
Abstract
This paper explores the pathology caused by lightning. It covers the basic physics and mechanisms of injury of lightning strikes followed by a short discussion. The purpose of this paper is to suggest an approach to the investigation and autopsy of a lightning-related death.
Introduction
The Roman author Pliny noted that “the man who sees the lightning flash and hears the thunder, is not the one struck” (1, 2).
The medicolegal and forensic perspectives surrounding a lightning strike have been highlighted in the newer literature as early as 1995 (3). Lightning may be defined as a transient, high-current electric discharge whose path length is generally measured in kilometers. The electric current involved in lightning strikes is direct current (DC) in the order of 30 000 to 50 000 Amperes (4).
Lightning may be thought of as a nonkinetic energy with multiphysics phenomena. The electrical engineering literature classifies lightning as upward lightning, downward lightning, negative lightning, positive lightning, or combinations thereof (5, 6). Ninety percent of lightning is negative downward lightning and positive upward lightning accounts for approximately 10 % (5.3 to 15.4%) of lightning discharges (7) (

A typical lightning discharge. Photograph courtesy of Dr. Neale du Plooy, Pretoria, South Africa.
Keraunopathology is the study of lightning-induced pathology or damage, (from the Greek: keraunos, thunderbolt + pathology). It is estimated that there are approximately 6000 to 24 000 lightning fatalities per year globally (8). Underreporting of lightning fatalities may be due to multiple factors including failure to report and misdiagnosis. It is important, therefore, for forensic pathologists to be familiar with lightning and lightning strike deaths.
Lightning has four main physics components, which may cause injury, namely light, heat, electricity, and barotrauma. The pathologist must therefore think in terms of these four physics components when seeking out keraunopathology. To date, six mechanisms have been described in the mainstream medical literature regarding lightning injury mechanisms (8). Briefly, these mechanisms are: 1) direct lightning strike; 2) indirect lightning strike (caused by contact with an object, such as a pole or a tree, that was directly struck; 3) a side flash (from a struck object, such as a tree, near the victim); 4) a person or animal standing near a struck object, or close to a flash of lightning, injured by step voltages produced by a lightning current flowing through the resistance of the soil beneath (this earth current may then flow in another pathway, namely, up one limb and down another of the victim, which may result in injury or even death); 5) bodies may become sufficiently charged during the lightning leader development process to cause upward streamers to be initiated from them, leading to injuries; and 6) a “pressure-shock wave” immediately surrounding lightning's luminous channel.
Lightning victims may present with minor lightning injury, moderate lightning injury, or severe lightning injury. This is almost tantamount to the “dose” of lightning to which the victims were exposed. The “dose” would depend upon aforementioned six mechanisms.
The purpose of this paper is to suggest an approach to the investigation and autopsy of a lightning-related death and hopefully serve as a reference text to refer to if one encounters such a case.
Discussion
Injury Due to the Light Component
Lightning may injure the eye and there is a relatively large body of literature describing such injuries (9–12). As such, in selected cases one may want to examine the retinae. Some authors suggest an opthalmic endoscope or an intraocular oculoscope in examining the eye after death; however, a trephine removal of the cornea at autopsy could probably be a cost-effective way to examine the eye postmortem (13). Bisecting the eye may also be a good way to examine the retina.
Ocular lightning-induced injuries have caused uveitis, cystic macular edema, macular holes, optic neuropathy, eyelid lesions, corneal lesions, thermal papillitis, retinal folds, retinal vein occlusion, bilateral iridocyclitis, and rhegmatogenous retinal detachment. The most common ocular injury from lightning is a cataract with posterior subcapsular damage (14–15). Cataracts typically develop approximately three to six months after the lightning strike incident. As such, retinoscopy may not be worth performing on a regular basis in acute lightning-related deaths. Lightning has been known to cause cataracts for almost three hundred years. Multiple theories exist as to why cataracts develop post-lightning strike (16). Injury to the protein lattice structure of the lens seems to be the most plausible theory for the development of such cataracts. Cataract surgery and lens implantation are typically performed by opthalmologists in such cases, with good results. These may be important to look for, should a lightning victim die at a later stage.
Injury Due to the Heat Component
The temperature of the lightning stroke varies with the diameter of the stroke and has been calculated to be approximately 8000°C (14 400°F). Other estimates of the temperature are as high as 50 000°C (90 000°F). After a few milliseconds, the temperature falls to 2000 to 3000°C (3600 to 5400°F), similar to the temperature of a high-voltage arc (8).
Oftentimes, there are linear, first-degree burns, which may follow the skin creases. These marks may be inches long and generally follow the long axis of the body towards the ground. There is often a smell of singeing or burning about the body and its clothing. The hair may be scorched or singed. There may also be superficial charring of the skin, chiefly over the trunk (17) (

Superficial charring of the skin on the abdomen. Note the synthetic material of the underwear which shows melting of fibres.
The likelihood of a lightning flash starting a fire when it strikes inflammable material depends on various factors, such as the intensity of the lightning current and, to a lesser extent, the rate of increase of the current with time. Before it can take fire, inflammable material has to be heated to its ignition temperature (18).
Injury Due to the Electrical Component
Metal objects on the body may “hold” onto the charge. As such, one should always take a look and comment on jewelry. For example, watches may be stopped and metal items may be magnetized. Some metal substances dissipate, leaving other metals behind (zincification or cuprification). Additionally, metal jewelry may become burned into the skin (8).
The skin lesions caused by lightning may range from very superficial stellate-type injuries (

Superficial stellate-shaped lightning injury noted on the skin of a lightning-strike survivor who survived a lightning tent strike in Witbank, South Africa 2013. Photograph courtesy of Mr. Corrie Pieters, Deputy Director and District Coordinator Nkangala District, Mpumalanga, South Africa.
Lightning may also cause the so-called “tip-toe” sign, a lightning “blow-out” laceration on the soles of the feet and/or shoes. The etiology of the “tip-toe” sign is thought to represent an electrical exit wound, similar to grounding injury seen in electrocution cases.
The most feared complication of lightning injury is cardiac arrest and cardiac dysrhythmias, both of which can occur in the immediate aftermath (22–24). Lightning injury may cause abrupt cerebral salt wasting syndrome. Cerebral salt-wasting syndrome ordinarily occurs after severe brain injury, severe cerebrovascular disease, or surgery. Hyponatremia may result in brain edema and secondary nausea, headache, altered consciousness, and sometimes death. Close monitoring of the serum sodium levels and immediate correction of electrolyte abnormalities are therefore necessary after severe brain damage. If left untreated without correct diagnosis, severe hyponatremia may result in seizures and worsening cerebral edema (25). Likewise, the electrical component of lightning may lead to rhabdomyolysis and acute kidney injury (indicated by an elevated creatinine) and delayed-onset psychiatric and cognitive symptoms, which may perhaps be due to a post-concussive syndrome (22, 26).
Post electric shock or lightning shock syndrome (PELIS) has been proposed in lightning strike survivors (27). The major neuropsychological consequences of which include depression and neurocognitive dysfunction with ongoing consequences. The proposed DSM diagnostic criteria insist on a demonstrated context for the injury, both in the shock circumstance and also in the physical consequences. The diagnostic criteria allow for a certain delay in onset of symptoms, and recognize certain exclusionary conditions.
Injury Due to the Barotrauma Component
Blast overpressure (BOP), or high-energy impulse noise, is the sharp instantaneous rise in ambient atmospheric pressure resulting from an explosive detonation, typically occurring with the discharge of weapons but may also occur with lightning strikes (28). The primary targets for BOP damage are the hollow organs, ear, lung, and gastrointestinal tract. Lightning may also cause pneumomediastinum due to the barotrauma component (29, 30). Postmortem computed tomography may help better demonstrate the pneumomediastinum. Oftentimes BOP may have biochemical and molecular mechanisms of injury. Free radical-mediated oxidative stress may occur and contribute to BOP injury. Understanding the etiology of these changes may shed new light on the molecular mechanism(s) of injury and can potentially offer new strategies for treatment (28).
The clothing of a lightning victim may be torn off and this can sometimes raise the suspicion of foul play if the lightning aspect is obscure (17). Always examine the clothing in acute lightning cases as the clothing often shows good physical evidence of lightning strike. The clothing may tear and tatter and synthetic fibers may melt. At times, the clothing tears at the seams, and at other times it may tear far away from the seams. Clothing and shoes may become brittle after a strike.
Cases are on record where lightning has exploded concrete pavement, causing fragments of exploded concrete to become embedded within the skin of the victim (31). The secondary missile fragments of concrete entering the skin are considered blunt force trauma; however, the explosive force causing the concrete to explode is due to lightning explosive barotrauma.
There are many references with regard to lightning damage of the human ear, the most common of which is tympanic membrane rupture (32) (

The lightning-damaged ear. About 29 pounds per square inch is required to produce minor eardrum ruptures.
A Comparison of Scenarios of Overpressure (or Blast Overpressure) Versus Predicted Injuries (41)
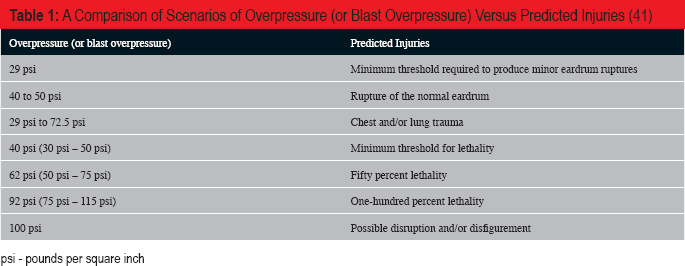
psi - pounds per square inch
Lightning may injure or kill individuals or groups of people (22). The spectrum of pathology sustained may vary markedly between individuals. Lightning strike survivors may therefore present with an array of symptoms. They may present with immediate and transient symptoms, immediate and prolonged or permanent symptoms, possible delayed neurologic syndromes or lightning-linked secondary trauma from falls and/or blast (8). For example, lightning injured 44 Ranger School participants during a training exercise on August 12, 2015, at Camp Rudder, Florida. Of the 44 victims, 20 were admitted to the hospital. One patient had cardiac arrest. This patient, along with two others, was admitted to the intensive care unit. Seventeen other patients were admitted for observation for rhabdomyolysis and/or cardiac arrhythmias. One patient was admitted with suspected acute kidney injury indicated by an elevated creatinine. All patients, including those admitted to the intensive care unit, were released on the day following the lightning strike without restrictions and were allowed to return to duty with increased medical monitoring (22).
Lightning may kill a person instantaneously, or victims may die later due to complications (42). These hospital cases are relatively rare and the pathology of trauma encountered at autopsy may be surprising. One such victim, a 13-year-old girl, presented at autopsy with intramyocardial hemorrhage after spending several days in intensive care (

Intramyocardial haemorrhage in a 13-year-old hospitalized lightning-strike victim. The victim died several days after having been struck by lightning.
Lightning strike survivors may suffer hematological abnormalities, endocrine abnormalities, sexual dysfunction, psychological, and neurocognitive dysfunction. There may be memory disturbances, concentration disturbances (adult attention deficit disorder), cognitive dysfunction, and problems with higher executive functioning. Behavioral issues, such as emotional lability and aggression, sleep disturbance, phobic behavior, depression, and others have been documented in the clinical literature (8). There may be cardiac injuries, pulmonary injuries, neurological injuries (central nervous system, peripheral nerve injury, autonomic nervous system injury, even posttraumatic headaches). Burns, blunt force injuries, and explosive (blast) injuries may be present. There may be eye injuries and ear injuries. As mentioned, always examine the clothing in acute cases as the clothing often shows good physical evidence of lightning strike (43) (

Tearing-and-tattering of clothing seen in a lightning strike victim.
The fetus of a pregnant woman struck by lightning has an unpredictable prognosis. Pregnant victims require specialist management, and the fetus may die. There is scant literature on the autopsy of the lightning-stricken fetus.
Due to the relative rarity of lightning strike deaths, such deaths need to be carefully examined. Medical examiners should make every effort to attend the scene of death of lightning fatality cases (42). Consultation with other experts, such as electrical engineers, adds value. Lightning-related deaths may have surprising and unusual keraunopathology, which may easily be overlooked. Therefore, it is incumbent upon the medical examiner to seek out and report such pathological findings.
Conclusion
The take-home message is to be thorough and look for the otherwise hidden findings including skin marks (

Lichtenberg figures on the upper chest. Note also the linear burns on the neck and chest, corresponding to the wire from a pair of earbuds the decedent was wearing. Photo courtesy of J. Keith Pinckard.

Melting of synthetic fibres from heat seen in a lightning strike case.

The “tip-toe” sign in lightning often correlates with “blow-out” defects of material on the shoes.