
Abstract
This article describes the current state of child death reviews (CDR) in the United States. The CDR process has evolved over almost 40 years from informal local meetings to a coordinated effort involving all 50 states. Child death review programs across the country vary in the level of financial and administrative support, legislation, and review processes. While there is still a long way to go in standardizing the practice between states, great strides have been made in data collection, education, and prevention initiatives.
INTRODUCTION
History
Child death review (CDR) teams have been active in the United States for nearly 40 years. Many CDRs began as informal meetings concerning a single case or series of similar cases, and subsequently became established into law. Other teams were established only after mandated by state law. Los Angeles County created the first formal CDR in 1978, under the Interagency Council on Child Abuse and Neglect (ICAN). While there was skepticism over the value of reviewing the deaths of children, participants began to recognize the value in the reviews. Additional information provided in a group setting led to better explanations of some suspicious deaths and even identified unsuspected homicides. Additional California counties followed suit and by the mid 1980's there were local teams in Oregon, South Carolina, and Missouri (1, 2).
By the mid 1990's, several reports by the US Advisory Board on Child Abuse and Neglect brought child abuse and neglect to the attention of the nation (3). In a 1995 report entitled, “A Nation's Shame, Fatal Child Abuse and Neglect in the United States,” the board made 26 recommendations concerning child abuse and neglect, ranging from new prevention programs and campaigns to increased sentences for child abuse perpetrators (3). While the scope of the report was child abuse and neglect, several recommendations focused on multidisciplinary training and review and would eventually encompass all child fatalities. Two recommendations are specifically of interest to forensic pathologists: 1) the need for more professionals in the field (though not specifically naming forensic pathologists) and 2) a need for child autopsy protocols
1995 US Advisory Board on Child Abuse and Neglect Recommendations Focused on Multidisciplinary Training and Review (3)

Many of the recommendations in the 1995 report saw little traction or support, despite national media attention. Progress was slow and associations such as the American Academy of Pediatrics and the National Association of Medical Examiners (NAME), along with several government agencies including the Centers for Disease Control and Prevention (CDC), pushed for federal funding for CDR programs (4).
By 2001, all states had some form of child death review; however, activity was inconsistent due to shifts in personnel and budget. In 2003, a nationwide review showed that Massachusetts and Ohio did not have active teams (5). This study noted that CDR programs were highly variable by state and that inconsistencies limited efforts to compare data at a state or national level and make prevention recommendations. At that time, 33 states had legislation permitting or mandating CDR and 16 states reported no state funding for CDR programs. Less than half of the participating states reviewed all child deaths. The study indicated that teams most often excluded natural deaths and deaths reported as SIDS (5). This highlights one of the dangers of considering SIDS to be a natural death and is one of the reasons some medical examiners are reclassifying these cases as “undetermined” (6).
By 2005, there were 20 states with local CDR teams with state advisory teams or boards. Fifteen states had only state reviews, 13 states had both state and local reviews, and two states had only local reviews (7). A 2010 study by Shanley et al. showed again two states (this time Arkansas and Idaho) with inactive state teams. By 2010, there was a substantial shift in case selection, with no teams reporting the exclusion of SIDS cases. Impressively, 15 state programs conducted full reviews of all child deaths (0-17 years). Twenty-two percent of the 34 programs not reviewing all deaths reported exclusion of cases due to natural causes or medical illness (7).
The most recent (2016) report on child death review from the National Center for Fatality Review and Prevention (NCFRP) indicates that there are now more than 1350 state and local teams, involving all 50 states, the District of Columbia, Guam, and the Navajo Nation (8). At the time of this publication, Puerto Rico is in the process of building a team. All states now have an oversight agency and a designated coordinator for child death review (8).
Healthy People 2020 (HP 2020), a ten-year initiative by the US Department of Health and Human services promoting healthy behaviors, specifically addresses CDR. Within their injury prevention plan, HP 2020 seeks to:
… increase the number of States and the District of Columbia where 90% of deaths among children aged 17 years and under that are due to external causes are reviewed by child fatality review teams (9).
It also lists a second goal to:
… increase the number of States and the District of Columbia where 90% of sudden and unexpected infant deaths are reviewed by a child fatality review team (9).
DISCUSSION
Legislation
At this time, 45 states (including the District of Columbia) have specific legislation concerning the structure and functions of CDR. Legislation or administrative regulations for state teams exists in over 88% of the states. Six states (Idaho, Montana, New York, South Dakota, Washington, and Wisconsin) have no legislation for state teams. Alaska has a review process for child abuse and maltreatment deaths through the Medical Examiner's Office, but reviews of all other preventable deaths are conducted through the Health Department and are not mandated (9).
There is more variability among state laws concerning local CDR. Only 17 states mandate local teams and another 19 states permit these reviews. Fifteen states have no specific laws concerning formation of local teams or their scope of work (9).
State laws often address specific concerns or protections for the teams and their cases. Many states dictate the meetings are confdential and not open to the public. Meetings and their reviews are commonly protected from subpoena or discovery and not subject to the Freedom of Information Act. In 2016, five teams reported that a team member had been served a subpoena for information collected at CDR, highlighting the need for laws protecting CDR information (9).
Thirty-seven states define the membership of state teams, while 26 states define the membership of local teams (9). State laws commonly address sharing of records and data between agencies, define the types of cases to be reviewed, and whether (and how often) the teams generate reports back to the state.
Child Death Review Purpose and Structure
Most CDR teams have two main purposes: 1) identifying and collecting data pertaining to the cause and manner of child deaths, and 2) providing prevention recommendations to state or local agencies based on this data. Most teams will also review agency involvement surrounding a death. Questions during these reviews may highlight gaps in protocols or the need for additional training, such as:
“Should Child Protective Services (CPS) have been notified of this death?”
“Why wasn't this case referred to the medical examiner?”
“Why was an autopsy not performed?”
Rarely, teams and their reviews assist in prosecution of child abuse and neglect. This may be by identifying a case that previously was not thought to be child maltreatment. In some jurisdictions, the case review is designed to be investigative, occurring shortly after the death (see below).
Child death review teams are structured differently depending on the geographic area and population. Many states have both state and local teams, but other states may only support one or the other. If present, local teams always review individual cases and may provide recommendations and responses to findings. State teams with no corresponding local teams have the same function. When there are both state and local teams, case reviews are most often only carried out by the local teams. Local teams may be mandated or voluntary depending on the state, but even mandated teams will have voluntary participation by its members. The NCFRP describes four models of CDR in the United States
Four Models of Child Death Review Described by the National Center for Fatality Review and Prevention (10)

Local team membership most often includes representation by a medical examiner or coroner (or Justice of the Peace in Texas), law enforcement, child protective services, emergency medical services, pediatricians, the local District Attorney's office, and public health. Other groups commonly represented may include injury prevention programs, child advocacy groups, mental health professionals, and educators. State teams can have a similar make up, but may also include appointees of the state or governor. Uncommon team members have included family members affected by a child death and representatives of the insurance industry, tribes, and the armed forces (5).
State teams commonly meet quarterly, while local team meetings are far more variable. In metropolitan areas with large numbers of child fatalities, the teams may meet monthly or even more frequently. Jurisdictions with smaller populations and lower numbers of child fatalities may meet every other month, quarterly, or may only meet as needed.
Child death reviews may be retrospective, investigative, or parallel to ongoing certification and investigations (5). Retrospective reviews occur after the cause and manner of death have been determined. Some states may even require that these retrospective reviews take place after criminal prosecution is complete, thus potentially delaying the reviews for years. Some teams may review cases shortly after the death and use the multidisciplinary approach to help determine the cause and manner of death or assist in the investigation. This investigative approach has the benefit of reviewing the case while it is fresh (as opposed to months or even years later), but may complicate the desire for team protection from subpoena or discovery. Parallel reviews occur prior to the completion of the death investigation or potential prosecution, but the team does not provide direct input into either.
Fetal and Infant Mortality Review teams (FIMR) are becoming more common, and there are now FIMR teams in 26 states (11). Some of these teams work with CDR while others are completely separate projects. A small percentage of teams also review cases of serious injury or “near fatality,” though identification of these cases may be more difficult. These events may be more appropriately addressed by a separate review team, or perhaps a subcommittee within CDR, assuming these near fatalities can be identified.
National Support for Child Death Review
In 2002, the National Center for Child Death Review (NCCDR) was funded by the US Department of Health and Human services. With the eventual inclusion of FIMR, the NCCDR became the National Center for Fatality Review and Prevention (NCFRP). Today, the NCFRP serves as the national resource for CDR and FIMR (12). The NCFRP website provides tools and guidance for state and local teams, links and instructions on entering information into the National Child Death Review Case Reporting System (NCDR-CRS), and access to child mortality data. One particular publication of note is the Program Manual for Child Death Review, published in 2005, which serves as a manual for development and management of state and local CDR teams (13).
Two of the original 2002 objectives of the NCCDR were to assess how states collected CDR data and- determine if it was possible to create a standardized reporting tool for all agencies. At the time, 44 of 50 states used some type of reporting system, but there was great variability in the data acquired. Child death review coordinators from 19 states participated in the design and testing of what would become the NCDR-CRS. The system allowed local and state teams to electronically collect data on child fatalities, generate reports from that data, and allow other advocates to access the data in order to guide prevention policies (14). The NCDR-CRS has gone through four versions since its creation and version 5.0 is currently in development. Of note, the upcoming version will incorporate a new module for FIMR teams.
In 2010, 35 states participated and entered more than 84 000 cases into the database. By 2015, this participation had increased to 45 states, but decreased slightly to 43 states in 2016. More than 189 000 cases have now been entered into the NCDR-CRS. For teams not using the database, a 20-page paper version of the reporting system is also available through the NCFRP website (15).
While this national reporting system is an enormous resource for child fatality data, it has several limitations. Not all child deaths are reported to the system, even within a single region. Data cannot be compared between states, or even teams, due to variability in cases reviewed (e.g., all, only homicides, everything but naturals) and the frequency of reviews (e.g., monthly, quarterly). There is often substantial delay between team reviews and when the cases are entered into NCDR-CRS.
Data quality is also a concern. Some teams input more data than others and teams may interpret cases differently. Of particular note, there is often variability in the questions concerning if a death was “preventable” or if “omission or commission” contributed to the cause of death, even between local teams within the same state.
The Role of the Forensic Pathologist
National data show that the majority of states coordinate their CDR programs through state health departments or social services, while only a handful of states (5.9%) coordinate their CDR programs through a medical examiner office (9). However, medical examiners/forensic pathologists have been heavily involved in CDR from the beginning. Of the states that have laws defining state and/or local CDR membership, over 30 specifically require the involvement of medical examiners or forensic pathologists (16).
The forensic pathologist is uniquely positioned to serve on multidisciplinary CDR teams. Determination of cause and manner of death requires the forensic pathologist to correlate autopsy findings with medical history, family and social history, and death scene investigation. Because of this access to history, medical records, autopsy results, and death certificates, the forensic pathologist often acts as gatekeeper, identifying cases for state and local review. Some states mandate that the medical examiner or coroner identify which cases will be forwarded to the state team for examination.
During the review of a case, CDR teams may question the certification of cause and manner of death. A medical examiner may be able to explain to the team the logic of the certification based on the available findings or why certain cases are traditionally certified in a certain way. This often increases understanding between local agencies by clarifying terminology or dispelling misconceptions. For instance, law enforcement and child protective services may not understand why a forensic pathologist certifies a suspicious case as “undetermined.”
Sudden unexplained infant deaths are often a source of confusion in CDR. Phrasing of the cause and even manner of death can vary significantly from one jurisdiction to another. For state reviews in particular, it may be confusing to see similar cases ruled as “SIDS” with a manner of “natural” in one county and “SUID” with a manner of “undetermined” in another county. It can also be unclear to team members why one case involving unsafe sleep practices may be undetermined while another may be ruled accidental. A forensic pathologist on the team can sometimes clarify these distinctions. On the other hand, it is also possible, especially in the light of additional investigative information provided during review, that the forensic pathologist may be of the opinion that the original cause and manner are incorrect.
Involvement in CDR can be insightful and rewarding to a forensic pathologist. As the mission of most CDRs is prevention of injury and death, forensic pathologists have much to contribute in addition to just the cause and manner of death. Although the forensic pathologist may have the best insight into prevention measures, unfortunately, some are unfamiliar with prevention programs within their states or communities. Getting involved in local prevention campaigns or activities can bring welcome positive attention to local medical examiners and what they provide to the community.
Limitations of Child Death Reviews
Most states provide limited funding for child death review, most commonly through state health departments or social services (8). This funding is typically at the state team level and may cover a coordinator or training opportunities. Many local teams receive no funding assistance, though some are lucky enough to receive city or county support. Some teams are supported through local advocacy centers, medical examiner offices, and injury prevention centers.
Nationally, funding for CDR increased between 2004 and 2008, but then saw a drop in several states corresponding to the recession. Recent years have shown an increase in financial support and the NCFRP reported significant increases in funding for six states in 2017 (9).
Most local teams lack significant funding for coordinators. Due to the voluntary nature of most local review teams, it is sometimes difficult to encourage participation. In large counties with multiple law enforcement agencies, it can be difficult to encourage those agencies to participate in review, especially if they are not regular team members. Having a local designated (and paid) coordinator can assist greatly in the organization of CDR, collection and reporting of data, and increase participation by agencies.
Team Recommendations
In 2016, 42 states reported advisory boards that make prevention recommendations to state officials and the public (9). State and local CDR teams are not only tasked with reviewing child deaths and collecting data, but also making recommendations for the prevention of additional deaths. In states that support local and state teams, the local teams usually make recommendations to the state team, and the state team drafts proposed recommendations/legislation to the state itself in the form of annual reports. A team may recommend and implement media campaigns to highlight certain risk factors, implement new programs through state agencies, or recommend changes to existing laws. Popular topics have included gun safety, distracted driving, unsafe sleep environments, suicide prevention, drowning, and vehicular hyperthermia. Despite the many efforts of CDRs around the country, it is often difficult to link these recommendations to measurable outcomes.
A 2011 study by Wirtz et al. assessed the quality of written CDR recommendations and provided guidance for improvement of these recommendations (17). Their analysis of CDR recommendations found that teams were better at problem assessment but fell short on written recommendations and acting upon those recommendations. While many teams made multiple recommendations a year, teams felt that little to no progress was made. The authors suggested best practices for constructing written recommendations
Writing Recommendations (16)
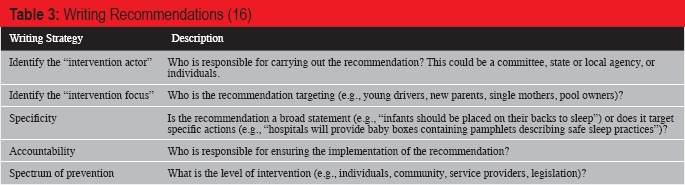
Common areas for potential prevention measures include unsafe sleep in infants, water safety, vehicular events (e.g., distracted driving, pedestrians and back overs, car seats, restraints and airbags, driving while intoxicated, and driver education), and gun safety.
International Teams
The first international CDR teams were located in British Columbia, Canada and New South Wales, Australia. Since then, teams have also been established in the United Kingdom, New Zealand, and the Philippines. At the time of this publication, only the United States and New Zealand have national data collection systems (18).
Similar to the US, most Canadian provinces have a CDR process, but there is extensive variation in structure and reporting (19). Canada currently struggles with national data collection, data standardization, and coordination of national preventative measures. A data collection system, such as the NCDR-CRS used in the United States, would be beneficial.
In Japan, the Ministry of Health, Labor, and Wellness established a committee to review child abuse cases and make recommendations to each region (20). Organizations including the Japan Pediatric Society and the Japanese Society of Legal Medicine are strongly in support of a CDR system that includes regional teams, but as of this publication a formal CDR system has not been implemented (21).
Child Death Review Impact
Child death review teams across the country have initiated hundreds of local and state prevention programs, conducted local and regional training on child death investigation and the CDR process, and collected data on approximately 189 000 child fatalities (8). There are many examples of preventive programs throughout the country focusing on infant safe sleep, water safety, firearm safety, motor vehicle safety, child abuse and neglect, and suicide prevention.
Vehicular safety has many different areas of intervention. Current legislative measures and media campaigns are focusing on distracted driving, including phone use and texting. In some jurisdictions, it is believed that distracted driving contributes to more motor vehicle accidents than alcohol. The consistent and correct use of infant car seats is a frequent focus of local CDR teams and injury prevention groups, and some teams organize yearly activities at day care centers and schools to increase awareness. Child roll-over mortality data from CDR teams and the NCDR-CRS contributed to the current requirement for all cars to have back-up cameras. Vehicular hyperthermia data has led several states to enact legislation specifically addressing children left unattended in a vehicle. Eleven states specifically protect citizens from civil liability if they break into a car to rescue a child or pet (22). Currently, the Helping Overcome Trauma for Children Alone in Rear Seats Act (HOT CARS Act, H.R. 6041) proposes that manufacturers of new vehicles develop a system to alert drivers of unattended children.
Drowning in residential pools, lakes, and other bodies of water have triggered numerous CDR recommendations and activities. Residential regulations may require specific fencing around newly constructed pools. Many states and counties have various water-safety campaigns as the summer begins. In Houston, Texas, “April Pools Day” is an annual event that includes a media campaign promoting water safety as well as multiple activities including cardiopulmonary resuscitation training.
Safe sleep initiatives have included programs to provide safe sleep environments (e.g., cribs, Pack-n-Plays, and baby boxes). Educational materials and media coverage continue to encourage the supine position and discourage bed-sharing.
In response to several case reviews, the Texas State Child Fatality Review Team recommended a birth match system that alerts Child Protective Services (CPS) to new births to parents who had a child die of maltreatment or who had parental rights terminated due to abuse or neglect. In 2013, the Departments of Family Protective Services and State Health Services worked together to develop Project HIP (Helping through Intervention and Prevention), which identified these families and triggered CPS visits, providing monitoring and services if necessary. Since the implementation in 2014, the program has led to additional support services for some families and removal of infants found to be at risk.
CONCLUSION
There is significant variability in the size, scope, and budget of CDRs across the nation, but all 50 states are now involved in CDR. The NCDR-CRS continues to collect and standardize CDR data across the nation and provide a resource for safety and prevention initiatives. New efforts by team coordinators and the NCFRP seek to standardize national data by comparing and improving state and local team responses to questions in the NCDR-CRS. State coordinators continue to support the formation of local and regional teams in an effort to achieve 100% coverage of all child deaths in the country. There is a national movement to increase collaboration between CDRs and other review teams (e.g., FIMR and domestic violence review teams). Finally, those who participate in CDR continue to advocate for increased financial support in an effort to translate CDR findings into preventive programs. States and the NCFRP could benefit from the development and monitoring of outcome measures that would better highlight the positive impact of CDR. These outcomes could be monitored through local injury prevention centers or state and local health departments.
Child death review has made a positive national impact on the health and safety of infants and children and it is the hope of all teams that prevention efforts will reduce the number of child fatalities in the United States.
Footnotes
ACKNOWLEDGEMENT
The author would like to thank Amy Bailey, Texas Child Fatality Review coordinator, for her valuable assistance on this project and her ongoing work with CDR in Texas.