integrated curriculum. For these medical students, a residency and career in pathology is not a common choice. For many, the television dramas are the only exposure to forensic pathology.
Residency
Graduate Medical Education (GME) funding has been frozen for 16 years and continues to be targeted for cuts in current deficit reduction packages, including President Obama's proposed 2014 budget (20). Without additional federal support, policymakers' laudable interest in expanding support of primary care could result in reducing support for specialty training such as pathology (20). The College of American Pathologists (CAP) position on the shortage of pathologists is as follows:
Increased Graduate Medical Education funding is needed to address the projected decrease in the number of pathologists over the next two decades. There is little awareness that pathology faces a shortage and needs preferential treatment for pathologists in the GME funding paradigm. The media has focused primarily on the shortage of primary care physicians; less attention has been paid to shortages in specialties (20).
CAP also reports that legislation in both the House and Senate would lift the GME funding cap and expand the number of funded residencies, including for specialties with a demonstrated shortage. All would phase in 15 000 additional Medicare-supported residency slots over five years and would set aside some percentage of the slots to shortage specialties (7).
Eighteen-thousand-seventy-eight individuals graduated medical school in 2014 and 568 (3%) chose to train in pathology. This is compared to 6698 (37%) entering internal medicine (8). Currently, there are 153 Accreditation Council for Graduate Medical Education (ACGME) pathology training programs with 597 available positions in the U.S. (21). In 2014, the postgraduate year (PGY)-1 pathology residents were 2.1% of the 27 293 PGY-1 residency slots accepted (22). Studies have shown that approximately 9% of pathology residents will drop out of their training before completion (23). The current numbers of pathologists completing training programs are substantially inadequate to compensate for the number of pathologists retiring in the next decade and a half (23). There is also concern about the recent closure of several pathology training programs, lack of funding for certain seats, and healthcare reform that might broadly cut financial support for medical education, affecting all specialties including pathology (23,24).
From 2008 to 2013, the number of pathology trainees decreased by 9.5%. As the number of pathologists decreases, the U.S., population and average life expectancy increase. The current life expectancy in the United States is 78.8 years (25). The estimated full-time employed pathologists for 2030 are 20 000. This means that to adequately serve the population, the U.S. will need 8.1% more residency positions; and they will need to be filled (23).
In 2014, after completing accredited training, 105 pathologists became certified in anatomic pathology, 65 in clinical pathology, and 495 in combined anatomic and clinical pathology. To subspecialize in forensic pathology, a resident must first complete accredited training in either anatomic pathology or combined anatomic/clinical pathology (26-28). Part of the anatomic pathology training is conductance of and competency in the autopsy procedure. Unfortunately, there has been a marked decline in the hospital-based autopsy to approximately 5% of hospital deaths (29). Medicare stopped paying directly for the autopsy in 1986, the Joint Commission dropped its minimal autopsy requirement, and the majority of physicians lost interest in the autopsy. Pathologists chose to spend their time on more lucrative diagnostic testing, and clinicians started believing that sophisticated diagnostic tests rendered the autopsy obsolete (18). The American Board of Pathology (ABP) requires only 50 autopsies be completed during training, a very minimal exposure to the procedure and to autopsy pathologists. Fewer and fewer young pathologists are familiar and competent with autopsy techniques and unable to interpret the macroscopic findings (19). The shrinking number of autopsies and reduced requirement for pathology training has contributed to a reduction in requisite expertise (18). Many pathology training programs must rely on forensic centers and forensic pathologists to train residents in autopsy pathology. Hospital-based autopsies referred to forensic centers and forensic autopsies performed by forensic pathologists are often the only training in autopsy pathology and contact a resident has with a forensic pathologist. The ACGME recommends that all anatomic pathology training programs provide their residents with exposure to forensic pathology. This requirement is not always being met. There is no requirement for a rotation, didactic curriculum, or other training in forensic pathology for the pathology resident.
Fellowship
There are 37 (39 as of 2016) ACGME-Accredited Forensic Pathology Programs in the United States. Among these there are 78 approved training positions but only 54 (69%) of those are actually funded. Of the 54 funded positions, 42 (81%) are filled. Seven of the programs (19% of programs) have no fellow this year. The United States averages only 41 pathologists training in forensic pathology each year. Although by 2016, the U.S. will have two additional training programs, at this point the current training positions are not even filled (30). For the aforementioned reasons and others to be described below, pathologists are not pursuing a career in forensic pathology.
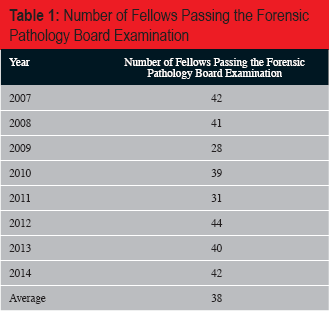
The ABP first offered forensic pathology board-certification in 1959 (31). In 2014, 42 ACGME forensic pathology fellows passed the forensic pathology board examination, a passage rate of 89% (26,27). Only an approximate average of 38 forensic pathologists entering the workforce each year
Number of Fellows Passing the Forensic Pathology Board Examination
Practice
In 2014, there were 13 710 practicing pathologists in the United States (8). Thirty-nine point three percent were under the age of 55 years, and 60.7% were 55 years of age or older. When looking at pathologists practicing from 2008 to 2013, the number is down 10.4%. Data from public domain sources on pathologists' retirement ages do not exist (23). The 2013 CAP workforce study reported that the average age at which pathologists plan to retire is 66.5 years (23). Pathologists older than 55 years report an average age of retirement of approximately 71 years (23). In 2015, it is predicted that 470 pathologists will retire, approximating 3-4%; retirees will exceed the number entering the workforce. The anticipated overall pathology retirement will peak in 2021 (23).
Now, to examine the data for forensic pathologists: the 2014 Practice Characteristics Survey Report by CAP reported that 11% of board-certified pathologists practice forensic pathology, but only 4% do so full-time (7). What is not documented is whether or not these pathologists are board-certified in forensic pathology (7). Each year, 30-40 individuals complete forensic pathology training and sit for the board-certification examination (6,27). Although some pathology residents choose and complete a forensic pathology training program, only two-thirds practice forensic pathology full-time. Only approximately 400-500 practicing forensic pathologists are in the U.S. Forensic pathologist retirement data are not known. If one applies the retirement of 3-4% to the specialty of forensic pathology for 2015, this would be somewhere around 12-20 retirees. A projected loss must also include the number of forensic pathologists who decide to drop out of the profession. Retention of forensic pathologists within the field is also an issue that needs to be addressed (17).
In 2004, there were approximately 2000 medical examiner and coroner offices in the U.S. (1600 coroner, 400 medical examiner) and approximately 400 practicing forensic pathologists (4). In 2004, 2 398 000 people died in the U.S. Approximately one million of these cases were referred to the medical examiner/coroner (ME/C) offices, 40% of all deaths. Depending on circumstances, 51% (almost half a million) of these were accepted for medicolegal investigation (5). The most recent U.S. vital statics are from 2013. At the end of 2013, the U.S. population was 320 050 716 (25). That year, 2 596 993 deaths occurred (25). Most deaths were from natural causes, but deaths due to injury/trauma (homicide, suicide, accident, and undetermined manner) were 192 945. It is estimated that 90% of all traumatic or suspicious deaths should be autopsied. Further, at least 50% of cases handled by most medicolegal offices are sudden, unexpected natural deaths, and about 33% of which require autopsy to identify the specific causes of death. An estimated 1.5 million were referred to ME/C offices in 2013. It is probable that many of the cases needed a medicolegal investigation and autopsy. Even if some cases were only examined by a coroner (nonforensic pathologist), it is unreasonable to assume that 400-500 forensic pathologists could handle the remaining workload. Review of NAME Inspection and Accreditation data and previously collected facility data show that ME/C officer operating at an acceptable level of autopsy performance annually perform approximately one autopsy per 1000 persons (32). A forensic pathologist caseload should not exceed 250 autopsies per pathologist per year. Therefore, with a U.S. population of approximately 320 million, a projected 1280 forensic pathologists are needed. It is irrational to think that such an excessive workload will not directly and seriously affect the quality of work or significantly endanger the welfare of the public or personnel (33). NAME recommends that each forensic pathologist perform no more than 250 autopsies per year (33). Unfortunately, the U.S. has an increased number of medicolegal/forensic cases with a short supply of forensic pathologists who should not perform more than 250 forensic autopsies per year.
Approximately one-third of forensic pathologists drop out of the field. The practicing forensic pathologist is often frustrated and dissatisfied due to the inability to practice quality forensic pathology and conduct medicolegal death investigations due to lack of funding for facilities, continuing education, and research; uncompensated time and for deposition and courtroom testimony; the burden of increasing medicolegal death investigations with a small workforce; and competition with noncertified pathologists who conduct autopsies for a lower fee. Furthermore, the salaries of forensic pathologists are significantly lower than other physicians and other pathologists. To recruit and retain individuals in the field of forensic pathology, we must make forensic pathology salaries more competitive with hospital/academic pathology and other medical specialties. A survey by CAP revealed that the average compensation of full-time pathologists is approximately $333 889 annually when base salary, incentive pay, deferred compensation, and other income are considered (7). In comparison, a study by Kemp recently showed that the average salary of a medical examiner is just under $185 000 (34). The salary is only slightly better for Chief and Deputy Chief Medical Examiners who have average annual incomes of approximately $220 000 and $190 000, respectively (34).
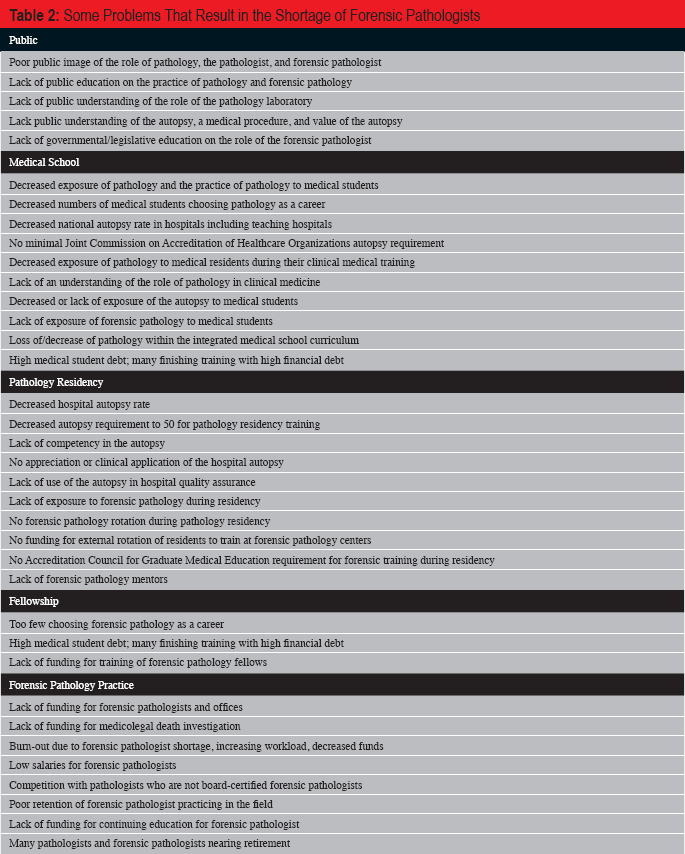
Some problems that result in the shortage of forensic pathologists is summarized in
Some Problems That Result in the Shortage of Forensic Pathologists
Conclusion
A shortage of pathologists and forensic pathologists definitely exists within the U.S. A study of the potential reasons beginning with public perception on through medical school, pathology residency, pathology fellowship, and into forensic pathology practice, exposes recurring themes. Poor public image of the forensic pathologist exists. Who is a forensic pathologist? Is the autopsy a medical procedure? The public includes citizens, future doctors, and governmental/legislative individuals. If we are not visible then we cannot be understood. If we are not understood or appreciated then we cannot expect changes in funding and legislation. The “death” of pathology in medical school will make it virtually impossible for medical students to consider pathology as a career. Pathology must be uncovered and revealed as the foundation of medicine and the link between the basic sciences and clinical medicine. Pathology must be reintroduced with a weight in the medical school curriculum. The value of the autopsy needs to be conveyed in the training hospital. All specialties and residencies need to realize the antemortem and postmortem discrepancies discovered by the autopsy, the value of the autopsy in treating future patients, and the role of the autopsy in overall hospital quality assurance and improvement. It is up to the pathologist to resurrect the important role of the autopsy. The pathology resident needs to have more exposure to autopsies and the use of the autopsy results. The American Board of Pathology should not decrease the number of autopsies required for board-certification eligibility. Residency training programs need to affiliate with local forensic centers if hospital-based autopsy numbers are not sufficient for their residency training program. Local forensic centers should welcome these trainees. The ACGME needs to require a specific block of time and curriculum for forensic training during anatomic pathology residency. Forensic pathologists need to take this time to serve as mentors. Finally, the financial and governmental/legislative issues must be appreciated. With the student loan burden and low forensic pathology salaries, student loan forgiveness should be considered. Funding for training and for forensic pathology offices and death investigation must be appropriated. Forensic pathologists need to realize that if they are not seated at the table with those at NIST, NCFS, OSAC, and others, then they cannot and will not be heard. If forensic pathologists do not advocate with legislation, then they will have no input on national standards, medicolegal death investigation, accreditation, certification, or forensic science funding. Forensic pathologists must address these issues at all levels in order to provide not only quantity but also high quality of individuals entering the field of forensic pathology.
Footnotes
The author has indicated that she does not have financial relationships to disclose that are relevant to this manuscript