
Abstract
The phenomenon referred to as “tandem bullets” occurs when two (or more) projectiles are expelled from a firearm barrel in a single pull of the trigger. A “tandem gunshot wound” occurs when tandem bullets produce injuries. Several scenarios can occur, including the occurrence of multiple entrance wounds produced by separate tandem projectiles as well as a single entrance wound through which multiple tandem projectiles enter the body. We present a case of homicide by tandem bullets in which two tandem bullets entered a single entrance wound, with one projectile exiting the body and one remaining within the body. In addition, we review the topic of tandem projectiles and summarize other situations that may cause initial confusion when attempting to account for all gunshot wounds on the skin and projectiles as viewed on pre-autopsy imaging.
Introduction
In gunshot wound cases, forensic pathologists must account for all external skin defects (i.e., entrances, exits, other) and projectiles, including those known to have exited the body and those that remain within the body. Expanding this concept to the overall investigation of shooting incidents, the ultimate goal of the entire process, including forensic pathology and police investigations, is to account for all firearm discharges, all projectiles and casings, and all injuries, including external and internal trauma. In certain situations, a phenomenon known as “tandem bullets” can cause difficulties when attempting to account for all defects and projectiles. In this report, we present a tandem bullet case of a 14-year-old who was the victim of a gunshot wound homicide in which he sustained a single distant/indeterminate-range gunshot wound of the upper abdomen.
Case Report
Police arrived at the scene of a reported shooting to discover a 14-year-old male lying in the street. Upon arrival of Emergency Medical Services (EMS), a projectile was discovered within the victim's shirt, adjacent to an apparent gunshot wound of the back. There was also a gunshot wound noted on the left side of the abdomen. Prior to transport from the scene to the Emergency Department at the hospital, the police collected and retained the bullet discovered by EMS as evidence. A subsequent radiograph at the emergency department showed the presence of an additional projectile internally
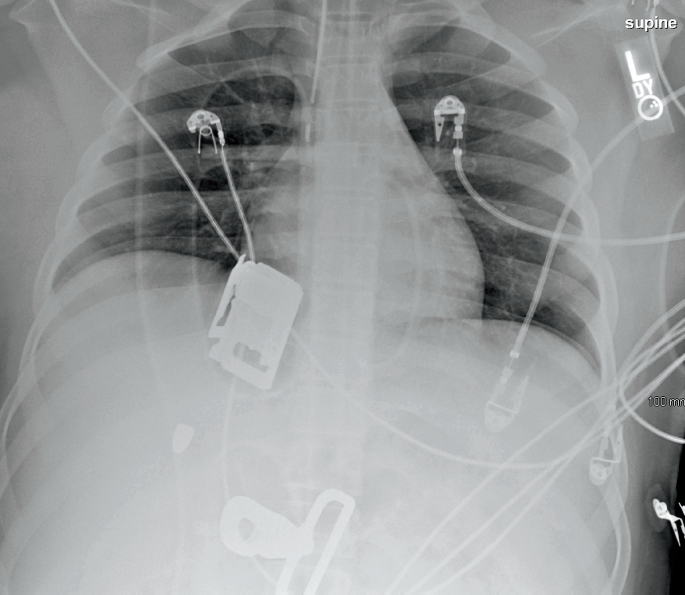
Emergency department radiograph showing a right-sided bullet.
At autopsy, a gunshot entrance wound was identified on the upper left abdomen
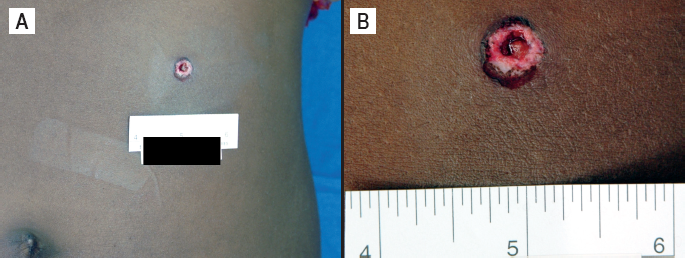
A) Gunshot entrance wound of left abdomen. B) Closer view of entrance wound.
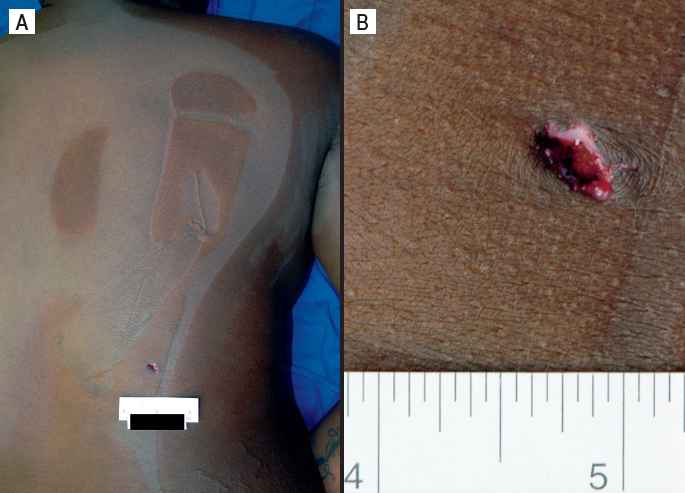
A) Gunshot exit wound of right side of back. B) Closer view of exit wound.
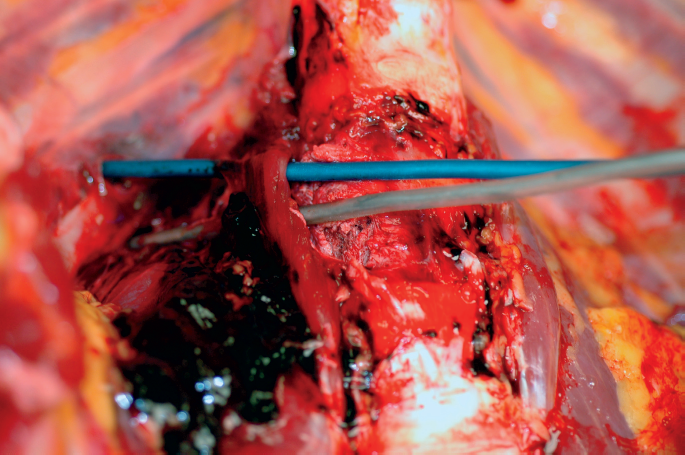
Autopsy photograph (after aorta and organ removal) showing the divergent pathways of the tandem bullets.
Based on the fact that there was a single track that separated into two distinct pathways internally, it was suggested that the case might represent a tandem bullet situation. Gross and stereomicroscopic examination of the two projectiles by a firearms examiner confirmed that they represented tandem bullets
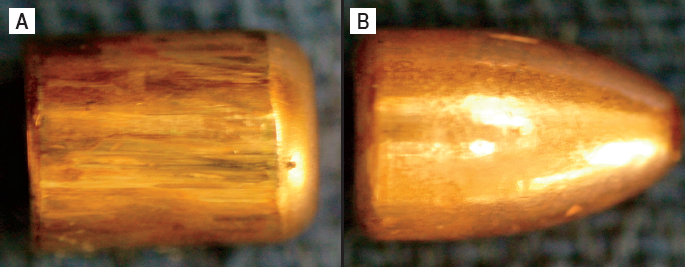
A) The rear-most (back) bullet. Note the flattening of the nose. B) The front-most (front) bullet.
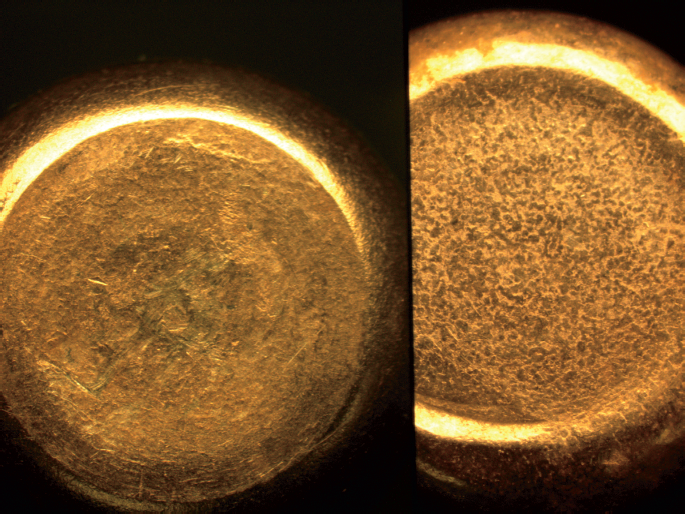
Composite/comparison microscope view of the nose of the back bullet (left) and the base of the front bullet (right).
Based on the autopsy findings and the firearms examiner's evaluation of the two bullets, it was determined that the decedent had died as the result of a single gunshot wound of the upper left abdomen region, involving two tandem bullets entering through the same entrance defect. The tandem bullet shot produced a single entrance wound, with a single track through the majority of the body. While traversing the aorta, the two bullets' trajectories diverged, causing one to exit the lower right back region and the other to remain within the decedent, lodged in the right back's subcutaneous musculature. The first (front) bullet, which had presumably been lodged in the barrel of the gun prior to discharge, remained in the body, while the second (back) bullet passed through the decedent and was found at the scene.
Discussion
Classically, tandem bullets are associated with self-loaded cartridges, poor quality cartridges, or inappropriate caliber cartridges, wherein a projectile from a cartridge with nonoptimal gun powder load becomes lodged in the barrel because of insufficient force to discharge it from the gun (1-5). Subsequent discharge of a subsequent round causes both bullets to be expelled from the gun. Some authors refer to tandem bullets as “piggyback” bullets (1,2). Although most cases of tandem bullets in the literature involve two projectiles, at least one case has been described involving a total of three bullets (6). In three separate but similar cases, a smaller than appropriate caliber cartridge casing and bullet acted as tandem projectiles along with an appropriately sized bullet (7-9). In a different case, two casings and a bullet from 7.65 mm rounds fired from a 9 mm pistol were recovered from within the head of a suicide victim (10). Depending on the range of fire, tandem bullets may produce a single entrance wound or separate entrance sites. While most cases involve bullets from rifled-barrel firearms, at least one case has been reported involving tandem projectiles fired from a shotgun (6). Occasionally, items other than bullets and casings are part of the tandem projectile event. In one case, a barrel cleaning brush was discharged along with a bullet (11). In another case, a bullet, a nail, and a screw acted as tandem missiles (12).
In clinical practice, trauma specialists sometimes refer to the “bullet rule,” wherein the sum of the number of bullet wounds on the skin surface (entrances and exits) and the number of projectiles detected on imaging studies should always be an even number (5,13). Forensic pathologists essentially follow the same reasoning, ultimately requiring an accounting for all skin defects and projectiles. If the “bullet rule” is “broken,” further investigation is warranted to account for the discrepancy. A situation involving tandem bullets with a single entrance wound is one of several instances wherein the bullet rule may be broken. In the case presented, the bullet rule is broken because the number of projectiles on radiograph (one) plus the total number of entrances (one) and exits (one) is three, an odd number. Interestingly, in the setting described in the reference above, with three bullets involved in a tandem bullet scenario, the bullet rule would not be broken (one entrance wound, one exit wound, two projectiles on radiograph). This scenario, along with other similar situations (see below) may be the reason that forensic pathologists do not necessarily routinely subscribe to the “bullet rule” or even use this term, which is somewhat simplistic. Rather, forensic pathologists, in coordination with police investigators, must account for all firearm discharges, all skin defects and all projectiles, whether they are viewed on imaging and eventually collected at autopsy, or they are collected elsewhere, such as at the scene.
Forensic pathologists are well aware of many other situations that may result in an initial apparent discrepancy in accounting for all shots fired, entrances, exits, and projectiles evident on radiographic imaging of bodies at autopsy. In addition to a tandem bullet situation, other situations may result in dilemmas related to accounting for all firearm discharges, bullets, and skin defects. These situations can generally be divided into two categories: situations which suggest that a projectile is unaccounted for, and situations that suggest there are too many projectiles (or too many exit wounds). Tandem bullets typically fit into the second category. In the ensuing paragraphs, a brief review of these two categories is presented.
A variety of situations, some common, some not, can cause initial concern that a bullet/projectile is unaccounted for. Misinterpretation of entrance versus exit wounds, overlooking/missing a “hidden” exit wound, and misinterpreting a graze wound as an entrance wound represent relatively common causes for this confusion. A classic scenario that can suggest that bullets are unaccounted for on initial radiographic exam involves the classic shored exit wound, in which the edges of the wound are supported by an object firmly pressed against the skin, producing an exit wound which mimics an entrance wound (14). Variations on the shored exit wound theme include “incomplete shored exit wounds,” which could theoretically lead one to the conclusion that there are an insufficient number of projectiles via radiographic exam if the shored wound is incorrectly interpreted as an entrance defect (15). The presence of nonfirearm-related skin wounds/defects which mimic gunshot wounds can cause confusion as well as alarm (16–17). Skin defects that mimic gunshot entrance wounds can result in a situation where it is believed that a bullet is unaccounted for. Another common cause for an initial impression that a bullet/projectile is unaccounted for is when the portion of the body containing the projectile is not visualized on initial radiographic exam. This is particularly common when “plain film” radiology is utilized. A variation occurs when a radiopaque object (medical therapy or other object) obscures the visualization of a projectile. A less common, but well-known scenario involves bullet emboli (18-22). Another radiography-related situation that results in a dilemma for the forensic pathologist is the “masking” of bullets on radiographic examination, wherein decreased subject contrast and summation artifact can produce a nearly imperceptible projectile on radiographic examination (23). Bullet/projectile removal via medical/surgical therapy or by other means, such as via peristaltic movement of the digestive tract (24), can cause great confusion, particularly if pathologists rely on antemortem radiographs and a sufficient time of survival precedes death. Blank cartridges can produce severe and even fatal injuries without the presence of a projectile (25-27). These may involve the head, neck, chest, or other locations. Such cases, which are typically contact wounds, will have no exit wound and no projectile detected on radiographs. Cases may occur where separate shots exit at the same skin defect (28). Although exceedingly uncommon, a case has been reported where an intracranial ricochet resulted in a bullet exiting via the entrance wound (29). In both of the latter situations, initial imaging studies will suggest the lack of an expected projectile or projectiles.
In addition to situations that suggest that a bullet/projectile is unaccounted for, forensic pathologists may be faced with situations that raise initial concerns that there are too many projectiles within a body, or, depending on the case, too many exit wounds. As with the previous category, such initial errors can result from simple misinterpretation of entrance versus exit wounds. Overlooking/missing a hidden or subtle entrance wound can produce similar confusion, as can the misinterpretation of a graze wound as an exit wound, or the presence of a partial/incomplete exit defect, which looks like a classic exit wound, yet the projectile remains in the body. The presence of a non-firearms-related skin defect that mimics a gunshot exit wound can lead to similar misinterpretation (16–17). Another situation that suggests there are too many bullets (or exits) can occur if a nonprojectile object, such as a dental restoration, a clothing zipper, or clothing rivet, is misinterpreted as a bullet/projectile during radiographic examination. The typical tandem bullet scenario, as presented in this case report, represents a rare but classic example of this category of cases. A more common occurrence involves bullet/projectile fragmentation/separation. This may occur prior to body impact, when a projectile strikes an interposed target, such that more than one entrance defect results from a single weapon discharge (30), but for the purposes of this category of confusing case types, separation/fragmentation typically occurs after the projectile enters the body via a single entrance wound, producing two or more relatively large pieces evident via radiograph. The classic example involves a jacket that separates from the core after entering the body; the different composition and density of jacket material compared to the core can be recognized via radiographic examination in some instances. The fragments/parts of fragmented projectiles may produce exit wounds in some cases. Another scenario that may suggest the presence of too many projectiles involves the radiologic identification of a retained bullet from a previous, unrelated shooting event (17). Although rare, cases have been reported describing situations where multiple different shots entered at the same site (31–32). In such cases, initial body and radiographic examination will suggest the presence of too many projectiles (or too many exit wounds). A similar, but slightly different scenario may occur when a cartridge is loaded with multiple bullets; examples include cartridges available in multiple calibers that are loaded with multiple lead bullets (e.g., such as produced by Silent Partner and Power Plus Enterprises), handgun cartridges loaded with multiple buckshot pellets, and a military 7.62 × 51 mm Duplex round named M-198 and composed of two 80-gr. bullets (33,34). For each of these multiple-bullet cartridges, a shot fired at close enough range may result in multiple projectiles entering the same entrance skin defect (33). Another potential scenario for erroneously concluding that there are too many projectiles on initial radiographic exam involves the concept described above: incomplete shored exit wounds (15). If such a wound is misinterpreted as a classic, truly exiting (“complete”) shored exit wound, then the identification of a bullet on radiographs is likely to cause confusion.
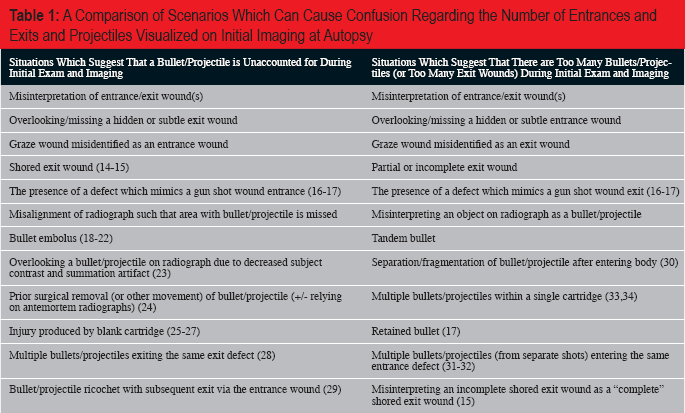
A Comparison of Scenarios Which Can Cause Confusion Regarding the Number of Entrances and Exits and Projectiles Visualized on Initial Imaging at Autopsy
In cases of gunshot wounds, it is important to ensure that projectiles are examined by a firearms examiner. This is especially true in cases that are suspected of involving tandem bullets. Evaluation of the suspect weapon is also ideal, if available for examination. In these cases, the firearms examiner can determine through rifle mark comparison that the tandem projectiles came from the same weapon. Additional features related to how the projectiles abutted one another during discharge allow the examiner to determine the position of the bullets relative to each other. This can involve the gross observation that the two tandem projectiles fit together like two puzzle pieces (4, 5, 9); however, stereomicroscopic comparison, as was performed in the current case, can also provide additional tool mark evidence that the questioned projectiles represent tandem bullets.
Often, the leading (front) bullet will have a large indention on its base, caused by the nose of the second bullet, while the nose of the second bullet is flattened. If the bullets have an exposed lead base, the base of leading bullet may display small indentations of gunpowder particles as well as small patches of striations on its inner periphery; these features are not characteristic of the base of the secondary (back) bullet (35).
Another feature which may occur in bullets having exposed lead bases is rearward protrusion of the lead core of the second (back) bullet; this is thought to result from the rearward impulse force produced on contact with the lodged bullet (35).
In addition to changes that can be seen on the projectiles themselves, certain classic features may be evident in the firearm as well. When the second bullet is fired, the pressure in the barrel is greater than under normal conditions, and this can cause damage to the firearm, resulting in the barrel bulging from the pressure (1). Thus, in a case where tandem bullets are suspected, a firearms evaluation is vitally important, as the gun may have been damaged during discharge. Another ballistics characteristic that is unique to tandem bullets is the velocity of the discharged bullets. The velocity of discharged bullets can be as low as half the velocity of a normally fired round (36). Each of these distinctions is important when considering a possible tandem bullets scenario, and the resultant injuries/findings in such cases.
Conclusion
In summary, a tandem bullet scenario may be one of many possible explanations when the number of firearm discharges based on scene/police investigation, the number of entrance and exit wounds, and the number of projectiles seen on imaging do not initially make sense. Tandem bullet scenarios may result in a single entrance wound or separate entrance wounds. Firearms examination of the projectiles (and gun) can provide conclusive evidence that a tandem bullet scenario has occurred. Additionally, the realization of the implications of tandem bullets can potentially aid in the investigation of the crime committed and ultimately assist in the successful adjudication of a case.
Footnotes
The authors have indicated that they do not have financial relationships to disclose that are relevant to this manuscript