
Abstract
Medical examiners are physicians tasked with conducting medicolegal death investigations to determine cause and manner of death. Although the autopsy is the most frequent tool utilized in these investigations and the one most often associated with the practice of forensic pathology, there is a wide variety of tools available to the medical examiner, whose statutory duty mandates death certification. We discuss the evidence supporting the usage of these myriad tools, ranging from the older techniques of scene investigation, microbial cultures, and toxicology to the cutting edge of medicine such as advanced imaging, molecular genetic studies, and biochemical analysis/metabolic testing. The forensic pathologist must select the correct tools for a particular investigation based on the evidence supporting their usage and a medical judgment of each tool's pretest probability to produce a useful result, its appropriateness for the case, and the resources required for its utilization. The incorporation of these techniques into the forensic pathologist's toolbox improves our ability to conduct thorough medicolegal death investigations beyond that which can be accomplished by invasive autopsy alone.
Keywords
Introduction
Forensic pathology is defined by the College of American Pathologists as
the subspecialty of pathology that directs its efforts to the examination of living or dead persons in order to provide an opinion concerning the cause, mechanism, and manner of disease, injury or death (1).
In a medical examiner system, the forensic pathologist is responsible for death certification, which the National Association of Medical Examiners (NAME) describes as “a process that integrates clinical, circumstantial and death scene information, autopsy findings, and other laboratory findings” (2). The forensic pathologist is thus an investigator who is charged with gathering the facts surrounding a death, interpreting their importance, and coming to a reasonable conclusion regarding cause and manner of death (3). This reasonable conclusion represents the forensic pathologist's opinion on what the most likely cause of death is; the expectation of the degree of certainty required in making this determination may vary by jurisdiction and individual. Indeed, even in coroner systems, the forensic pathologist often performs the same functions and advises the coroner. Regardless, most forensic pathology fellowship programs are focused on training new practitioners in the medical examiner model.
Comprehensive medicolegal death investigation is not limited to the autopsy alone (3); while the autopsy is a powerful tool and the one most commonly associated with a forensic pathologist's identity, relying on the autopsy in the absence of other data sources or viewing the autopsy as the only tool may lead to erroneous conclusions. The final interpretation of the findings in any case must always be considered within the context of the case as a whole. In other words, the forensic pathologist must consider the circumstances surrounding death, the decedent's relevant social and medical history, as well as any data derived from ancillary laboratory studies prior to forming any conclusions (3).
In order to gather adequate data in the conduction of a comprehensive medicolegal death investigation, the forensic pathologist has at his/her disposal a variety of tools. These tools range from the simple and inexpensive to the cutting edge of medical technology. As Assistant Attorney General David Kris remarked in an address regarding law enforcement methods in counterterrorism,
we need to use all available tools that are consistent with the laws and our values, selecting in any case the tool that is best under the circumstances (4).
Like physicians in other disciplines, however, forensic pathologists sometimes become pigeonholed into one particular tool or technique — the autopsy. For example, when asked what we do for a living, it is almost second nature to reply, “I'm a forensic pathologist — I do autopsies.” While that answer is reasonable for social situations and certainly is a valid descriptor at the most basic level, it is very easy to become trapped in that mode of thinking. What we actually do is investigate deaths and come to conclusions regarding cause and manner of death. An autopsy is simply one of the many tools — and indeed, one of the most common tools — that we use in order to fulfill our professional obligations. Depending too much on one particular technique, especially at the expense of not taking advantage of other more modern techniques that may augment or supplant it, is detrimental. An overreliance on one particular tool has historically been called “the law of the instrument: Give a small boy a hammer, and he will find that everything he encounters needs pounding” (5). This concept was modified by Maslow as follows: “I suppose it is tempting, if the only tool you have is a hammer, to treat everything as if it were a nail” (6). During the early days of forensic pathology, an autopsy really was the only tool that forensic pathologists had. It was their hammer. This is no longer the case; forensic pathologists now have access to other, very powerful tools; we have much more than just a hammer. These tools often allow for an increased degree of medical and/or scientific certainty in the determination of cause of death over autopsy examination alone. In addition to their utility in arriving at a reasonable diagnosis, many of these tools aid in preserving data, thus serving a role in the forensic aspect of the investigation. The notion that the autopsy is (or should be) the primary tool in our toolbox may no longer always be correct or appropriate in every case.
In this article, we discuss some of the tools available to the forensic pathologist in the conduction of a medicolegal death investigation besides the autopsy, including recent and cutting edge techniques and the evidence demonstrating their utility. We also discuss the appropriate and inappropriate applications for these tools.
Discussion
The Tools in the Toolbox
Autopsy
The autopsy, intended here to mean the external and internal examination of the body, is perhaps the most utilized tool in the forensic pathologist's toolbox, and with good reason: it is the gold standard in identifying disease and injury in order to determine cause of death. As such, the autopsy has become the “hammer.” This is almost certainly why we forensic pathologists identify with this tool so closely. The term “complete autopsy” is an elusive one; what constitutes a complete autopsy has been discussed elsewhere and is summarized as follows:
… an autopsy can be said to be complete when it allows for the accurate determination of cause and manner of death (statutory duty), when it facilitates the collection and documentation of evidence and determines the underlying nature of disease or injury (creation of a minimal dataset for societal and governmental inquiry), and allows practitioners to obtain and maintain experience with a broad variety of case material relevant to daily practice, and of value in the interpretation of complex cases (maintenance of competency) (7).
And the autopsy, of course, is one tool that is exclusively “owned” by forensic pathologists. There is a potential danger, however, in the continued reliance on one particular tool when new tools come about that can potentially make our jobs more time- and cost-efficient.
Scene/Investigation
Some of the simplest and oldest tools used for investigation are often the most critical ones to utilize in a medicolegal death investigation. Consider the hypothetical case of a truck driver found deceased in his overturned vehicle who had no lethal injuries evident at autopsy. The scene investigation revealed that the driver's head and neck were buried within soft dirt, inhibiting the decedent's ability to breathe. The correct determination of the cause of death in this case relied on interpretation of photographs of the scene, one of the oldest and simplest investigative tools. Consider also the hypothetical case of an elderly male found unresponsive in bed who expired in the hospital after toxicological screen and subsequent quantitative toxicology revealed a high concentration of hydrocodone. A phone call to the decedent's daughter revealed that he had recently stated his intentions to take his own life on the anniversary of his wife's death, which was the day he was found unresponsive. In this case, the manner of death is correctly determined based on a phone call. These basic investigative tools often prove crucial to the forensic pathologist in determining cause and manner of death.
Advanced Imaging Techniques
In many cases it may be appropriate to consider a more advanced tool. In recent years, there has been an explosive increase in publications describing potential uses for advanced imaging techniques in forensic pathology. As with any new technology, concerns have been expressed regarding what the impact of postmortem imaging will be on the practice of forensic pathology (8). However, the utility of these imaging techniques is becoming increasingly clear based on the myriad case reports and systematic reviews in the medical literature. It is most likely that postmortem imaging will become (and is becoming) an incredibly useful tool to use as an adjunct to autopsy, with some cases in which it either has no utility at all and some cases in which it would suffice as an alternative to autopsy
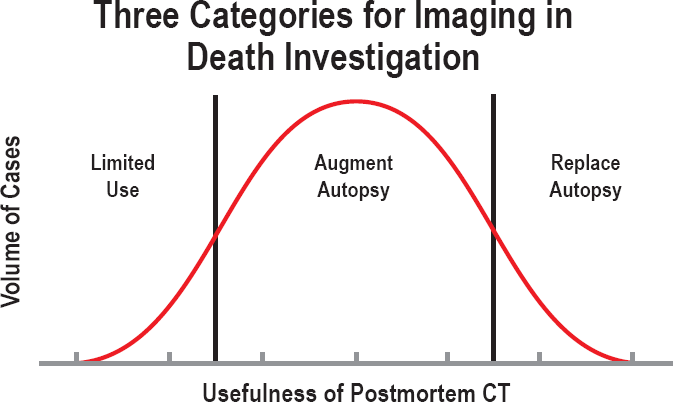
Categories for imaging in death investigation.
There has been concern that postmortem imaging is insufficient to document injuries in trauma. A study in 2007 demonstrated that antemortem computed tomography (CT) scans had low sensitivity for detecting traumatic injuries, particularly of the head and neck (9). This study compared results of antemortem CT scans performed within 24 hours prior to death to results from subsequent conventional autopsy. It is important to note that postmortem CT (PMCT) is substantially different from antemortem, clinical CT. Because the subjects are deceased, there are no concerns for the amount of radiation exposure and because of this, the images are strikingly more detailed than CT images obtained during life. Furthermore, postmortem imaging studies are not subject to motion artifact. Recent studies have compared the results of postmortem imaging techniques to conventional autopsy (10-17). These studies suggest that postmortem imaging sensitivities are increasing. A large systematic review of validation studies comparing noninvasive and minimally invasive postmortem imaging techniques with conventional autopsy demonstrated sensitivities for cause of death ranging from 20% to 100% and agreement on cause of death ranging from 27.3% to 100% for imaging only modalities (18). When combined with minimally invasive methods (such as postmortem CT-guided biopsy), the sensitivities increased to 89.5% to 94.7% with agreement on cause of death ranging from 76.7% to 93.8% (18).
Specialized postmortem imaging techniques may serve an increasingly useful role in particular cases. CT angiography has been demonstrated to have utility in the evaluation of coronary artery disease, with a correlation rate of 80% with traditional autopsy dissection techniques (10). CT angiography has also demonstrated utility in the diagnosis of other traumatic and nontraumatic vascular diseases, including lesions of the cerebral vasculature, dissection or rupture of the internal carotid and vertebral arteries, pulmonary embolism, and aortic vascular pathology, to name a few. This technique provides added value, particularly in those cases for which traditional autopsy dissection is limited or challenging.
While magnetic resonance imaging (MRI) in general is more expensive than CT imaging (18), it may have utility in the examination of fetuses. A study comparing postmortem magnetic resonance (PMMR) to conventional autopsy revealed a sensitivity and specificity for final cause of death in fetuses of 69% and 95% respectively as opposed to 28% and 64% in children and adults (19). PMMR is also superior to PMCT in the evaluation of pathological fluid accumulations (e.g., hematomas, bone contusions, and organ lacerations) and may have the added benefit of possibly highlighting early myocardial ischemia. Along with PMCT, PMMR has proven useful in the evaluation and documentation of pulmonary edema and other primary and secondary pulmonary pathologies, as well as the interpretation of brain pathology within the context of variably severe forms of putrefactive decomposition (20).
Proponents of postmortem imaging techniques point out the many advantages of these non- to minimally-invasive techniques: in cases where there is a familial or cultural objection to autopsy, imaging provides a noninvasive alternative that may be more acceptable. Imaging studies can be performed without the disruption or destruction of anatomic structures, which may result in loss of evidence (21). Furthermore, imaging studies produce records which may be reviewed indefinitely, allowing for additional consultations long after the body has been released (18,21).
Despite the many potential advantages of postmortem imaging, there are multiple concerns about its implementation into forensic pathology practice. One such concern is the overall cost required to implement these modalities. Certainly the purchase of a CT or MRI scanner dedicated for postmortem imaging is not insignificant; however, a viable option is to purchase refurbished scanners at a discount (21). Some studies have suggested that the implementation of CT angiography requires an expensive heart-lung machine for the distribution of contrast material; however, simpler alternatives requiring a roller pump with a controllable contrast flow rate cost significantly less at approximately $3000 (21). As Roberts et al. described, the consumables required for CT angiography cost approximately $30 per decedent (10). One study comparing minimally invasive autopsy to conventional autopsy calculated that the former cost on average $1497 while the latter cost $2274 (22). While a dedicated CT scanner for forensic cases is certainly ideal, an alternative strategy is to employ the use of a hospital CT scanner during off-hours for postmortem studies, obviating the need for an office to purchase a separate scanning instrument. Perhaps the largest potential for imaging to represent a cost-saving investment is in its use as a pre-autopsy screen; if a cause of death such as aortic dissection or massive intracranial hemorrhage is identified prior to conventional autopsy, the costs and labor of performing a conventional autopsy can be avoided (16).
The argument can be made that there is value in documenting all traumatic injuries (including those that may be missed by imaging techniques), and not just documenting injuries sufficient to account for death. There is frequently educational value in performing an autopsy to discover all of these traumatic injuries, both to pathologists in training and to the clinicians who care for these patients prior to their death. However, there is a distinction between the jurisdictional responsibilities of the medical examiner and the educational duties of the pathologist. In medicolegal jurisdictions, the medical examiner is charged with providing “an opinion concerning the cause, mechanism, and manner of disease, injury or death” (1); if this opinion can be determined without an autopsy, it may constitute an overreach of one's jurisdiction to perform one for educational purposes. Certainly in those jurisdictions where resources are limited, it may be considered by some as a breach of public stewardship to expend the resources necessary to perform a conventional autopsy when an external examination with imaging would suffice.
The National Association of Medical Examiners' autopsy standards state that a forensic autopsy should be performed if “the deceased is involved in a motor vehicle incident and an autopsy is necessary to document injuries and/or determine the cause of death” (23). However, if injuries have been documented prior to death in the hospital setting, many offices will not perform an autopsy and will determine the cause of death based on an external examination in conjunction with hospital records, which have often documented injuries based on antemortem imaging. This approach satisfies the duty of the forensic pathologist to conduct an investigation to determine cause/manner of death, and is in compliance with the NAME standards. If fatal injuries documented by antemortem imaging are sufficient to determine cause and manner of death, why should fatal injuries detected by postmortem imaging be any different?
Another concern is the qualifications of forensic pathologists in interpreting postmortem imaging; forensic pathologists are not radiologists. However, the same argument can be made for forensic pathologists interpreting conventional radiographs, a practice which is routine. Similarly, forensic pathologists frequently interpret the results of postmortem toxicology. One need not be a toxicologist to recognize a lethal concentration of oxycodone, just as one need not be a forensic radiologist to recognize an intracranial hemorrhage or atlanto-occipital dislocation on postmortem CT.
Molecular Genetic Studies
Another new technology with the potential to become a routine tool in the forensic pathologist's toolbox is genetic testing, following the explosive advances in molecular techniques. As molecular studies become increasingly rapid and inexpensive, their utilization in forensic investigations has become increasingly prevalent. Genetic testing has become a routine tool in the investigation of sudden unexpected deaths. In fact, a NAME position paper and the NAME Autopsy Standards currently advise the collection of blood or other appropriate specimens at autopsy “for potential genetic testing in sudden, unexplained deaths that remain unexplained at the completion of the autopsy” (23,24). Recent studies have suggested that pathogenic mutations may be identified in up to 30% of cases of sudden unexplained deaths (25).
To date, molecular studies at autopsy are most frequently used in cases of suspected sudden cardiac deaths in individuals less than 40 years of age. This is a function of several factors: 1) many fatal cardiac diseases may have no or minimal gross or microscopic findings at autopsy (26); 2) there are multiple specific pathogenic mutations implicated in conditions presenting with sudden cardiac death (26,27); and 3) many of these conditions are heritable and hence appropriate counseling of surviving family members is beneficial (28).
Testing for genetic mutations implicated in sudden cardiac death has typically been performed via targeted mutational analysis using sequence-specific primers to identify a selected panel of mutations, particularly those implicated in cardiac channelopathies (29). Recently, advances in massive parallel sequencing (also known as next generation sequencing) have resulted in the identification of hundreds of potential pathogenic mutations. Reductions in the time and cost required to perform these techniques have made whole exome sequencing and even whole genome sequencing potential tools for the forensic pathologist (26,30,31).
Given the complexity of interpretation of molecular results, the constantly expanding test methodologies available, and the potential need for extensive workup and counseling of surviving family members, a multidisciplinary team approach is ideal for cases of potential heritable conditions. A recent article provides an excellent summary of such a team approach to sudden cardiac deaths utilized in Minnesota involving forensic pathologists, cardiovascular pathologists, cardiologists, and genetic counselors, among others (32). The role of the forensic pathologist is to identify potential cases of heritable conditions, collect appropriate specimens for testing, document relevant autopsy findings (including consultation with cardiovascular pathologists when appropriate), and alert family members to the possibility of a heritable condition and initiate referral to genetic specialists (32-34).
Postmortem Cultures
Postmortem microbiological cultures are rife with potential pitfalls. Their utility in death investigation has been controversial since the early 19th century, and there are currently no specific standards addressing when they should be collected and what specific cultures should be performed (35). One particularly influential study demonstrated that postmortem blood culture results were in agreement with antemortem results in only 35% of cases, suggesting that postmortem blood cultures demonstrated little utility (36). However, in select cases, this postmortem investigative tool may provide useful information. Certain symptoms should raise the index of suspicion for a previously undiagnosed infectious death; flu-like symptoms, fever with respiratory symptoms, and encephalopathy or new onset seizures have been demonstrated to have a high positive predictive value for fatal infections (37). Postmortem cultures may also be beneficial in the confirmation of an antemortem diagnosis or to provide additional information as to the extent and severity of a previously identified infection (35).
The selection of appropriate specimens for culture is critical. Specimens obtained from a site exhibiting evidence of infection (e.g., purulence, granulomatous inflammation) are more likely to yield useful results (38). Blood, cerebrospinal fluid, and lung tissue are the samples most commonly collected. Studies have demonstrated that appropriate precautions to avoid contamination at the time of collection results in a majority of cultures demonstrating no growth and a minority of cultures demonstrating mixed growth (39,40).
As with any other testing modality, the interpretation of postmortem culture results must be performed in conjunction with other findings. Positive blood cultures must be interpreted in the context of the organism identified, whether this organism was isolated alone or in conjunction with other microbial growth, and the decedent's history and circumstances surrounding death (38). The postmortem interval is also critical to consider in the interpretation of culture results; bacterial growth isolated in culture increases proportionally to the postmortem interval, and as such cultures should be collected within 24 to 48 hours following death (35). Additional ancillary studies such as immunohistochemistry and molecular testing may prove useful to corroborate results obtained by culture. A positive culture result without a gross or microscopic pathologic correlate identified at autopsy almost certainly does not represent the cause of death, let alone real pathology. Unfortunately, routine cultures in autopsy cases are often performed, especially in infants, based on tradition or office policy.
Biochemical Analysis/Metabolic Testing
The investigation of sudden unexpected infant deaths (SUID) includes consideration of inborn errors of metabolism (IEM), some of which may initially present as sudden death. These disorders comprise a varied group including fatty acid oxidation defects, organic acidurias, congenital adrenal hyperplasia, galactosemia, congenital hypothyroidism, and biotinidase deficiency.
Screening for these diseases can be performed by tandem mass spectrometry using postmortem blood and/or bile dried on a filter paper (41). A large retrospective review of sudden unexpected infant deaths demonstrated that fatty acid oxidation disorders were detected using this testing modality in 2% of these cases (42). However, the positive predictive value (PPV) and negative predictive value (NPV) of this testing modality has not been established. Furthermore, interpretation of these results is limited by several factors; results of this testing are influenced by the postmortem interval, body mass index, and liver weight (42). Additionally, the spectrum of inborn errors of metabolism is vast and many forms of these diseases are not routinely assessed using this methodology.
A recent study evaluating the utility of postmortem blood and bile screening by tandem mass spectrometry in 135 sudden unexpected infant death cases revealed nine false positive screening results, two false negative screening results, one true positive screening result, and 123 true negative screening results, corresponding to a sensitivity of 0.333, specificity of 0.932, PPV of 0.1, and NPV of 0.984 (43). Based on these findings, the authors of this study advised that routine screening for IEM in SUID cases is not recommended. Rather, screening should be performed in cases with other findings concerning for IEM including recent symptoms (recent vomiting, seizures, jaundice, etc.) and autopsy findings (cardiomegaly, hepatomegaly, accumulation of fat within viscera).
Toxicology
Forensic toxicology is an invaluable tool, but one that must never be used in isolation. Postmortem drug concentrations must be interpreted in the context of decedent characteristics, the history and circumstances surrounding death, scene information, and findings at autopsy (44).
As there is no universal test that detects all potential poisons and drugs, the selection of which specimens to collect for toxicological analysis and which analyses to perform depends greatly on investigative findings. The decedent's occupation may point to potential exposure of unusual chemicals (45). Physical characteristics of the body may point to certain intoxicants: characteristic discoloration of the body or unusual odors may suggest the toxic effects of chemicals such as carbon monoxide or cyanide. Gross or microscopic findings at autopsy may also provide useful clues to direct further testing: renal papillary necrosis may suggest aspirin toxicity, and the presence of a foam cone at the nose and mouth may indicate intoxication with heroin or opiate narcotics (44).
The collection of appropriate specimens for analysis is critical in obtaining useful toxicological data. Blood obtained from peripheral sites such as the femoral vein is recommended for quantitative analysis, while blood obtained from the heart is suitable for qualitative analysis or screening. Urine collection is also routine given that many drugs and metabolites may be detected for a longer period of time and are present in larger concentrations in urine than in the blood. Vitreous humor may be useful in cases of severe trauma, putrefaction, or environmental exposure since this specimen is relatively resistant to these changes. While liver was routinely collected historically for toxicological analysis, its collection is no longer recommended given the increased sensitivity of detection of blood testing, with rare exception (45). Stomach contents may provide value in cases of tablet ingestion, as large amounts of unabsorbed drug may be detected. However, it is important to remember that the concentration in the blood is almost always the most important factor in determining whether the drug caused death. Hair specimens may be useful to demonstrate chronicity of drug abuse, and muscle tissue may provide benefit in cases where the body has been charred or embalmed (46).
There are currently no defined standards regarding what testing should be performed for an individual case; this decision is at the discretion of the forensic pathologist in conjunction with the toxicology laboratory. The NAME Forensic Autopsy Performance Standards require that the forensic pathologist have access to toxicology testing; include the source of sample, type of screen, test results, and method of analysis in the toxicology report; and perform a forensic autopsy in deaths “by apparent intoxication by alcohol, drugs, or poison,” (23) but provide no indication of what testing is required. Various authors have suggested testing strategies such as using urine dipstick drug screens in cases of natural disease versus drug-related deaths (47), routine urine drug screen and blood ethanol screen in non-natural deaths, and the preceding plus blood drug screen with quantification in undetermined or pending manners of death (48). The ultimate determination of what testing should be performed is dependent on the specifics of the individual case and the expert opinion of the investigating forensic pathologist.
The forensic pathologist must be cautious in the interpretation of the results of toxicological analysis given the challenges inherent to postmortem testing. In death investigation, the time of ingestion and amount consumed are rarely known. Standard toxicology texts rarely account for postmortem artifacts, other significant medical conditions, drug tolerance, or other factors that may affect drug concentration or physiologic effect (44).
Selection of Appropriate Tools
All of the preceding tools have useful applications for the forensic pathologist in certain cases. The selection of the appropriate tools to use in a particular death investigation is dependent on three factors: 1) the pretest probability that the tool will produce useful results, 2) the appropriateness of the tool for the case, and 3) the resources required to utilize the tool.
Pretest Probability
The conduction of a medicolegal death investigation by a forensic pathologist involves examination of the scene, evaluation of the decedent's past medical and social history, postmortem examination, and special tests (e.g., toxicology, imaging). As such, it is the practice of medicine; this position is emphatically supported by the National Association of Medical Examiners (2). The same principles that apply to the internal medicine clinician in selecting the appropriate workup to diagnose a medical condition also apply to the forensic pathologist selecting the appropriate techniques to utilize in the determination of cause and manner of death. This selection involves a consideration of the pretest probability of a certain condition and the sensitivity, specificity, and positive and negative predictive values of a given test. This is the clinical pathology foundation of forensic pathology.
The “shotgun approach” to medicine (ordering a multitude of tests in the hopes that one will return a useful result) violates the principles of good clinical judgment in a medical workup, but unfortunately is prevalent in many aspects of forensic pathology. Perhaps the most notable example is in the workup of a sudden unexpected infant death, in which countless tests including screening for inborn errors of metabolism, a myriad of cultures (sometimes the collection of which is mandated by law) (49), and genetic testing may be undertaken. The shotgun approach is at best a misuse of resources and at worst may result in potentially misleading false positives that create more confusion than clarity. As previously described, studies have demonstrated that screening for inborn errors of metabolism (43) and infectious etiologies of death (36-38) are beneficial only in cases where the decedent's history or findings at autopsy suggest abnormalities pointing to these etiologies; in other words, cases in which the pretest probability of finding an abnormality is high.
The shotgun approach is considered unthinkable and is actively discouraged in clinical medicine; it should be no different in forensic pathology. While there may be pressure in some cases to arrive at a conclusion regarding cause of death within a short time frame, the practice of ordering of multiple tests unlikely to yield useful information at once should be discouraged.
Appropriateness
Another important consideration in the selection of a tool is its appropriateness for a particular case. A wrench can be used as a hammer, but that's not what it's for. For example, atherosclerotic cardiovascular disease in a 90-year-old male can be diagnosed with postmortem coronary angiography, but a review of medical records demonstrating longstanding hypercholesterolemia and a prior myocardial infarction is a far more reasonable and responsible approach. The medical literature is rife with examples of the utilization of complicated and/or expensive tools in situations where a simpler tool would be more appropriate (50,51).
In cases of natural deaths in which the decedent had a potentially fatal natural disease, the primary care physician (PCP) is expected to complete the death certificate as the final act of caring for his/her patient. However, it is not an uncommon occurrence that the PCP will refuse to perform this function. Medical examiner law in some states dictates the forwarding of these cases to the medical examiner's office. Some offices may choose to conduct a conventional autopsy in these cases. The selection of the conventional autopsy as a tool for the investigation of these deaths is often unnecessary and may represent using the hammer to pound things that are not nails. Why would an autopsy be necessary in cases where the PCP refuses to sign the death certificate but unnecessary in cases where the PCP agrees to sign the death certificate? If the decedent had a documented medical history of a potentially fatal natural disease, a thorough review of the medical records should be sufficient in the certification of these deaths.
An air compressor-powered nailer is an excellent tool for putting a roof on a house, but hardly needed for putting a picture hanger on the wall. A recent study demonstrated statistically significant differences in the tandem mass spectrometry (TMS) profiles of blood and/or bile in cases of sudden unexpected infant death with histological evidence of infection versus those with isolated positive culture results or no findings following autopsy, suggesting that TMS may be useful for identifying infection (52). However, this tool did not provide any additional information beyond that discovered by histology, and therefore would not be an appropriate selection in the workup of a suspected infectious death.
Similarly, although there are many potential uses for postmortem imaging, there is a problematic trend in the literature to suggest utilizing these tools in situations where a simpler tool would suffice. Recent articles have suggested the utility of postmortem CT angiography in cases of death due to falls from great heights (50) or in deaths due to other sources of trauma or massive bleeding (51,53). However, fatal injuries were evident in these cases either by conventional antemortem CT imaging or by autopsy, making the additional time and resources required to perform postmortem CT angiography unnecessary for the determination of cause of death. Postmortem imaging is a valuable tool for forensic pathologists, but as with any tool, there are situations in which it is useful and situations in which it should remain in the toolbox.
Resource Utilization
An additional major consideration in the selection of appropriate tools for a given investigation is the resources required. These resources include the monetary cost, time requirement, expertise needed, and tissues/fluids necessary to perform a particular test. As each office is unique in its budgetary constraints, access to various experts, and personnel available, the decision of which tests are desirable and feasible to employ in a particular case is variable depending on the office. Similarly, cases in which fluids are scant (e.g., infant deaths, bodies in states of advanced decomposition) necessitate careful selection and prioritization of the optimal tools.
One of the unfortunate realities facing many medical examiner offices is a limited (and often inadequate) budget. Many of the tools described above are expensive; a recent article describing whole exome sequencing to search for heritable cardiac conditions estimated a cost of $1528 per case (31). For many of these other tools, including advanced imaging techniques, a determination of the cost per case varies depending on a number of variables (see “Advanced Imaging Techniques” section above).
Although the cost of advanced imaging techniques may make this tool seem unfeasible for some offices, the savings of the time required for certain cases should not be ignored. A common constraint in many medical examiners' offices is a limited number of forensic pathologists available to distribute the caseload. As previously discussed, if a postmortem CT scan demonstrates fatal injuries, there may be no need to perform an autopsy, saving valuable time and personnel requirements. A forensic pathologist can do an external exam and read a CT scan in much less time than it would take to perform a complete autopsy.
Incorporation of New Tools into Forensic Pathology Practice
As with any new technology, there are difficulties in the incorporation of the new tools available to the modern forensic pathologist into routine practice. Concerns exist regarding the qualifications of forensic pathologists to utilize these tools, and if these tools may in some way take work away from forensic pathologists.
Regarding the first concern, forensic pathologists have utilized tools in addition to the autopsy for decades, including those that may at first glance not appear to be within their purview. Forensic toxicology is an invaluable part of any modern forensic pathology practice, and the ultimate interpretation of toxicology results is well within the realm of the medical examiner's responsibilities and qualifications despite the fact that the medical examiner is not a toxicologist. And in fact, the toxicologist is only in an appropriate position to report the result — not interpret it, as he/she does not have access to the totality of the investigative dataset. The role of the medical examiner is to interpret the findings in the context of the case as a whole. Similarly, the concern that forensic pathologists are not qualified to interpret postmortem imaging fails to take into account the purpose of postmortem imaging in the context of a medical examiner's practice; namely, the study is performed to identify fatal trauma or gross natural disease. Any forensic pathologist should be able to identify an intracerebral hemorrhage or cervical fracture on postmortem CT just as well as he/she should be able to identify a bullet or rib fractures on postmortem radiographs, despite not undergoing residency training in radiology.
The fear that these new tools may take work away from forensic pathologists fails to consider that no death investigation consists of utilizing the results of a single tool. A molecular panel or postmortem CT result does not constitute a comprehensive medicolegal death investigation. The role of the medical examiner is to incorporate all of the findings from a wide selection of tools to determine the ultimate cause and manner of death. This is not a task that a molecular pathologist or radiologist is able to do based on an interpretation of a single study, and more importantly, they are not legally empowered to do so. Forensic pathologists are the physicians who incorporate all of the components of a death investigation together and opine on cause and manner of death. Furthermore, these newer tools are most commonly useful in supplementing the autopsy, not in replacing it entirely. Their incorporation into forensic pathology practice will likely streamline the workflow, not disrupt it.
There are many historical examples within the field of pathology of new techniques facing criticism upon initial description followed by widespread acceptance into routine practice. George Papanicolau and Aurel Babes published articles describing cytology for the detection of cervical cancer in the 1920's, but this technique was ignored by the medical profession for decades before it became routine practice (54). William Welch performed the first frozen section for the intraoperative evaluation of a tumor in 1891, but this method was criticized as unreliable until the 1920's (55). Both of these methods are now integral parts of routine pathology practice.
Many new tools in surgical pathology were feared at the time of their introduction to potentially disrupt how surgical pathologists did their jobs, or even to eliminate those jobs. Decades ago, electron microscopy/ultrastructural analysis was held as a revolutionary tool that would replace light microscopy in the diagnosis of tissue-based disease. Similar fears appeared with the advent of immunohistochemistry and then molecular analysis of genetic markers in tumors. And yet, surgical pathologists have not been replaced by technology; it is the surgical pathologists who use all these tools, along with their light microscopes and hematoxylin & eosin stains, to do their jobs even better. Despite the angst and initial resistance, the new tools were ultimately assimilated by those who should be their rightful owners.
As forensic pathologists, we need to be mindful of such history in other branches of medicine and pathology. Many of the newer tools coming into existence will be powerful adjuncts; some may in some cases appropriately replace a conventional autopsy. Newer techniques such as postmortem CT should not be feared or criticized because they are new and represent change. Just because we use our hammer (the autopsy) most often, we should not identify ourselves so tightly with it that we feel the need to continue to use it in all cases simply by tradition, as newer tools become available.
Whether some of these new tools should augment or supplant the autopsy is also a matter of office philosophy. In the previous aortic dissection example, this could be diagnosed by PMCT. However, an autopsy would be much better at elucidating the cause of the dissection (e.g., idiopathic, Marfan's Syndrome, syphilis). PMCT could easily detect fatal injuries in a motor vehicle collision, but only an autopsy might contribute the finding of lymphocytic myocarditis that may have caused a cardiac arrest in the driver, causing him to lose control of the vehicle. Cause and manner of death would not be affected, but being able to answer these other questions might be important information nonetheless, to families or an insurance company. It depends on how the office interprets its mandate and how it wants to utilize its resources. A detailed discussion of this point is beyond the scope of this manuscript but the concept of the “value-added” autopsy is described in detail elsewhere (56).
Conclusion
The goal of this article is not to advocate for the use of any one technique in forensic pathology over the other; rather, the aim is to advocate for the responsible use of the appropriate techniques for the appropriate cases. Conventional autopsy (accompanied by investigative history, of course) is still considered the reference standard for determining cause and manner of death. However, conventional autopsy is only one tool in the toolbox, and its utility in isolation is inadequate for a comprehensive medicolegal death investigation. Forensic pathologists should not be viewed as pathologists who perform autopsies; we should be viewed as pathologists who utilize the appropriate resources to conduct a thorough investigation of deaths and incorporate all of the results to determine the cause and manner of death.
Footnotes
The authors have indicated that they do not have financial relationships to disclose that are relevant to this manuscript