
Abstract
High altitude illness (HAI) is the current accepted clinical term for a group of disorders including acute mountain sickness (AMS), high-altitude cerebral edema (HACE), and high-altitude pulmonary edema (HAPE), which occur in travelers visiting high-altitude locations. High-altitude illness is due to hypobaric hypoxia, is not associated with age or physical conditioning, and mild forms are easily treated. High-altitude cerebral edema and HAPE are medical emergencies that are fatal if not promptly treated and fortunately are uncommon. The cause of most high-altitude fatalities is not related to HAI and can be easily distinguished from HACE and HAPE; however, other causes of death may have symptoms and physical findings that overlap with HAI, making postmortem diagnosis challenging. Fatalities due to HAPE and HACE are diagnoses of exclusion. Medical examiners and coroners who work in jurisdictions with high-altitude locations should be aware of the risk factors, physiology, pathology, differential diagnosis, and classification of HAI to accurately recognize HAI as a cause of death. Medical examiners who do not work in jurisdictions with high-altitude locations may be asked to evaluate deaths that occur overseas associated with high-altitude trekking and mountaineering activities.
Keywords
Introduction
Travel to high-altitude regions and mountainous areas has become increasingly popular for tourism, recreation, adventure activities, and sometimes rescue missions. Hackett and Roach estimate 30 million people travel to mountainous regions of the western United States annually (1). Tens of thousands of travelers visit high-altitude destinations throughout the world each year and many travelers will experience symptoms of high-altitude illness (HAI) (2). Acute mountain sickness (AMS) is the most common form of HAI. Fifteen to forty percent of people traveling to Colorado from elevations less than 914 m (3000 ft) will develop AMS when they arrive and stay overnight at 2438 m (8000 ft) or higher (3). Acute mountain sickness is not fatal and therefore not encountered by medical examiner/coroner systems. High altitude pulmonary edema (HAPE) and high altitude cerebral edema (HACE) are fatal if not treated promptly. Fortunately, HAPE and HACE are uncommon compared to AMS. This was evident in a study conducted by Chen et al. with 339 young adult volunteers who resided at sea level and then traveled to 3200 m (10 500 ft) in 48 hours (4). Of the 339 volunteers in the study, 58 developed AMS using AMS-Lake Louise Scoring criteria, two developed HAPE, and none of the volunteers developed HACE.
The most common causes of death at high altitude include, but are not limited to hypothermia, blunt force trauma, avalanche-related deaths, carbon monoxide intoxication, lightning, hyponatremia, drug and alcohol intoxication, and preexisting natural disease. As an example, the Colorado Avalanche Information Center (5) alone has documented an average of 27 avalanche-related deaths per year in the United States over a ten-year period. These avalanche-related deaths involve skiers, hikers, snowshoers, climbers, and individuals pursuing other activities. These deaths do not include non-avalanche related trauma such as falls. Lightning deaths in all states between 2007 and 2016 averaged 30.5 cases per year and hypothermia deaths in all states between 1999 and 2011 averaged 1301 per year (6, 7). Lightning and hypothermia deaths are not reported with specific association to high-altitude, but are frequently encountered at high altitude. While some causes of death are easily differentiated from HAI, significant clinical overlap occurs and differentiation from natural disease, metabolic disorders, and effects of drugs and alcohol can be problematic. Knowledge of the forms of HAI, high-altitude physiology, and HAI associated pathophysiology is important.
Discussion
Physiology of Altitude
The key to understanding the physiology, and therefore the pathophysiology, of altitude illness is to appreciate the concept of partial pressure. At sea level, the barometric pressure (PB) is 760 mmHg and at 5791 m (19 000 ft), the PB is one-half or 380 mmHg. The concentration of oxygen remains at 21% throughout the troposphere, but the partial pressure of oxygen decreases with decreasing barometric pressure on ascent to high altitude, such that at 5791 m, the pressure of oxygen is 75 mmHg versus 150 mmHg at sea level. It is the partial pressure of the inspired gases, not the actual percentage of the gas present, that dictates physiologic changes. Therefore, during an ascent to altitude the individual experiences a gradual decrease in oxygen partial pressure, which can lead to HAI.
Unlike what is seen in an underwater environment, the nitrogen present in inspired air is of little consequence at altitude. Decompression sickness can occur with altitude exposure, but the change in altitude typically has to take place very rapidly, as would occur with flight in an unpressurized aircraft or loss of cabin pressure in a previously pressurized aircraft.
Pathophysiology of Altitude
The primary pathophysiologic event that causes HAI is hypobaric hypoxia with resulting hypoxemia. Decreased partial pressure of oxygen (PO2) in arterial blood due to the decreased partial pressure of inspired oxygen is sensed in the peripheral carotid body receptors and hyperventilation ensues as a compensatory mechanism. Hyperventilation causes hypocapnia and respiratory alkalosis. Due to respiratory alkalosis, the central chemoreceptors in the medulla limit the increase in ventilation until acclimatization is achieved by increased renal elimination of bicarbonate. Ventilation will increase following attenuation of alkalosis. If the altitude gain is tolerated without HAI, sustained exposure will lead to acclimatization. Acclimatization is also accompanied by a gradual shift in the hemoglobin dissociation curve, an increase in erythropoiesis, and an increase in capillary angiogenesis. These physiologic responses may begin with exposure to altitudes as low as 2000 m (6500 ft) but are insufficient to allow for acclimatization to extreme altitudes such as 5486 m (18 000 ft) or higher (8).
Hypoxemia results in cerebral vasodilation and increased cerebral blood flow, creating an overall increase in cerebral blood volume and edema. Pain sensitive areas in the brain include arteries, veins, dural sinuses, and the meninges and may account for early symptoms of AMS. These symptoms may include headache, nausea, and general malaise. Imaging studies of patients suffering from AMS have demonstrated a small amount of cerebral edema in some cases (9). If the process ends here, typically the individual has not progressed beyond AMS and intracranial pressure will normalize, resulting in complete resolution of symptoms. Untreated AMS may progress to severe AMS and HACE when increased intracranial pressure persists and cerebral edema is universally present. In one magnetic resonance imaging (MRI) study, seven of nine patient's findings included increased T2 signal in white matter areas, particularly in the splenium of the corpus callosum and suggested a vasogenic mechanism (10). The exact pathophysiology has not been elucidated, though the involvement of biochemical, mechanical, and cytotoxic pathways have been proposed.
In contrast to the cerebral circulation, pulmonary hypoxia causes pulmonary vasoconstriction, variable increase in pulmonary vascular resistance, and increased pulmonary artery pressure. The proposed mechanism for development of HAPE is uneven hypoxia-induced vasoconstriction resulting in increased pressures in capillary beds, subsequent fluid shifts, and vascular leakage (11). Disruption of the endothelial barrier results in fluid, proteins, and even hemorrhage into alveolar spaces (12). On a molecular level, the proposed mechanisms for the development of pulmonary edema at altitude include the nitric oxide pathway, the renin-angiotensin system, heat shock protein, pulmonary surfactant proteins, and hypoxia inducible factor (13).
Acute Mountain Sickness
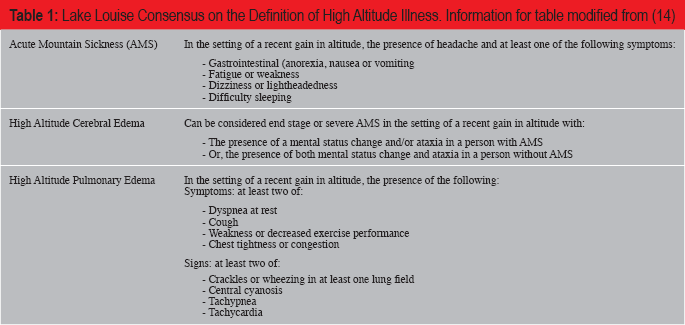
Acute mountain sickness may develop in hours, but typically not beyond 24 hours, is not fatal, and is easily treated. The most common symptom of AMS is headache, but other symptoms must be experienced to meet the criteria to be defined as AMS. During the 1991 International Hypoxia Symposium held at Lake Louise in Alberta, Canada, The Lake Louise Criteria for the diagnosis of HAI were defined by a group of experts (
Lake Louise Consensus on the Definition of High Altitude Illness. Information for table modified from (14)
High-Altitude Cerebral Edema
High-altitude cerebral edema may occur following severe AMS when increased intracranial pressure persists and frequently develops as a complication of hypoxia due to HAPE. High-altitude cerebral edema may develop without preceding symptoms of AMS. In the setting of a recent altitude gain, the diagnosis of HACE depends on the development of ataxia or mental status change in a patient with AMS. Alternatively, in patients without AMS, development of both ataxia and mental status change can be used to diagnose HACE. The mental status changes may include drowsiness, behavioral changes, and confusion. Focal neurologic deficits are not characteristic. Imaging studies demonstrate acute cerebral edema with fattening of the gyri.
High-Altitude Pulmonary Edema
As with AMS and HACE, the diagnosis of HAPE is based on the history of recent altitude gain with the presence of at least two of the following symptoms: dyspnea at rest, cough, weakness or decreased exercise performance, and chest tightness or congestion; combined with at least two of the following signs: crackles or wheezing in at least one lung field, central cyanosis, tachypnea, and tachycardia. High-altitude pulmonary edema typically occurs within the first two to four days of ascent and most often on the second night (3). With frank pulmonary edema, production of pink frothy sputum may occur. A chest radiograph typically demonstrates patchy lung infiltrates and a characteristic arterial blood gas measurement would show a respiratory alkalosis with severe hypoxemia.
Risk Factors
High-altitude illness tends to afflict individuals who are exposed to altitudes greater than 2438 m (8000 ft), although there is great individual susceptibility and physical fitness does not impart any protection. Different authors have stratified the altitude exposure into categories with varying cutoffs, but most agree that there is significant physiologic stress to an individual who travels from sea level to an altitude of 2438 m or higher and that extreme altitude exposure is reached at 5486 m (18 000 ft) or higher (8, 10). Davis and Hackett roughly organize altitude stages as intermediate (1524 m to 2438 m), high (2438 m to 4267 m), very high (4267 m to 5486 m), and extreme (above 5486 m) (10). In general, the predictability and severity of HAI increases with increasing altitude gain.
Risk factors for developing high-altitude illness have been proposed, though not all researchers are in agreement. In general, risk factors can be grouped into behavioral and biologic. Behavioral factors that increase risk include, but are not limited to altitude gained, rate of ascent, insufficient time spent for acclimatization prior to ascent and/or at stages of continued ascent, physical exertion, use of drugs that suppress respiration, and alcohol use. Factors that decrease risk include pretreatment with a carbonic anhydrase inhibitor to promote acclimatization, oxygen use, and adequate hydration. Biologic factors that increase risk include, but are not limited to individual sensitivity to hypoxia, past history of HAI, diseases that compromise oxygen carrying capacity, sickle cell disease, congenital heart disease, some diseases that compromise pulmonary function, and genetic variation. Asthma is not considered a risk factor for HAI by some sources and asthma symptoms may actually improve at high altitude (3). Factors that may predispose more specifically to the development of HACE include preexisting space occupying intracranial lesions/masses or any condition that increases intracranial pressure.
Individuals who already reside at an altitude above 1500 m (5000 ft) are less susceptible to exposure to increased altitude, presumably the result of acclimatization. One study found female gender, obesity, and underlying pulmonary disease to be risk factors for high altitude illness (16). Another group of researchers noted no correlation between gender and the development of high-altitude illness, but concluded that poor or average health, no prior altitude exposure, and age less than 55 years to have a positive correlation with the development of disease (17). It is unclear if dehydration due to increased water vapor lost from pulmonary sources contributes to the development of high altitude illness (1).
Postmortem Examination
A complete postmortem examination should be performed to evaluate deaths that are associated with high altitude. Like drowning death investigation, death due to HAI is a diagnosis of exclusion. All organ systems should be evaluated including a complete neck dissection. On a case-by-case basis, evaluation of the cardiac conduction system and/or investigation for a possible genetic conduction system abnormality should be considered. Microscopic examination should be performed routinely. Postmortem radiography including routine views or whole-body computed tomography scan may have value and should be considered on a case-by-case evaluation. Complete toxicologic examination should be considered routine in all HAI suspected deaths. Vitreous analysis is essential, especially to evaluate for hyponatremia, which may be difficult to differentiate from HAPE and HACE. The postmortem examination findings of pulmonary edema and diffuse brain swelling are not specific and therefore require careful evaluation to exclude other causes and to identify factors that may promote susceptibility to HAI. All information must be correlated with the findings of the death investigation and medical history.
Case Examples
Case 1
A 41-year-old male was hiking with his three children ages 15, 13, and 7 in mid-July in a mountainous, remote wilderness area for days when they were caught in a rain and lightning storm and sought shelter in their tent at approximately 3071 m (10 076 ft) elevation. Wet, cold, and shivering due to rain and a precipitous temperature drop, a camp stove was used to heat water and to warm the tent interior. Hours later, the 15-year-old child woke-up and felt nauseated and cold. Her 7-year-old sibling also woke-up, was hallucinating, and thought snakes were in their tent. Their 13-year-old sibling was status post congenital heart repair and was cold and unresponsive. Their father was cold and unresponsive. Their camp stove was tipped over and between their father's head and a tent corner (

View of stove and decedent location at tent corner.

View of decedent from tent interior.

Exterior view of tent with position of both decedents.
Case 2
A 65-year-old male hiker who lived at 1524 m (5000 ft) elevation was hiking with two companions. They hiked to 3657 m (12 000 ft) in one day and his companions last saw him alive at 10 pm. He was discovered unresponsive lying face-up in his tent the following morning (

View of decedent in tent with intraoral device.
Postmortem examination revealed marked pulmonary edema (right and left lung weights of 1026 g and 838 g, respectively), patchy areas of intra-alveolar hemorrhage (
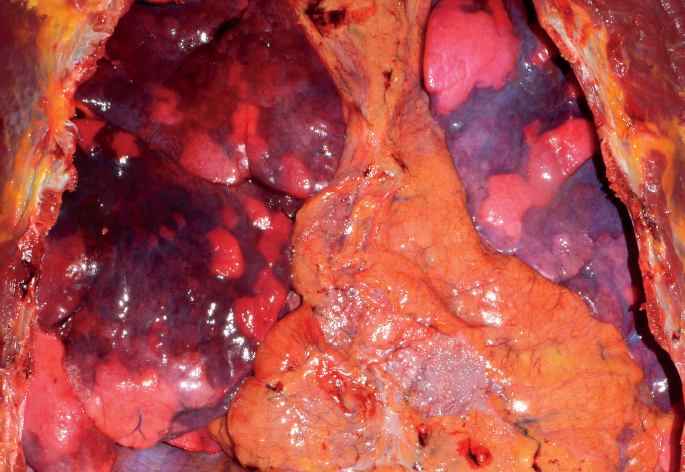
Thoracic cavity depicting lungs with edema and intra-alveolar hemorrhage.
Case 3
A 20-year-old female who lived at sea level few to Colorado and spent her first night at 1609 m (5280 ft) elevation. The following day, she departed to spend two days at 2784 m (9134 ft) and then departed for a hike to camp at 3413 m (11 200 ft). She consumed marijuana edibles at the beginning of the hike. Along the way to her destination, she experienced dizziness and wheezing and continued hiking after using a companion's inhaler. Upon reaching their destination, she became confused, was vomiting, and attempted to descend, but stayed at altitude due to darkness. She stopped eating and drinking and her neurologic status continued to decline. Emergency medical services were contacted; however, upon their arrival she had stopped breathing and had foam coming out of her mouth. Resuscitation efforts were to no avail. Postmortem examination revealed marked cerebral edema (
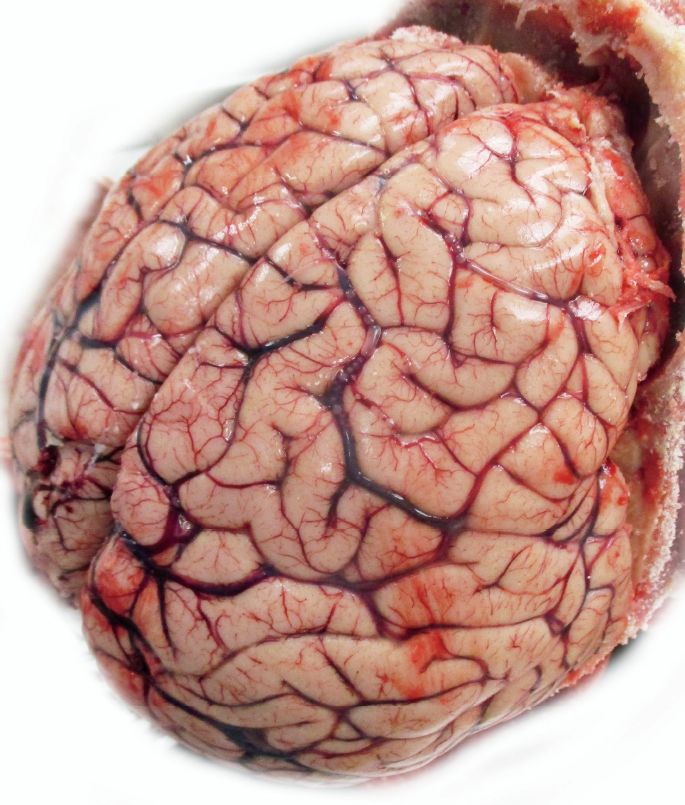
Diffuse cerebral edema.
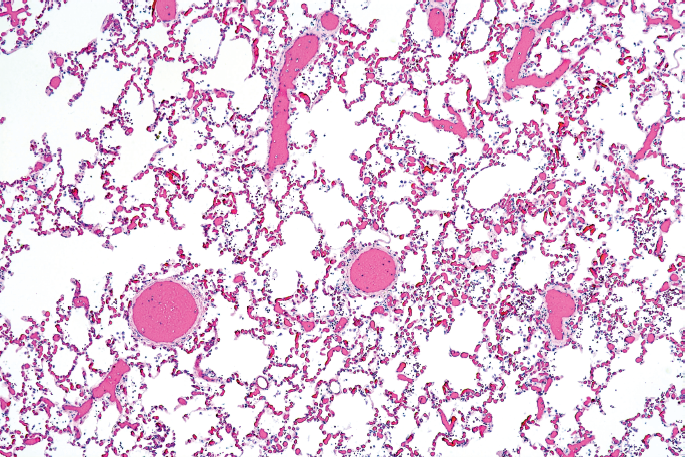
Low power view of lung with pulmonary congestion (H&E, x40).
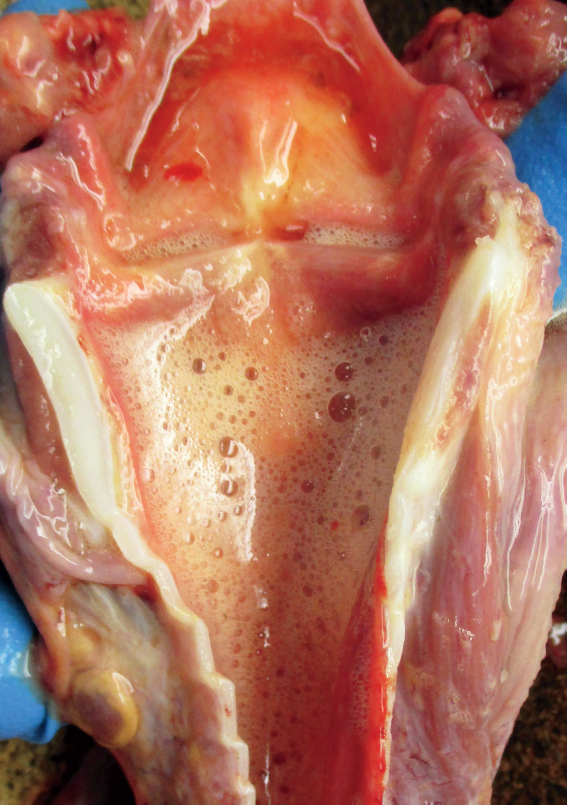
Froth in larynx.
Cases 4 and 5
Case 4 involved a 29-year-old male from Colorado who lived at 1402 m (4600 ft) elevation, traveled to Africa to participate in a six-day trek to the summit of Mt. Kilimanjaro, and arrived at 894 m (2933 ft) elevation. He traveled to the first destination at 2134 m (7000 ft) on day one and in the ensuing days reached 5486 m (18 000 ft). Initially, he did not experience problems; however, days later he developed a headache, fatigue, and cough. He was advised to descend, but refused. That evening his condition deteriorated. He developed rales, tachycardia, pallor, and became unresponsive. An evacuation team was arranged, transport to the nearest hospital was planned and initiated, but death occurred before the evacuation was completed. Case 5 involved a 37-year-old male from Colorado who lived at 1402 m (4600 ft) elevation, traveled to Africa to participate in a trek to the summit of Mt. Kilimanjaro, and arrived at 894 m (2933 ft). He had no significant preexiting disease and no past high-altitude experience. He trekked to 3962 m (13 000 ft) and experienced difficulty sleeping, weakness, and fatigue, and could not proceed further. Ataxia and dyspnea were not observed. Two porters helped him descend; however, only 800 m (2624 ft) were descended in two days. The remainder of the descent took place in one-half day. He did not use supplemental oxygen, continued to deteriorate, and had to be carried. He was admitted to the hospital in respiratory distress, administered furosemide, developed cardiopulmonary arrest, and could not be resuscitated. Postmortem examination revealed severe HAPE. Both cases present investigation challenges due to a death occurring overseas and the need to rely on potentially limited death investigation in a remote area. Information collection in nonmilitary overseas deaths can be facilitated with the adventure/travel companies, local authorities, and health care. The State Department is an additional resource. Case 4 had a clinical review performed by a HAI expert and the features were considered typical of HACE and HAPE. A postmortem examination performed overseas specifically listed diffuse brain swelling. However, upon return to the United States, a second postmortem examination was performed. A coronal incision typical for examination of the brain was present, but the calvaria was not incised and brain was not examined as previously reported. Despite the erroneous reporting, the brain did have diffuse swelling. Case 5 was also reviewed by a HAI expert and classified as atypical HAPE. In this case, the clinical presentation was considered atypical due to lack of respiratory symptoms despite pulmonary edema and marked hypoxemia; this can be observed in persons with absent or poor carotid body response to high altitude hypoxia. A second postmortem examination was not performed in this death, but review of the first postmortem examination report was requested.
Manner of Death
Based upon general principles and recommendations in the National Association of Medical Examiners “A Guide For Manner of Death Classification”, prepared by Hanzlick, Hunsaker, and Davis, the manner of death in fatalities due to HAPE and/or HACE are best classified as accident (20). High-altitude pulmonary edema and HACE are generally not predicable and are the unintended consequence of exposure to a hostile environment. In Case 1, the manner of death was easily classified as accident. In Case 2, the manner of death was classified as accident by one of the authors; however, an argument could also be made for a natural death. In the opinion of the authors, the manner of death in Cases 3 to 5 is best classified as accident. As in all death investigations, careful review of the circumstances is warranted to fully evaluate factors involved in death.
Conclusion
Deaths due to high-altitude illness are uncommon and successful diagnosis is dependent upon complete review of circumstances including detailed travel history, medical history, detailed report of symptoms, and detailed report of physical findings prior to death combined with a complete postmortem examination, toxicology, vitreous electrolyte determination, and other special examinations as indicated on a case-by-case evaluation. Due to increasing travel to high altitude locations for recreation, adventure, tourism, and work-related activity, the incidence of HAI will likely increase. It is important to recognize that acute mountain sickness is not a fatal condition, whereas HACE and HAPE are serious conditions and will progress to death in hours to days if not recognized and treated. Advances in the understanding, recognition, and diagnosis of HAI, particularly HACE and HAPE, will help advance HAI awareness and strategies to prevent HAI morbidity and mortality.
Footnotes
Acknowledgements
The authors wish to thank Dr. S. Ayers, Pitkin County Coroner's Office, Garfield County Coroner's Office, Dr. Dawn Holmes, and Dr. Peter Hackett.