
Abstract
As anthropologists take on a larger role in medical examiner's offices, the incorporation of bone trauma analysis into the autopsy increases. The purpose of this invited review is to summarize recent anthropological literature that exemplifies the value of forensic anthropology in medicolegal death investigation, concentrating in the area of skeletal trauma analysis. Forensic anthropologists have a strong understanding of bone's response to trauma, gained through research and case studies. With this body of knowledge they are able to examine and interpret skeletal injury resulting from blunt, sharp, firearm, and thermal trauma. For example, toolmark class characteristics are recognized through sharp force injury examination, and fracture pattern analysis provides details of the impacting surface area. Interpretation of skeletal trauma allows for reconstruction of events surrounding death, and may inform the manner of death classification.
Introduction
The forensic anthropologists' understanding of bone biomechanics position them to thoroughly and accurately evaluate skeletal trauma, which may provide information critical to the medicolegal death investigation. Anthropologists analyzing blunt force trauma fracture patterns can assess the minimum number of impacts, the direction of impacts, and details of the impacting surface. Tool mark analysis can lead to the recognition of class characteristics of a suspect weapon. Assessing thermal changes in bone allows for the conditions of the fire and the relationship of the body to the fire to be estimated. Anthropological consideration of ballistic defects can contribute to interpretation of projectile trajectory. Details obtained from skeletal analysis may have an impact on the manner of death classification, case investigation, and/or case adjudication.
As anthropologists take a larger role in medical examiner's offices, we see increased bone trauma analysis of skeletal as well as nonskeletal cases (1). The information gained through analysis informs not only the individual case but the field of forensic anthropology as well. The purpose of this invited review is to summarize recent anthropological literature that exemplifies the value of forensic anthropology in medicolegal death investigation, concentrating in the area of skeletal trauma analysis. The review is augmented with images taken from the authors' casework that demonstrate concepts discussed in the research.
Discussion
Before reviewing recent anthropological literature in skeletal trauma analysis, a few concepts and terms need to be defined. Bone, like most material, is stronger under compressive rather than tensile stress. The compressive strength of bone is directly proportional to its density (2). The organic component of bone is elastic and capable of absorbing tensile and compressive forces. The load rate and duration dictate how bone will respond to stress. Continual slow loading stress causes elastic deformation (temporary bending of bonds between atoms), followed by plastic deformation (permanent bending of bonds between atoms) and finally failure. Rapid loading stress results in bone failure in absence of elastic and plastic deformation, behaving as a brittle material (2, 3). Slow loading stress is associated with blunt force trauma while rapid loading stress is associated with firearm trauma. Understanding fracture initiation and propagation is important to accurate fracture interpretation. Fracture initiation is the location of initial bone failure and fracture propagation is the course the fracture takes through the bone. Fracture propagation depends on the direction of force as well as bone microstructures and buttressing systems (3). Controlled impacts of bone have shown that fracture initiation and propagation are strongly affected by impact type, magnitude of force, and cortical thickness (2).
Blunt Force Trauma
Skeletal fractures resulting from blunt force trauma reflect the type, amount, and direction of the force causing the injury. Analysis of the fracture characteristics as well as the fracture distribution pattern is often informative to events surrounding death. For example, a rib fracture pattern resulting from a fall onto a broad surface area such as a floor is very different from a rib fracture pattern resulting from a physical assault with multiple strikes in various directions. In some cases, a fracture pattern analysis may assist the pathologist in the manner of death classification.
Bone biomechanical analysis and anthropological case studies have furthered our understanding of fracture mechanics. Both intrinsic and extrinsic factors affect how bone is fractured. Intrinsic factors include bone geometry, bone density, and stress risers (e.g., the buttresses system of the cranium) (2). Extrinsic factors include area of the impacting object, load velocity, and load weight (2, 3).
Cranial fracture patterns provide information on impact location and surface area of the impacting object. Fracture patterns are commonly described as linear, complex, and comminuted (4). Linear fractures have two end points and may be described as linear or curvilinear. Complex fractures have three or more end points; a stellate fracture is a common descriptor of a complex fracture. Comminuted fractures are fractures that result in fragmentation of the bone. The different fracture patterns provide varying information regarding the impact.
Case reports illustrate anthropologists' success in linking cranial fracture patterns with suspect weapons. Love describes an anthropologic analysis of a cranial fracture pattern identifying a minimum of seven impact sites, consistent with strikes from an object of relatively small surface area (5). A bloodied hammer was recovered from the scene

Calotte with multiple impact sites consistent with strikes from an object of small surface area. The decedent was reportedly hit in the head with a hammer.
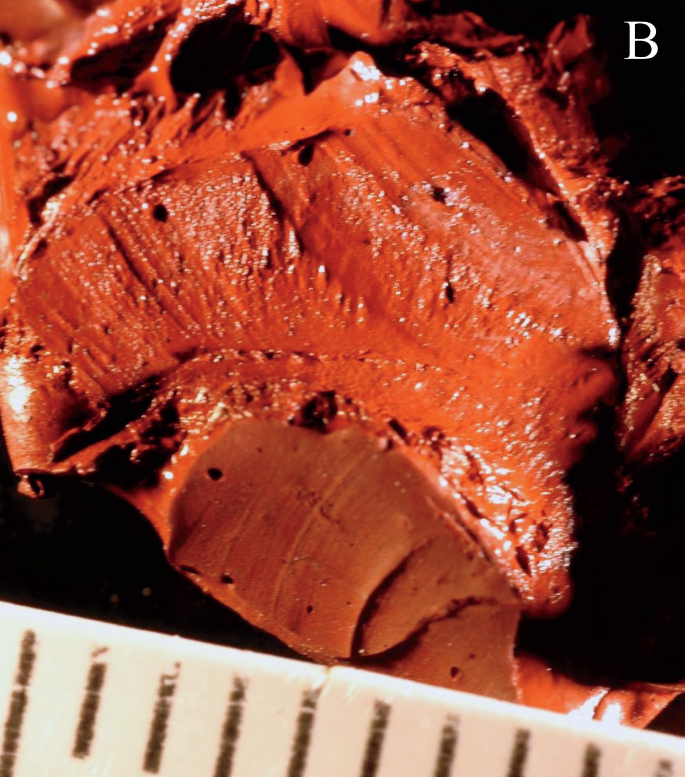
Long bone and rib fractures provide information about the direction of force and type of impact as well and a significant amount of recent research is focused on these bones. For example, Reber and Simmons impacted 255 sheep femora with a pendulum apparatus using an accelerometer to measure the impact force magnitude and a high-speed camera to record the impact site and fracture propagation (7, 8). Evaluating the entire fracture pattern, including complete and incomplete fractures, the authors were able to pinpoint the impact location accurately on 98% of the samples. The authors described eight common fracture patterns. Each fracture pattern consisted of a complete fracture at the point of tension and radiating fractures coursing through the bone at various angles, acute and obtuse. The complete fracture at the point of tension was opposite to the point of impact in the majority of the specimens
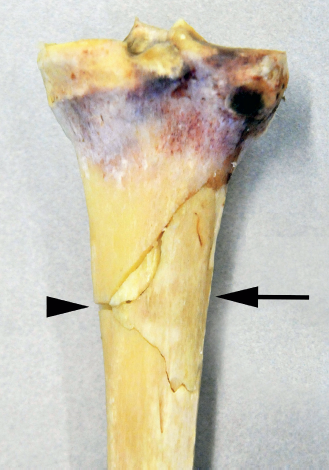
Right tibia with a butterfly fracture. The triangle is marking the point of failure in tension and the arrow is indicating the direction of force.
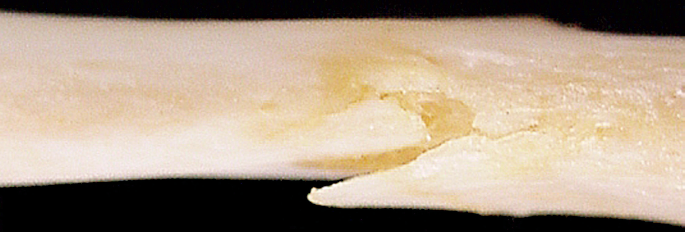
Buckle fracture of an anterior rib. Note that the pleural surface (inferior) is folded onto itself, a failure from compressional forces.
Although a significant amount of anthropological research has enabled practitioners to accurately assess blunt force fracture patterns, other research has continued to raise questions. Most notably is research focused on fracture propagation within the cranium. Gurdjian and colleagues set the foundation for the research by evaluating the propagation of cranial fractures using a “stress coat” technique (11). The researchers coated dry human skulls with a brittle lacquer, dropped the skulls onto a hard surface and evaluated where the lacquer cracked. The team found that on the endocranial surface the cracks initiated at the impact site, regardless of the impact location on the skull. In contrast, the cracks of the ectocranial surface initiated at a location away from the impact site. Based on the lacquer cracking pattern, the researchers concluded that in-bending occurred at the impact site generating tensile forces on the endocranial surfaces and out-bending occurred around the impact site creating tensile forces on the ectocranial surface. Kroman and colleagues tested Gurdjian's theory using unembalmed human heads and a high-speed video camera (12). The researchers placed five human heads in a drop tower structure and struck each on the anterior parietal region with a mass weighing 8.58 kg. The complete skull was exposed except for a small patch of skin at the impact site. Evaluation of high-speed video showed that all fractures radiated out from the point of impact and no out-bending was observed. Baumer and colleagues also investigated fracture propagation using controlled impacts of infant porcine skulls (13). The researchers struck the parietal bone with either a rigid or compliant surface measuring the impact force, impact duration, and fracture length and documenting the location of each fracture. Of the 76 impacted crania, 70 crania were marked with fractures that initiated at the bone-suture boundaries and propagated towards the impact site. This finding is consistent with Gurdjian's theory and inconsistent with Kroman's theory. The use of different methods and human verses animal models limits the conclusions that can be drawn from the research. However, the difference in biomechanical response observed between the human adult and infant pig skulls is a cautionary tale that understandings developed using adult bone studies cannot be applied to pediatric bones without consideration for developmental differences.
Thermal Trauma
Thermal trauma poses unique challenges to decedent identification and recognition of sharp, blunt, or firearm traumata. The role of the forensic anthropologist in cases of thermal trauma often begins at the scene. Forensic anthropologists are trained to distinguish osseous from nonosseous material and human from non-human remains, skills necessary for sorting through fire debris. Furthermore, anthropologists are equipped to thoroughly document the scene, which is critical to maintaining fragment provenience and separating commingled remains. The importance of employing an anthropologist at the scene is best exemplified by the Black Saturday fires that occurred in Victoria, Australia on February 7, 2009 (14). The massive fires resulted in 145 separate scenes spread over 1500 square miles. Initial scene processing did not involve anthropologists. Ultimately, 86 of the scenes were revisited with an anthropologist and 56 additional victims were recovered.
Thermal destruction of bone results in the elimination of water, consumption of the organic components, color change, splitting, shrinkage, and warping (15); yet, significant information can be obtained from burned bone. Warping of bone precludes metric analysis for estimating the biological profile, but morphoscopic methods can be accurately applied (16). Osseous pathologic features are often recognizable in burned bone. For example, remnants of an ossified fracture callus remain adhered to bone despite destruction of soft tissue. Pathologic changes in bone shape (e.g., diffuse idiopathic skeletal hyperostosis) are visible in burned bone despite heat induced warping and shrinking (15). The color of the bone can provide information to the context of the burning and temperature (15, 17). For example green, yellow, pink, or red stains on bone signify that the bone was burned in the presence of metal such as copper, bronze or iron while blackened cortical bone suggest a lower temperature of approximately 300°C and white cortical bone suggests a higher temperature of approximately 800°C (15, 17).
Anthropologists have focused a notable amount of research on recognizing perimortem trauma in burned bone. For example, Pope and Smith introduced sharp, blunt, and firearm traumata to forty donated unembalmed cadaver heads prior to thermal damage (18). Following the burning, the cranial bones were reconstructed and examined for signatures of trauma. Internal and external beveling and radiating fractures were observed in the crania subjected to ballistic trauma
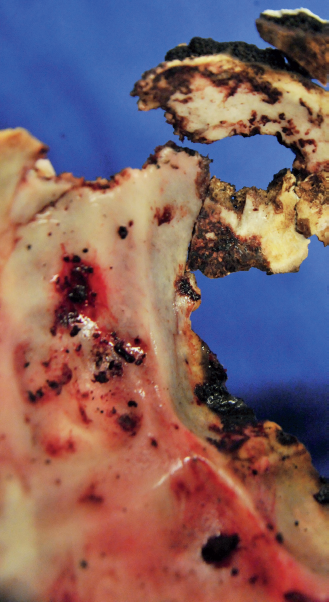
Internal surface of a reconstructed occiput with an entrance gunshot wound (GSW). The decedent was burned in a car fire. The majority of the neurocranium was highly fragmented and required reconstruction to identify the GSW. Note the internal beveling of the wound margins.
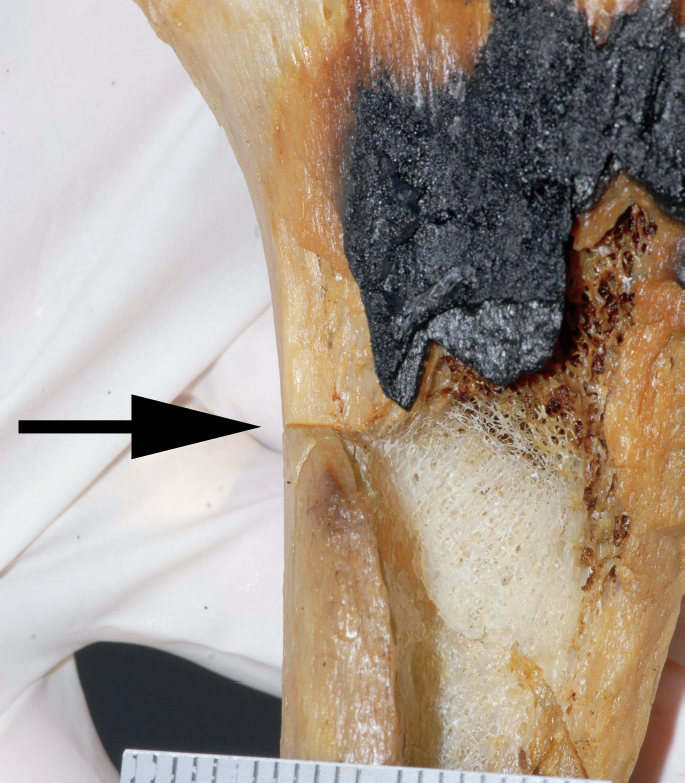
Sharp force injury in a burned proximal femoral shaft. Note the straight margins of the cut mark (arrow).
Sharp Force Trauma
When a knife or saw is used to cut bone or cartilage, signatures of the tool's cutting edge are recorded on the specimen
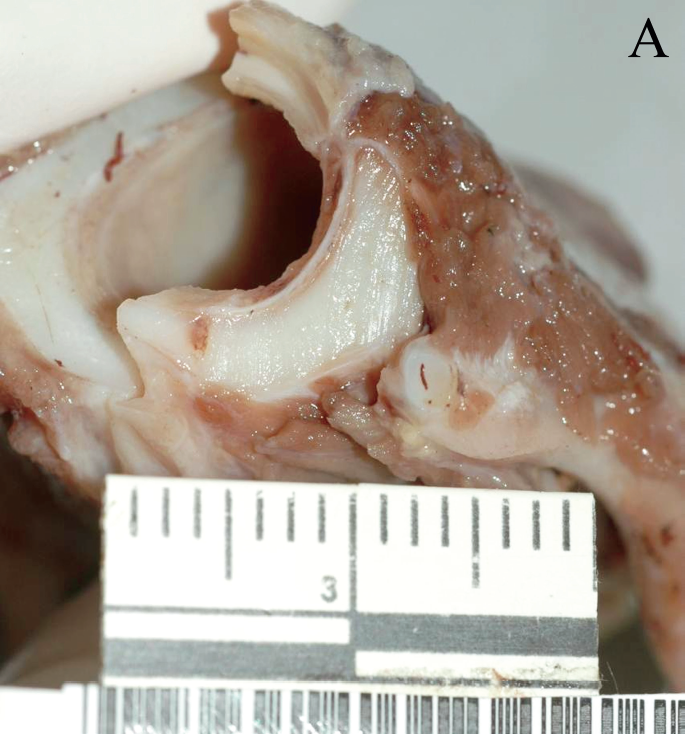
Cut mark through the trachea.
Cast of the cut mark through the trachea. Note the striation pattern indicating a tool with a major and minor serration pattern along the cutting edge.
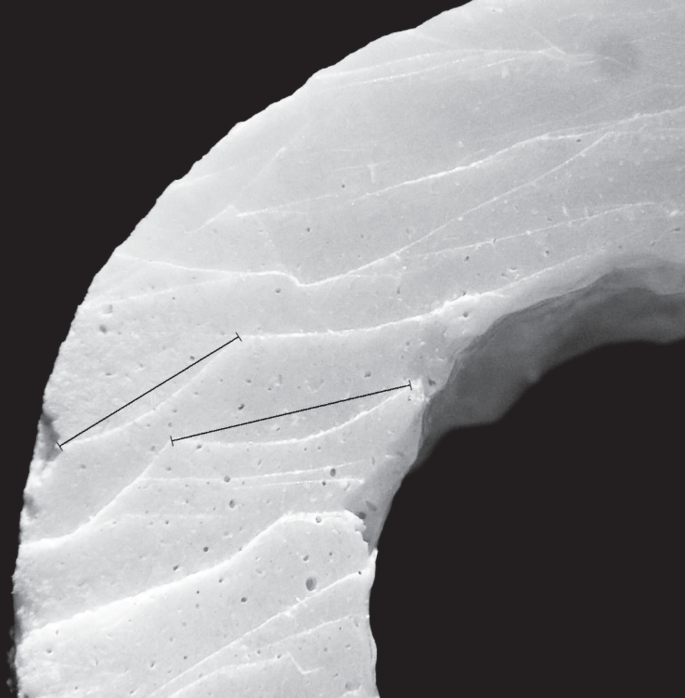
Saw mark made with an eight teeth per inch alternating saw. The lines are marking the tooth hop. The peak to peak distance reflects the teeth per inch setting.
After combining serrated and partially serrated knives into a single group, the researchers found a 98% accuracy rate in recognizing the blade type from the cut mark.
Several sharp force trauma case studies illustrating tool mark analysis from bone and cartilage are published and tool mark analysis has been found admissible in court. For example, Reichs published six saw mark cases in her text Forensic Osteology: Advances in the Identification of Human Remains (24). In each case, she was able to identify class characteristic in the saw mark. In Shepherd v. The State of Texas, the anthropologist provided testimony regarding a tool mark analysis she performed on burned bone (25). During the trial, the defendant admitted to dismembering the victim with an electric jigsaw. The defendant was convicted and sentenced to 99 years of confinement. The defendant appealed the conviction on the grounds that the court erroneously admitted the tool mark testimony based on qualifications of the anthropologist and the reliability and relevance of the testimony. The appellate court found the anthropologist qualified to testify on the tool mark analysis and the testimony to be reliable and relevant under Texas Rule of Evidence 705.
Firearm Trauma
Forensic anthropologists are regularly asked to render their opinion on firearm injuries involving the skeleton. The specific questions asked typically involve projectile trajectory and number of separate impacts. The literature pertaining to the interpretation of ballistic wounds is fraught with problems (26), and has resulted in an oversimplified focus on projectile velocity as the primary factor influencing the characteristics of firearm injuries. For example, the terms “low velocity” and “high velocity” are commonly used to categorize penetrating firearm wounds. These are gradient terms and the thresholds used to demarcate them vary considerably. Ballistic definitions for low velocity vary from less than 400 feet per second to somewhere between 2000 and 3000 feet per second (26). By this definition, most handguns are considered low velocity, and many rifles are considered high velocity, but there is considerable overlap. In addition, velocity alone does not adequately account for variation in ballistic wounds. As with blunt trauma, the manifestation of ballistic injury is influenced by both intrinsic (e.g., bone density, geometry) and extrinsic factors (e.g., size, shape and velocity of impacting object) (2, 3,26). This is true whether the impact material is soft tissue or bone. Bone exhibits considerable focal variability in its resistance to fracture based on morphology and structure. According to Young's Modulus, the capacity of a material (including bone) to resist fracture is dependent primarily on the rate at which a force is applied (2). In general, firearm projectiles impose rapid loads relative to blunt force impacts, and bone tends to respond to ballistic (rapid) loading as a brittle material. Regardless of the ballistic category of a particular weapon, there is no known biomechanical failure threshold that applies to all bones; but, the harder the tissue, the greater the amount of resistance it presents to an impacting projectile and the more destruction it will undergo upon failure (27). Bone is subject to reduced plastic deformation under higher velocity loads. Because of the relative lack of plastic deformation, the bone fragments resulting from ballistic impact are often numerous, but are more easily re-approximated to facilitate interpretation. Further, the lack of plastic deformation is suggestive of ballistic trauma in cases of incomplete reconstruction due to the extent of destruction or incomplete recovery of bone fragments.
The anthropological contribution to the interpretation of ballistic trauma is often through an anatomically informed reconstruction of bone fragments and subsequent interpretation of projectile trajectory. There is generally less tissue loss in bone than soft tissue, and with careful reconstruction, bones often present a detailed record of ballistic wound characteristics. Trabecular bone, as present in the ends of long bones and the bodies of flat bones like the innominate, and fragile cortical bone, as present in the ribs, the body of the scapula, and the midface, can provide an indication of projectile trajectory when carefully reconstructed. For example, anthropological reconstruction of the fragile bones of the midface can clarify the location and number of ballistic wounds.
Both gunshot and shotgun projectiles leave diagnostic defects in bone. Analysis of these defects enables projectile trajectory reconstruction (28–32). Kieser et al. examined experimental gunshot wounds in pig ribs and identified several consistent entrance and exit characteristics (32). The projectile created a cone within the rib with a smaller defect on the side of entry and a larger defect on the side of exit. Also, the exit surface was beveled and radiating fractures extended outward from the wound
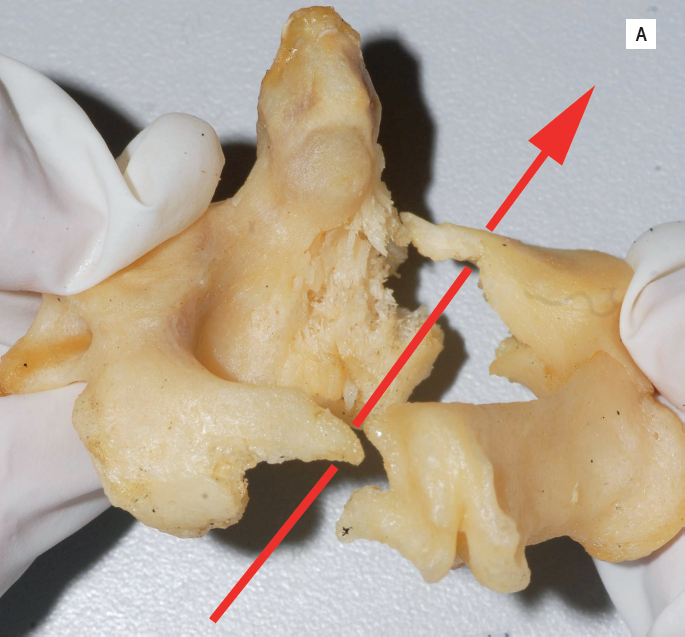
Gunshot wound trajectory through a 2nd cervical vertebra.

Gunshot wound trajectory through a 2nd cervical vertebra.
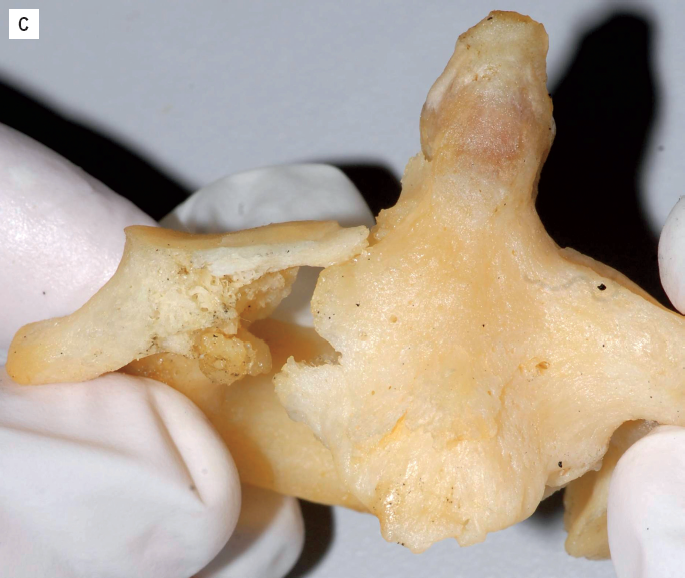
Gunshot wound trajectory through a 2nd cervical vertebra. Note the external beveling along the wound margins.
Anthropological interpretation of firearm trauma is dependent on recognizing diagnostic features that may be present on highly fragmented bone. Careful recovery of skeletal elements, some of which may appear too small to be of value, is important to wound reconstruction and subsequent interpretation of skeletal injury. Thus, the contribution of the anthropologist in cases of firearm injury may extend to the scene as well as collecting bone fragments in soft tissue during the autopsy.
Conclusion
Forensic anthropologists are well-trained to understand bone's response to trauma. Through careful reconstruction of fragmented bone and examination of fracture patterns and wound characteristics, anthropologists can interpret the type of force and minimum number of impacts as well as identify features of the tool. This information may allow for the events surrounding death to be reconstructed and may inform the manner of death classification, case investigation, and/or case adjudication.
Footnotes
The authors have indicated that they do not have financial relationships to disclose that are relevant to this manuscript