
Abstract
In infants and toddlers (less than four years of age), determination of cause and manner of death often requires a complete autopsy. Few evidence-based guidelines exist regarding optimum nervous system sectioning in this population. Over a six-month interval and using a comprehensive section protocol, we categorized cases having neuropathological findings that were critical (Class A), contributory (Class B), or noncontributory (Class C) to the final cause and manner of death. We further evaluated which sections helped make this determination. Among 53 cases (44 infants, 9 toddlers; 26 girls, 27 boys), Class A neuropathology was noted in nine (16.9%). Seven infants had meningoencephalitis (2/7, 28.6%), craniospinal trauma (3/7, 42.8%), brainstem necrosis suggesting Leigh Disease (1/7, 14.3%), and hydrocephalus in Dandy-Walker malformation (1/7, 14.3%); two toddlers had inflicted craniospinal trauma (2/2, 100%). Class B factors were identified in 11/53 (20.8%), including recent hypoxic-ischemic lesions (2/11, 18.2%), meningitis or dural venous sinus thrombosis in systemic sepsis (2/11, 18.2%), multicystic encephalopathy following peripartum asphyxia (2/11, 18.2%), and microcephaly and delayed myelination (Cri-du-Chat Syndrome) (1/11, 9.09%). Class B also included three toddlers (3/11, 27.2%) with features of hippocampal dysgenesis, two in the setting of febrile seizures. Class C comprised normal brains (3/53, 5.7%), and those with findings of uncertain significance, such as white matter and brainstem gliosis (30/53, 56.6%). The sections most valuable for detection of relevant pathology, and thus recommended for routine sampling, were: 1) bilateral hippocampus; 2) cerebral cortex and leptomeninges; and 3) pons or medulla.
Introduction
Forensic agencies throughout the world generally aim to follow the mandate, emanating from the original National Institutes of Child Health and Human Development recommendations from 1991 (1), to perform a complete autopsy, scene investigation, toxicologic, and microbiologic studies in cases of sudden unexpected infant death (SUID) and, by extension, sudden unexpected death in childhood (SUDC). While the neuropathologic examination is a key component of the complete autopsy, forensic pathologists vary in their approach to the central nervous system for several reasons: 1) the uneven availability of neuropathologic expertise or consultation; 2) the lack of staff and material support for the special techniques often required for proper brain tissue processing; and 3) variability in the extent of training and experience in analysis of the developing brain.
The most frequently cited published protocol for neuropathologic examination in SUID is that of the California Department of Public Health. In that protocol, the following blocks are considered “mandatory” for microscopic analysis: pontomesencephalic junction, pons, midbrain, hippocampus, frontal lobe, cerebellum, and choroid plexus; basal ganglia sampling is “discretionary” (2). Of course, any macroscopic abnormalities should also be sampled. A similar approach is advocated by the Royal College of Pathologists. In that protocol, the guidelines specify sections of cerebral hemisphere, brainstem, cerebellum, meninges, and spinal cord, as well as dura if hemorrhages are noted, following two to three weeks fixation in formalin (3).
In this study, we sought to determine, using an evidence-based approach, the optimal examination protocol that would be both high-yield for important diagnostic details and also resource-conscious, given the constraints under which many forensic agencies, including our own, must operate.
In this article, we report our analysis of an unselected series of infant and toddler deaths during a six-month interval, during which we extensively sectioned the nervous system of all cases in a uniform way. We scrutinized two outcomes. The first was whether the neuropathologic examination was critical (Class A); contributory (but non-critical, Class B); or noncontributory (Class C) to the medical examiners' rendering of cause and manner of death (COD and MOD, respectively). The second measure was which brain sections were most frequently used to detect critical and contributory features.
Based on our findings, we recommend a “minimal” section protocol for histology processing (i.e., slides for review prior to finalization of death certificate). Moreover, arising from our experience with this small series, we also suggest a “stock section” protocol for backup, in cases having more complex or unforeseen features requiring further workup.
Methods
During a six-month period, we examined all brain specimens from live-born infants (aged up to one year) and toddlers (aged from one year and one day up to four years) received at the Office of the Chief Medical Examiner, New York City (NYC OCME). We included neonates less than one week of age for the sake of completeness and consistency. At our agency, the medical examiners refer all such pediatric cases to the neuropathology service after placing the brain, along with any other related samples (e.g., spinal cord, dura, eyes, cervical vertebral block [vertebrae and paravertebral soft tissues, with spinal cord and nerve roots in situ]) in 20% neutral-buffered formalin for a fixation period of one to three weeks. While we recognize that some of the referred cases had a presumed cause and manner of death (e.g., child abuse, drowning), we included all infant and toddler cases as an unselected series in order to apply our uniform approach, as a means of determining the utility of various aspects of examination.
The submitted specimens were then evaluated using a uniform protocol developed by Robert's Program on Sudden Unexpected Death in Pediatrics (4), based at Boston Children's Hospital in Boston, Massachusetts (5). The histologic section protocol is comprehensive, identifying 17 specific neuroanatomic sites, including cerebral hemispheres, brainstem, cerebellum, and spinal cord, for standard processing and paraffin-embedding (
Section Protocol for Neuropathologic Examination of Sudden Unexpected Infant Death and Sudden Unexpected Death in Childhood, and Diagnostic Yield of Particular Histologic Sections With Regard to Diagnostic Class A or B

NA - Not analyzed
Sections not part of Robert's Program protocol.
Hematoxylin and eosin stains were applied using standard laboratory techniques. Perl's stain for iron was done in a subset of cases (usually those in which trauma was suspected). Immunostains for various antigens (such as CD45 [leukocyte common antigen], amyloid precursor protein [APP], or macrophage markers [CD68]) were obtained in selected cases.
The slides were reviewed by one of us (RDF) and one or more of the other authors. Additional data (macroscopic photographs, scene investigations, toxicology, microbiology, radiography, forensic anthropology, metabolic, and/or genetic reports) were reviewed. A final neuropathologic diagnosis was made available to the medical examiner to use as needed in their determination of cause and manner of death.
The significance of the neuropathologic findings was qualitatively determined by consensus of all authors as the number and proportion of cases in which the neuropathologic diagnosis was 1) critical (Class A); 2) contributory (Class B); or 3) noncontributory (Class C) to assigning the final cause and manner of death. Class A findings were defined as those primarily or independently responsible for the death of the child (e.g., severe cerebral or spinal trauma, meningitis). Class B findings were considered to be those that did not primarily cause the child's demise, but represented significant lesions (e.g., dural venous sinus thrombosis in sepsis, multicystic encephalopathy from birth asphyxia). Class C cases had no neuropathology or abnormalities insufficient to explain or otherwise predispose to death (e.g., diffuse white matter or brainstem gliosis); we acknowledge that in these cases, the neuropathologic examination ultimately does contribute to determination of COD and MOD by excluding significant lesions of the nervous system. Notation was also made of additional particular findings of uncertain significance, potentially meriting focused research; these features were broadly labeled “possible microdysgenesis” (8–14) and are currently under separate analysis.
For purposes of this study, examples of some Class A and B diagnoses are illustrated in the Results. For some Class C diagnoses, the following features were used. For diffuse white matter gliosis, the presence of two or more astrocytes with hypertrophic cytoplasm per high-power field (x400) was considered sufficient. Care was taken not to overcall myelination glia (
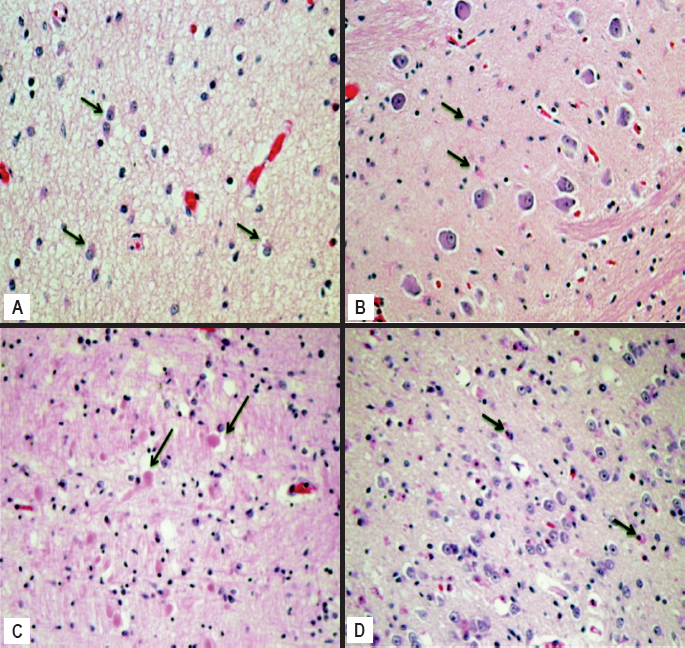
Some common histologic features seen in the cohort (see also
Acute neuronal ischemia (ANI) was noted when neuronal nuclei were condensed and angulated, and the cytoplasm was hypereosinophilic; sometimes the nuclei were fragmented (apoptotic) (
Hemorrhagic lesions (subdural, subarachnoid, epidural, germinal matrix, ocular; not illustrated) were called “acute” if intact red cells were seen in the specified site; “subacute” if scattered macrophages or occasional spindle cells (fibroblasts) were infiltrating; and “chronic or old” when hemosiderin, macrophages, fibroblasts, and fine neovasculature were seen.
Meningoencephalitis required inflammatory cells within the leptomeninges and cortical parenchyma, the latter characterized by microglial nodules and/or neuronophagia (see Results). Focal slight inflammation in any site was considered nonspecific, and not used for diagnosis.
Hippocampal dysgenesis was determined based primarily on dispersal and bilamination of the dentate gyrus, as well as macroscopic asymmetry of the hippocampal formations, as described by Kinney and colleagues (7, 10) (see Results).
Results
The demographic characteristics, causes and manners of death, and neuropathologic findings are shown in
Case Demographics and Findings in Sudden Unexpected Infant Death and Sudden Unexpected Death in Childhood
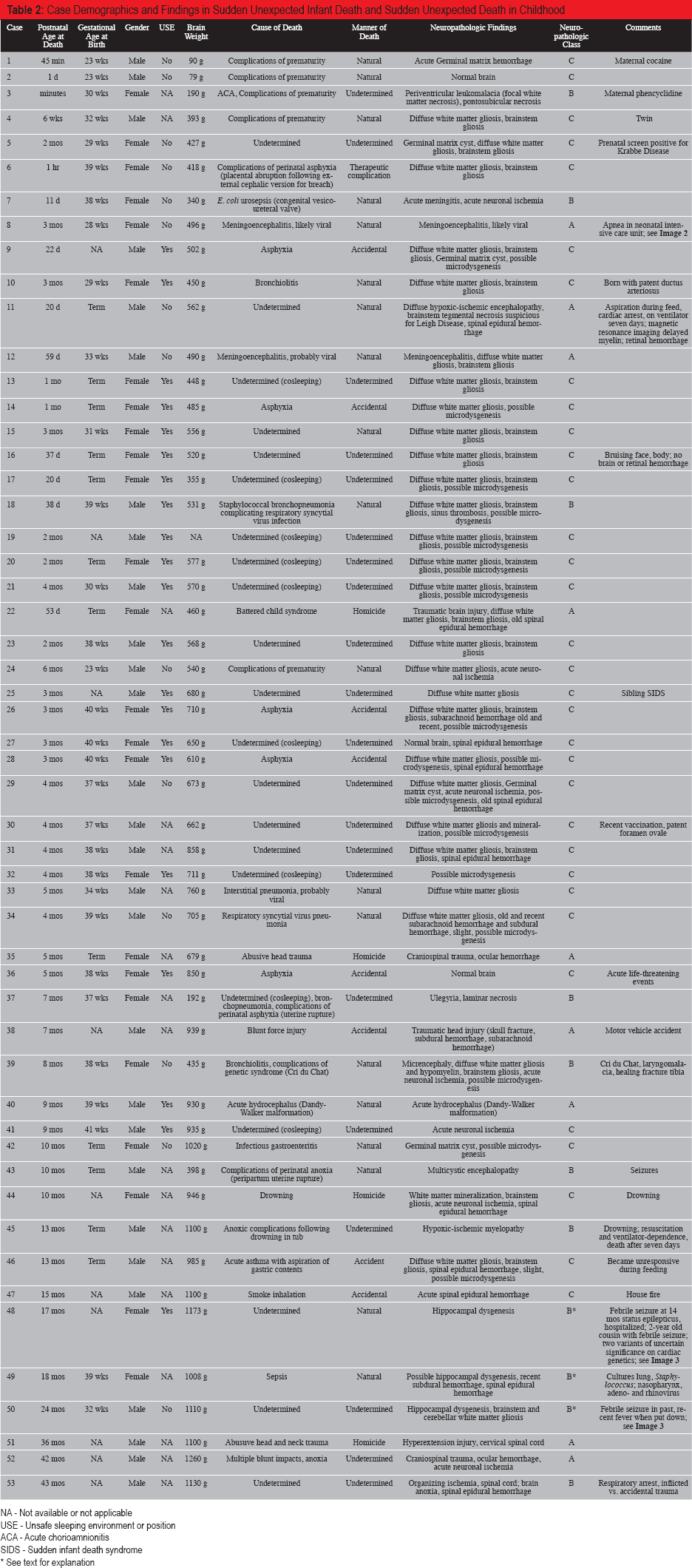
NA - Not available or not applicable
USE - Unsafe sleeping environment or position
ACA - Acute chorioamnionitis
SIDS - Sudden infant death syndrome
See text for explanation
Clinicopathologic Characteristics of Study Group
During the six-month study interval, we received 53 cases for evaluation. Of these, 44 were infants (age range, minutes to ten months; median, two months) and nine were toddlers (age range, 13 months to 3.5 years; median, 18 months). Twenty-six were girls and 27 were boys. Thirteen were born prematurely between 23 and 36 completed gestational weeks. The gestational age in weeks was not known in all cases; in many it was only known to be “term”, and when no specific mention in the investigator's or medical examiner's notes was made, it was assumed to be term.
One infant had a history of acute life-threatening events (ALTEs) prior to demise. One had episodes of apnea in the nursery. Specific neurologic conditions noted in infancy prior to the time of autopsy included Dandy-Walker malformation (n=1; status post ventriculoperitoneal shunt, with recent removal), Cri du Chat syndrome (n=1), and multicystic encephalopathy/ulegyria (n=2; related to catastrophic peripartum anoxia at term).
Two toddlers had a personal history of febrile seizures. One of these (Case 48) had required hospitalization for status epilepticus three months prior to death, and had a 2-year-old cousin with febrile seizures; at autopsy, two variants of uncertain significance (TRPM4 [NM_017636.3:c.2502C>G g.19:49699988C>G] and ANK2 [NM_001148.4:c.5786C>T g.4:114275560C>T]) were noted on our in-house 95-gene cardiac genetic analysis panel. The other (Case 50) had one febrile seizure in the past; the night he was put to bed, he had been noted by the caretaker to have a fever. A third case with hippocampal histology suggestive of dysgenesis (Case 49) was not known to have any prior febrile seizures, but did have autopsy microbiologic cultures positive for S. aureus, adenovirus, and rhinovirus.
Of the 12 infants known to be born prematurely, four died of related complications (two within a short time of birth at 23 gestational weeks and two after multiple complications including respiratory and gastrointestinal illnesses). One died within minutes of birth at 30 gestational weeks in the setting of severe, acute chorioamnionitis. Ten infants (both term and preterm) died of infection (pneumonia, sepsis, gastroenteritis, or meningitis; bacterial or viral).
With regard to unsuspected substrates for sudden death, one infant had a cardiac defect found at autopsy and another had brain changes highly suggestive of Leigh disease, including neuroimaging findings of delayed myelination, although the diagnosis could not be confirmed (specific mitochondrial abnormality testing was not available).
Five infants died of accidental asphyxia related to wedging, overlaying, or occlusive bedding in bed sharing or other positional compromise.
Nine others were in unsafe sleeping environments (e.g., bed sharing and excessive soft bedding; denoted as USE in
Abusive head and/or spinal trauma was documented, along with general autopsy findings and consistent perimortem circumstances, in four cases (two infants and two toddlers). Two children died by drowning, and one in a house fire. One infant died following accidental blunt force trauma (in stroller hit by motor vehicle).
Findings with Regard to Diagnostic Class A, B, or C
Of the 44 infant cases, seven (15.9%) had Class A neuropathologic findings critical to the cause and manner of death. These diagnoses included meningoencephalitis (2/44) (
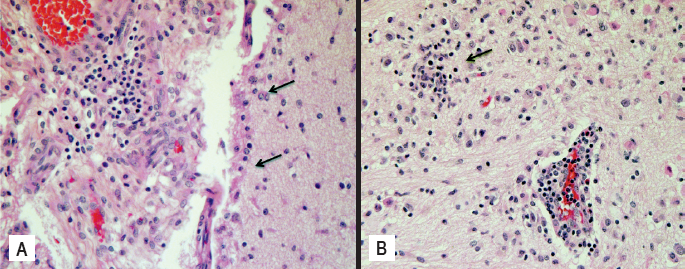
Meningoencephalitis, likely viral.
Among the toddlers, two of nine (22.2%) had Class A neuropathologic findings, comprising inflicted craniospinal trauma (
Among all infants and toddlers, Class B factors were identified in 11/53 (20.8%), and included recent hypoxic-ischemic lesions (2/11, 18.2%); meningitis or dural venous sinus thrombosis in systemic sepsis (2/11, 18.2%); multicystic encephalopathy/ulegyria following peripartum asphyxia (2/11, 18.2%); hypoxic-ischemic myelopathy, one in (near-)drowning after seven days on mechanical ventilation, and one in undetermined circumstances (2/11, 18.2%); and microcephaly and delayed myelination (Cri-du-Chat Syndrome) (1/11, 9.09%). Class B also included three toddlers (3/11, 27.2%) with features of hippocampal dysgenesis, two in the setting of febrile seizures denoted as B* in”
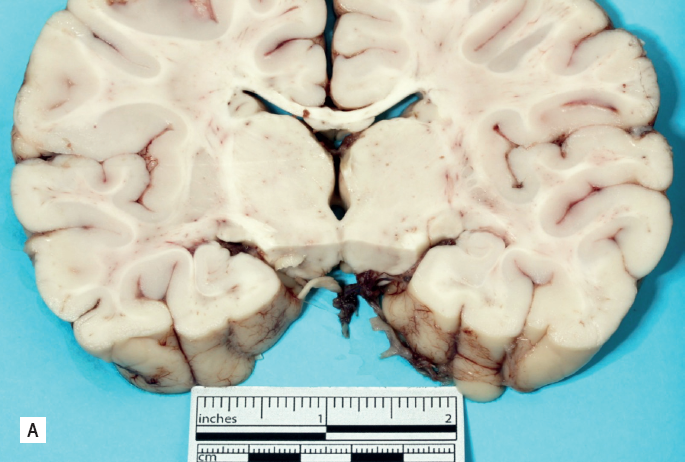
Hippocampal dysgenesis. Coronal section of cerebral hemispheres at level of lateral geniculate nuclei, demonstrating asymmetry of the hippocampal formations. Note the more vertical orientation of the left hippocampus (left side of image), as compared to the right (Case 48).
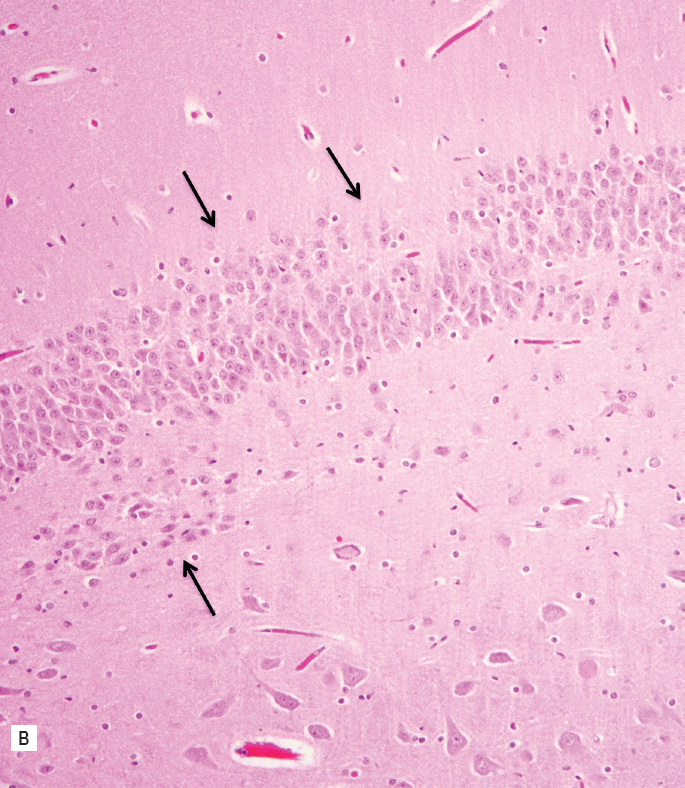
Hippocampal dysgenesis. The dentate gyrus shows marked irregularity in thickness with focal duplication (bilamination) (arrows) (Case 50) (H&E, x200).
Noncontributory (Class C) features, such as white matter and brainstem gliosis, were identified in 30/53 (56.6%); three of 53 cases (5.7%) had normal brains (
Diagnostic Yield of Histologic Sections
Of the 53 study cases, the recommended neuroanatomic sites were sampled in at least 77.4% (amygdala), up to 98.1% (cerebellum). Those that had more limited sampling (n=6; number of sections submitted, 5–11) tended to be very premature (i.e., have small brain specimens), autolyzed, or otherwise suboptimal. Even among those cases with limited sampling, Class A and B diagnoses could be made (Cases 12, 38; Case 7, respectively).
The most valuable sections in terms of providing information considered Class A or Class B with regard to the determination of the COD and/or MOD were the hippocampi (45.0-50.0% of cases), basal ganglia including internal capsule (40.0%), midbrain and pons (45.0%), medulla (60.0%), cerebral cortical sites (up to 35.0%), and dura (generally when hemorrhages or neomembranes were seen macroscopically, 35.0%) (
Eyes and/or optic nerves and cervical cord/vertebral blocks with nerve roots were obtained by the referring medical examiner in ten and three cases, respectively. Of note, these specimens were generally obtained in cases with a high index of suspicion (rather than being routinely taken as a default); thus, they were not included in the analysis of diagnostic yield.
Discussion
The NYC OCME is a busy center performing over 5000 full autopsies per year. As a government (i.e., taxpayer-supported) entity, we are under continual pressure to justify our resource allocation, while also being expected to care for families and protect the public health. Thus, we depend upon evidence-based analyses of our practices to determine the optimal diagnostic yield for our efforts regarding certain types of deaths among the population we serve. It was our goal, in this study, to survey an unselected series of infant and toddler cases received at our office across a six-month interval in order to determine an overall best practice with regard to the extent of the neuropathologic examination needed to influence the final formulation of the cause and manner of death.
We applied a comprehensive, uniform sectioning protocol to all infant and toddler central nervous system specimens, and tallied the instances in which the neuropathology examination was critical (Class A); contributory (Class B); or noncontributory (Class C) to the medical examiner's formulation of the COD and MOD. Our findings indicate that a substantial proportion of cases—about 17% across infant and toddler deaths—had neuropathologic abnormalities having crucial impact on the final COD and MOD. An additional 21% had neuropathologic findings playing a somewhat influential role in the final formulation of cause and manner. These results stand in contrast to the study of Pryce et al., in which only 6% of SUID cases had gross and/or microscopic neuropathologic findings of importance to the final diagnosis (15). That study differed, however, in important ways from ours. Although it was a very large study, comprising 724 SUID cases having both macroscopic and microscopic findings accrued over 14 years, the neuropathological examinations were conducted entirely by pediatric pathologists in 38% and by pediatric pathologists macroscopically and by neuropathologists microscopically in 36%, with only 26% being completely worked up by neuropathologists. Moreover, the study was retrospective and therefore lacked the uniformity of approach and consistent expertise leveraged in our study. Of note, the range of neuropathologic findings in that study was similar to ours, including meningitis and hydrocephalus. Their concluding points were that a “macroscopically abnormal brain and the presence of a clinical history of possible neurological disease or of inflicted injury are significantly more likely to be associated with significant histological brain abnormalities” (15). While we essentially are in agreement, we demonstrate a higher percentage of cases in which the neuropathologic examination was influential. We further offer a refinement of the default section protocol, based on the impact of microscopic evaluation of specified regions on the final determination of cause and manner of death.
In line with many prior reports in SUID (also referred to as SIDS in the historical literature), we also noted relatively nonspecific neuropathologic changes, including gliosis of the deep cerebral white matter and brainstem, and acute neuronal ischemia, in over 50% of our cohort. Such subtle white matter and brainstem gliosis has been interpreted as a marker of hypoxia-ischemia, perhaps occurring in the setting of observed or occult ALTEs (16). Of note, one infant in our cohort had a clinical history of ALTEs, and another had apnea in the intensive care nursery; however, neither had appreciable gliosis according to the criteria set forth in the Methods.
Spinal epidural hemorrhage was fairly common (10/53 cases), and showed no pattern of association with the dominant pathologic process related to COD and MOD. This finding is in alignment with the review of Ali and Fowler (17).
Hippocampal dysgenesis, as defined by Kinney and colleagues, first in toddlers with febrile seizures (12), and more recently in infants (8, 13), has yet to be replicated as a diagnostic entity in other large series. Nevertheless, we felt compelled to make the neuropathologic diagnosis in two of our toddlers with clinical histories of febrile seizures, on the basis of macroscopic asymmetry of the hippocampal formations as well as microscopic features, chiefly dispersal and bilamination of the dentate gyrus. We also had a third toddler with pathologic features suggestive of hippocampal dysgenesis, but without a known personal or family history of febrile seizures. During the course of this study, we came to consider these cases as “Class B*” (
Less clear-cut (i.e., more subtle) variability in the microscopic anatomy of the hippocampus (e.g., thickness of the dentate gyrus with dispersal and/or attenuation, or looping of dentate cells around a vessel) was noted in a subset of our cohort, and is undergoing separate detailed analysis with regard to potential clinical significance.
Of note, those cases assigned by us as Class C, though not directly contributory to COD or MOD, nonetheless have value in excluding underlying substrates in SUID and SUDC. We emphasize that following the suggested sectioning protocol lent a degree of confidence that no significant finding was missed in what was undertaken to be a complete autopsy.
With respect to the value of specific neuroanatomic sampling in the determination of COD and MOD in our study population, we found that the following sections tended to have the greatest diagnostic yield, assisting in detection of inflammation (infection), hypoxia-ischemia, or malformation: hippocampus (both sides if asymmetric, or in the setting of concern for febrile seizures); cerebral cortex and leptomeninges; basal ganglia; and brainstem, especially medulla. Sections of dura were useful for dating of associated hemorrhage, when present. We emphasize that all other neuroanatomic locations mentioned in the protocol in
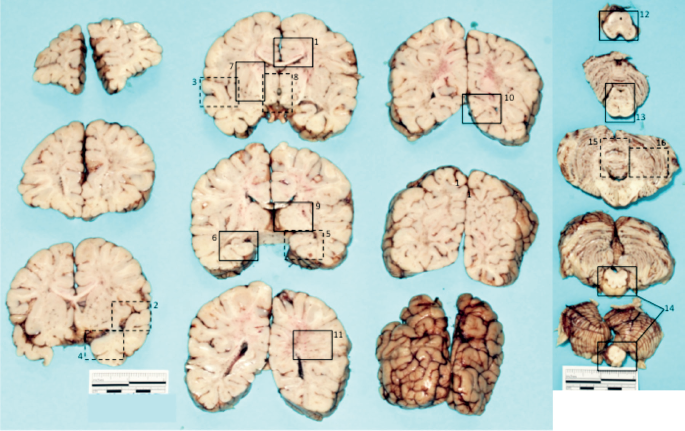
Blocking diagram for histologic sectioning in sudden unexpected infant death and sudden unexplained death in childhood cases, numbered according to the section number in
Limitations and Strengths of Study
We acknowledge certain limitations in our study, particularly the somewhat subjective nature of determining diagnostic impact class in a given case. We tried to set forth our criteria a priori, and required consensus among all authors after reviewing all circumstances of each case. However, other practitioners may bring a different set of experiences and judgment to bear on this determination. Our cohort also consists of an admittedly relatively small number of cases.
Despite these potential weaknesses, we highlight some important strengths. First, we point out the value of the uniformity of our approach to all cases in an unselected series, using a sectioning protocol recommended by a recognized expert in the field of sudden unexpected death in pediatrics, Dr. Hannah C. Kinney, who trained and has been a long-time collaborator of one of us (RDF). This approach likely minimized variability in selection of anatomic blocks, as well as in interpretation of neuropathologic changes, which we defined at the outset. All blocks were processed in a single, experienced laboratory at the NYC OCME. With this approach, it was our hope to provide guidance for the larger forensic pathology community with regard to the optimal approach to examination of the nervous system in these challenging cases.
Conclusion
It was our goal to develop an evidence-based rationale for a standard neuropathologic workup in cases of sudden unexpected infant and childhood death. To that end, we analyzed the proportion of such cases in which the nervous system was of key importance in determining the COD and/or MOD. We found that as many as one in five cases had significant abnormalities of the nervous system impacting on the final understanding of the cause and manner of death, reinforcing the need for careful and thorough evaluation of the brain, spinal cord, and their coverings. Moreover, we identified a practical subset of sections for microscopy for optimal yield of such key findings. Finally, we add limited evidence that, at least in toddlers, hippocampal dysgenesis in the setting of febrile seizures may be worthy of recognition as an underlying mechanism of death sui generis.
Footnotes
Acknowledgments
The authors gratefully acknowledge the support of Juliette Smith, Amal Rezkalla, Skye Bailey-Rodney, Maribel Sansone, William Wu, Joseph Hynes, Latasha Martin, Histology Staff at the NYC OCME Histology, for their care and skill in overseeing the processing of these precious diagnostic samples. Agency photographers Jeff Spielman, Gina Santucci, Rosie Johnson, and Julie Lee provided expertise in specimen photography. We also thank Dr. Barbara Sampson, Chief Medical Examiner, Deputy Chief Dr. Jason Graham, Manhattan Deputy Dr. Michele Slone, Brooklyn Deputy Dr. Jennifer Hammers, and Queens Deputy Dr. Melissa Pasquale-Styles for their support of this project.
The authors have indicated that they do not have financial relationships to disclose that are relevant to this manuscript