
Abstract
How do coaches make decisions when they become concerned about a client’s mental health needs? Using a Grounded Theory approach, this U.S. based study explored key decisions made by 12 experienced coaches of physicians; a group of highly stressed professionals more likely to engage in coaching than therapy. Findings included a theory describing how coaches recognise mental health needs and make decisions about how to respond, without attempting to diagnose or treat any psychological condition. This theory, called the Decision Bridge, has general coaching implications, as well as practical application for coaching distressed physicians.
Introduction
Coaches often face decisions about how to respond when clients experience distress. They need strategies to recognise and respond to mental health needs in a coaching context, without attempting to diagnose or treat any psychological condition. This is especially important if the client is open to coaching but not therapy. Physicians comprise a highly stressed professional group who are more likely to engage in coaching than therapy, therefore coaches of physicians must prepare to recognise and respond effectively to physician distress in a coaching context.
Literature offers guidance on how mental health concerns should be handled in coaching, but the phenomenon of how coaches actually recognise and respond to client distress is an under-researched area, especially in physician coaching. This study is a window into that phenomenon.
The following sections will review literature on physician distress and the effects of coaching, describe unanswered questions, and outline the methodology chosen to investigate those answers in this study. Key findings will show how participants recognised and responded to physician distress, followed by a discussion of the Decision Bridge Theory, which emerged from this research as a model for decision-making to address mental health needs of clients. The conclusion highlights practical implications of the Decision Bridge as a tool for general coaching practice, and offers recommendations for future research.
Literature Review
Physician distress and coaching
Physicians are experiencing unprecedented levels of stress, moral injury, and exhaustion (Murthy, 2022; Mong & Noguchi, 2022). Some studies reveal deeper suffering, including self-harm and suicide (Shanafelt et al, 2021; Moutier, Myers, Feist, Feist & Zisook, 2021).
Doctors are conditioned to ignore their own suffering, and are excellent at hiding their distress (Moutier, 2018; Wong, 2020). Despite their need for support, however, physicians are significantly less likely than the general population to seek therapy, due to concerns about their reputation and license if perceived as being mentally unhealthy (Weiner, 2020; Clough, March, Leane & Ireland 2018; Gold, Andrew, Goldman & Schwenk, 2016). Fortunately, doctors are often willing to accept coaching, which carries less stigma (Gazelle, Liebschutz & Reiss, 2015).
Evidence shows that coaching interventions are effective to reduce distress and improve well-being in physicians (Boet, Etherington, Andreas & Denis-LeBlanc 2022; McGonagle et al, 2020; Dyrbye, Shanafelt, Gill, Satele & West 2019) but questions arise about the processes being used by coaches of physicians.
Diagnose and Treat or Recognise and Respond?
Coaching is not intended to
Navigating boundaries between coaching and therapy is a richly debated topic. Some argue that “crossover” must be avoided (Williams, 2003). Others maintain that some overlap is unavoidable, and can even be useful in the context of appropriate training (Bachkirova and Baker, 2018).
Psychologists debate using the client’s level of mental health as a guide for who should be coached, based on the problem of defining what a “mentally healthy” coaching client is (Buckley, 2007; Cavanagh and Buckley, 2018). While there are concerns that coaching may be used by some clients as a way of bypassing the clinical help they need, it has been noted that, for clients with “subclinical symptoms” coaching may serve as “early preventative intervention” that can help clients avoid “sliding into frank clinical symptomology” (Aboujaoude, 2020).
Legal codes define the licensure, education, and scope of practice for a U.S. psychologist or psychiatrist. However, coaching activity is restricted because no licensure or education mandate currently exists. (Jasper & Griffin, 2022).
Confusion can occur for clients or sponsors, since coaching and therapy share a toolkit of psychology-based techniques, like ACT-based Coaching (Blonna & Antiss, 2018) or Cognitive Behavioral Coaching (Williams, Edgerton & Palmer, 2010). Coaching applications of these and other techniques are not intended as mental health treatment, but they do sit on a continuum with clinical psychology interventions, which work at a deeper level (Bradwejn, 2020; Bluckert, 2005).
Recommendations from coaching literature
Coaching literature makes recommendations for recognising and responding to mental health needs of clients. Buckley (2007) says all coaches should learn to identify key signals that a client needs referral for psychotherapy, providing a detailed book as a guide (Buckley & Buckley, 2012). Hullinger and DiGirolamo (2018) outline recommendations for when and how to make this referral with a coaching client, and Cavanagh (2005) points out that it is important to have “a process for deciding” what to do, proposing questions to assess a client’s suitability for coaching if a concern arises.
These valuable resources support a coach’s understanding of what should be done. Questions remain, however, about what coaches actually do, and why. Descriptive studies are needed to answer these questions and to shed further light on effective practices.
Methodology
An interpretivist philosophy informed this qualitative research, based on the premise that humans create meanings that can be studied (Saunders, Lewis & Thornhill, 2016). The research design was based on Grounded Theory (GT) (Glaser & Strauss, 1967) using a constructivist perspective to gain insight about participants’ data through “the logic of their experience” (Charmaz, 2006:35).
Data collection took a phenomenologist approach, focusing on participants’ lived experience, to provide richer understanding of the context as unique to the circumstances of participants (Alharahsheh & Pius, 2020). Some maintain that within participants’ stories may be an interwoven story of the researcher as they gain insight about themselves (Creswell, Hanson, Clark Plano & Morales, 2007). With this in mind, I took care to reflect on my own values and experiences as a physician coach, maintaining awareness of personal assumptions during data interpretation.
Participant Selection
Purposeful sampling guided selection of 12 participants who could provide information-rich descriptions of multiple cases (Neuman, 2005; Saunders et al, 2016:301; Patton, 2002) resulting in a sample size based on number of incidents discussed (24) not just number of people interviewed (Woolsey, 1986).
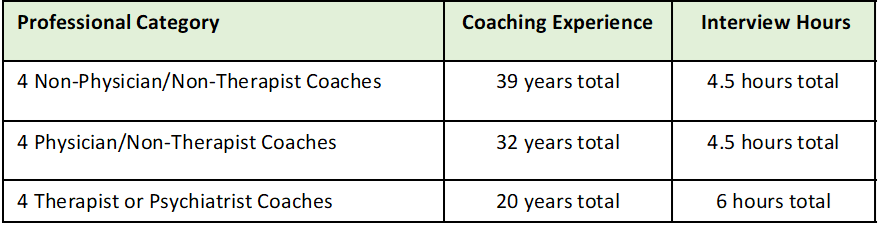
Participants were given information about the study, and were recruited in three categories, defined by their background in 1) full-time coaching; 2) coaching + medicine; 3) coaching + psychology/psychiatry. (Table 1.) Recruitment was done through professional coaching organizations, physician support groups, and outreach to experienced colleagues. Approval was granted and research conducted under the ethical guidelines of York St. John University regarding confidentiality, data security, and informed consent.
Professional Profile of Participants
Segmented Interviews
Interviews were divided into two segments. The first segment employed Critical Incident Technique (CIT) (Flanagan, 1954) using self-report of incidents to understand cognitive, affective and behavioural elements of the participants’ perspective. (Chell, 1998; Butterfield, Amundson & Maglio, 2005).
An advantage of using CIT method in GT research is that it does not involve a preconceived idea on the part of the researcher about what the respondent will find important, allowing the incident to be understood subjectively from the perspective of the respondent (Gremler, 2004:66). In behavioural interviews, Klemp & McClelland (1986) caution against letting interviewees generalize about what they usually do in typical situations and why, which does not yield much accurate information about their actual behaviour. Beginning with the CIT segment helped participants stay ‘in the story’, focused on narrative details of what happened, knowing they could comment later on what they usually do and why.
During the second segment, general questions elicited participants’ perspective on boundaries and overlaps between coaching and therapy, and on competencies and strategies for coaching distressed physicians. During the general interview segment, additional themes and sub-themes were identified, revealing a decision process that occurs between recognition and response. This developed into the core variable and Decision Bridge theory, which will be described in Findings and Discussion.
Analysis and Coding
Interviews of 60-90 minutes were conducted over Zoom, recorded using transcription software from Otter.ai, and coded manually from transcripts corrected by hand during audio playback.
The CIT segment enabled the speaker to recall accounts freely, rather than answering specific questions (Gremler, 2004). During analysis of early interviews, this facilitated identification of primary themes based on patterns in the narratives about what was going on (thoughts, feelings, behaviors) when the coach “recognised” distress, and what was going on when they “responded” to it (Chell, 1998).
Quotes were disassembled and reassembled in categories relevant to “Recognised” or “Responded”, and sub-categorised according to the “thoughts” “feelings” and “behavior” of the coach during that part of the story. These categories led to major themes identified in each area. Subsequent interviews contributed to the support or adaptation of that theme, and in some cases sub-themes became evident. (Braun & Clarke, 2006, 2021; Boyatzis, 1998).
An abductive approach to theory development was used, moving between induction (observing patterns to develop a theory) and deduction (testing of the theoretical proposition) to arrive at the “most plausible interpretation of the observed data” (Charmaz, 2006:186). Through memoing, constant comparison of data, and contrasting with activities coded differently, a stable set of themes and subthemes were created (Denscombe, 2007). Thematic saturation was reached at the “new information threshold”, when data from new interviews contributed no new information to the theory (Guest, Namey & Chen, 2020).
Findings
To answer the question “How do experienced coaches recognise and respond to mental health needs of physicians?”, 12 coaches from nine U.S. states were interviewed. All had Masters, PhD or MD level education, with additional training in coaching, psychology, and healthcare, plus 91 combined years’ experience coaching physicians. Over a nine-week period, 15 hours of interviews yielded 24 incidents coaching distressed physicians. Seven incidents involved risk of harm or suicide, or distress over suicide of a colleague. In 12 of 24 incidents, coaches referred clients to therapy.
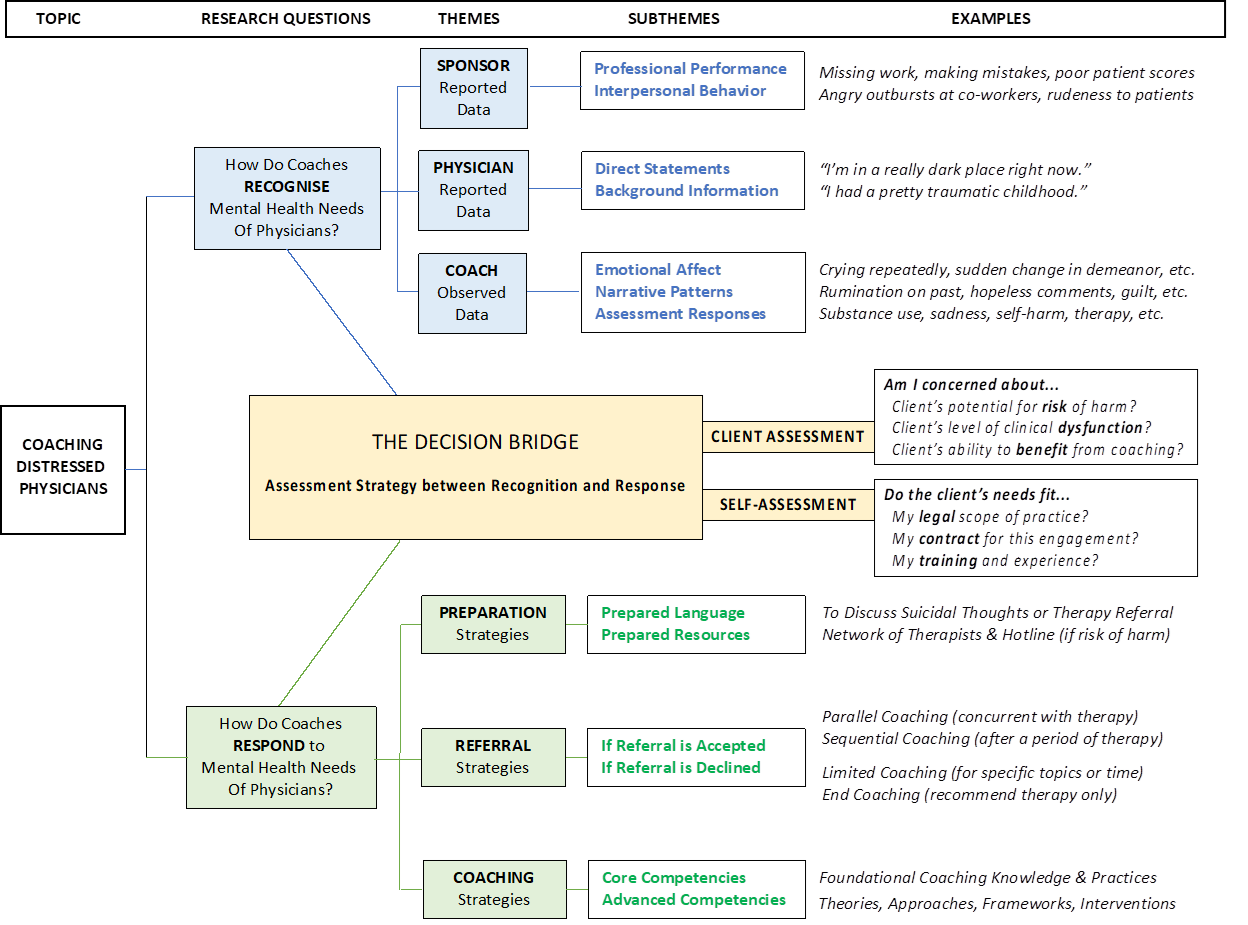
Three themes and seven subthemes were identified showing how coaches
Table 2 outlines the overall structure of these findings as a
The Decision Map: How Coaches Recognise and Respond to Mental Health Needs of Physicians
Recognising Physician Distress
Recognition Theme 1: Sponsor-Reported Data
In 5 of 24 stories, the first indication of physician distress had been information from a sponsor or administrator who referred the physician for coaching. These included two sub-themes; concerns about the physician’s
While coaches considered sponsor-reported data a valid potential indicator of distress, they sought to put these behaviours into context by eliciting the perspective of the physician-client about their working environment and personal background.
Recognition Theme 2: Physician-Reported Data
In all 24 stories, coaches described gaining insight through two sub-themes of physician-reported data. One involved
Recognition Theme 3: Coach-Observed Data
In all 24 stories, coaches described indicators of physician distress that were noted through direct observation. These observations developed into three sub-themes; observation of
Responding to Physician Distress
Response Theme 1: Preparation Strategies
In 7 of 24 incidents, conversations included suicide of a colleague or suicidal thoughts. In 12 of 24 incidents, therapy was recommended. Coaches described two sub-themes of preparation;
Some described feeling unprepared the first time the topic of suicide or self-harm came up with a client, or the first time they needed to recommend therapy. Others said preparation and practice for these conversations had been integral to their training.
Response Theme 2: Referral Strategies
All 12 coaches described referring clients to therapy at some point in their practice. Two sub-themes were identified based on the client’s decision to
If therapy was initially declined, most continued coaching and were eventually successful in helping clients accept therapy. In a few cases, there was a delay getting an appointment. Coaches expressed the importance of not abandoning the client during this time, instead continuing coaching support.
Response Theme 3: Coaching Strategies
Participants’
Examples of
Examples of
Whether or not the coach was a physician themselves, all coaches expressed the critical importance of understanding the context in which doctors train, work and live as a key competency in physician coaching. Their description of familiarity with the physician experience included both an understanding of the external landscape of the medical environment, as well as the individual personality, background, and specialty of the physician.
The Decision Bridge
The second segment of each interview invited participants to go beyond describing a specific incident, to comment on how they make decisions about responding to a client’s mental health needs.
As they articulated their legal, ethical, professional and individual position in these areas, coaches revealed details about how they made decisions on a case-by case basis. As they reflected on how they assessed a physician’s level of distress, they used examples to describe their chosen responses.
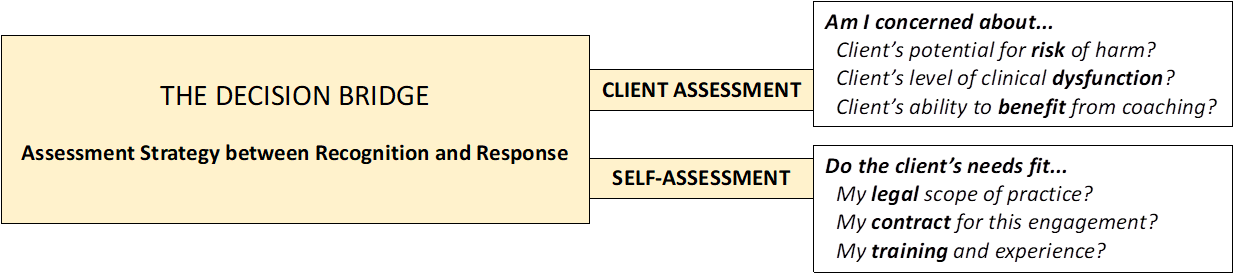
These secondary conversations thereby revealed common patterns of how these coaches moved from recognition to response. This pattern of comments is represented here as a separate theme called the Decision Bridge, shown in Table 3 and described in two sub-themes;
Decision Bridge
Client Assessment: Risk, Dysfunction, and Benefit
In deciding how to respond to distress, participants evaluated the client’s
However, when faced with concerns about a client who seems distressed, coaches must develop a professional opinion about whether the client should be referred to a mental health professional, or if coaching is appropriate. Therefore, this study specifically looked at the process used by coaches to decide how to proceed in these situations. The result then becomes, not a clinical diagnosis about the underlying cause, but the subjective recognition that there may likely be a problem, and a decision about what to do based on that recognition. It is framed by a concern on the part of the coach, not a diagnosis. Therefore, the
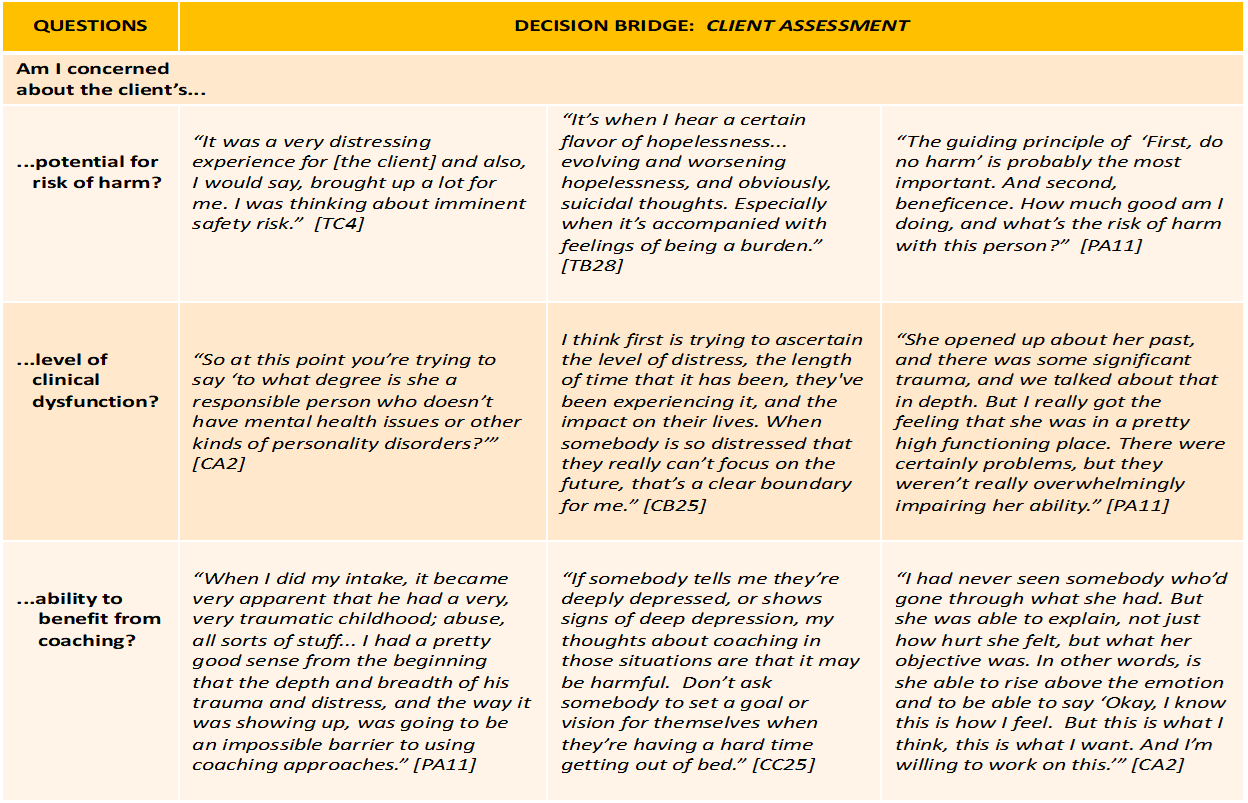
Client Assessment Questions and Quotes in the Decision Bridge Model
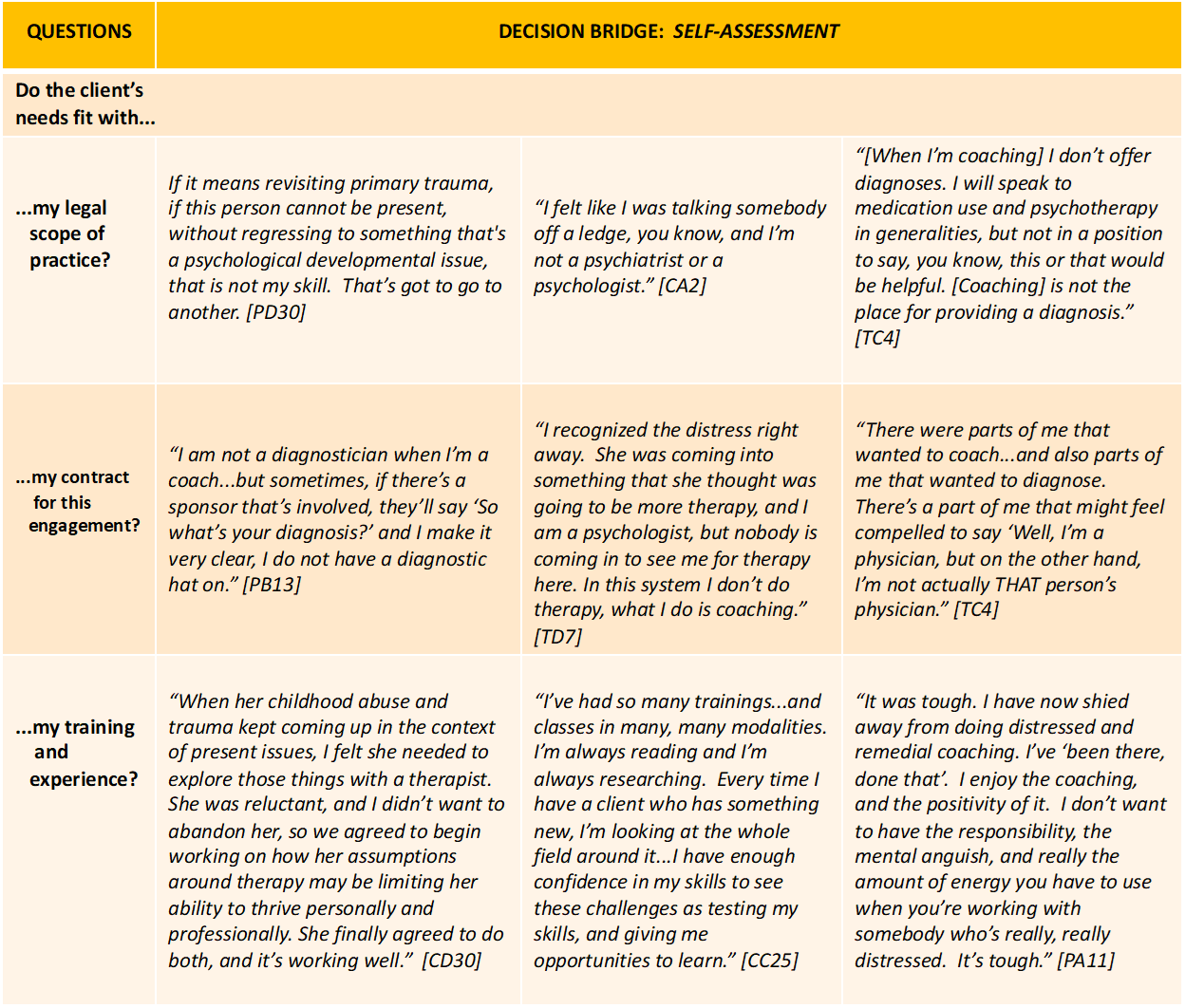
Self-Assessment: Law, Contract, and Training
In this study, coaches described how client needs compared with honest self-assessment of the coach’s
Table 4 provides supporting quotes as examples of
Self-Assessment Questions and Quotes in the Decision Bridge Model
Discussion
This study identified how coaches recognise and respond to mental health needs of distressed physicians, but it also introduced an unexpected theme that emerged as the core variable:
The Decision Bridge Theory
Grounded Theory aims to identify a core variable that could be described to generate and test theory grounded in the data (Simmons, 2010). In the course of coding data and analysing themes from interviews, a common pattern of assessment emerged in these coaches’ decision-making process. This core variable was explored in later data collection. The resulting theme is represented in the form of six paraphrased questions, expressed as a mental model called the Decision Bridge.
Assessment questions are a well-established process for reflection in coaching, and authors have provided excellent questions and guidelines for coaches to consider when evaluating their competencies and the mental health needs of clients (Buckley, 2007; Buckley & Buckley, 2012; Cavanagh & Buckley, 2018). However, no previous publication has described the process that physician coaches are actually using as they make decisions about how to respond. This study explored the questions coaches tend to ask themselves when making decisions, identifying three key questions about the client, and three questions about themselves.
The Decision Bridge is proposed as a mental model that can help coaches reflect systematically on both
Client-Assessment: Risk, Dysfunction, and Benefit
In deciding how to respond to distress, coaches in this study evaluated the client’s
Based on concerns about
Regarding level of
A third question in the Decision Bridge involved the client’s
Self-Assessment: Law, Contract, and Training
Participants assessed their
Fielder and Starr (2008) emphasize the critical role a contract plays in clarifying the
Coaches in this study also asked themselves, do the client’s mental health needs fit my
Kets de Vries (2010) cautions against falling into the Rescuer Syndrome, when a coach’s desire to help goes too far. This can occur because coaching is not guided by the kind of oversight present in licensed professions, potentially “turning helpers into ’rescuers’, unable to differentiate between their own needs and those of their clients.” This could lead coaches to blur boundaries and take their relationship with clients into inappropriate areas.
Self-reflection, training, and supervision can help coaches avoid this pitfall, and the coaching contract itself can serve as a clear reminder of the coach’s scope of practice, even if they have advanced training.
Finally, when coaching does seem to be an appropriate modality in a situation, coaches must consider their personal level of
When a coach recognises a client’s need that goes beyond their training and experience, continuing education and supervision is critical, and the best decision may be to make a referral (Iordanou, Hawley & Iordanou, 2017; Bachkirova, Jackson & Clutterbuck, 2021). In all cases, “coaches who care about their model of coaching practice will be wise to constantly reform, refine, re-examine and rebuild that model.” (Bachkirova, Clutterbuck & Cox, 2018).
As the coaching profession matures, scholars are calling for expanded research in outcomes, effectiveness, and competencies (Boyatzis et al, 2022). Mental health literacy is a critically important competence for coaches, and it is hoped that studies like this will complement the body of information being gathered and shared in that area (Institute of Coaching, 2022).
Conclusion
This study answered the research question “How do experienced coaches recognise and respond to mental health needs of distressed physicians?” Findings demonstrated
The
Implications for this research are twofold: 1) to further the contribution to literature on how experienced coaches make decisions about working with physicians in distress and 2) to offer the Decision Bridge model as a tool that can be generalised and developed for coaching distressed clients in any profession.
Acknowledging the limited sample size of this study, it remains to be seen whether these findings can be generalised to other coaching situations. If these findings do turn out to be widely applicable, the following recommendations are offered to coaching researchers, coaching organizations, and coaches: First, more research is needed in the area of physician coaching, and in the competencies required to work with this population of highly stressed professionals. Second, Mental Health Literacy training should be offered by coaching organizations as continuing development for all coaches, to understand how to recognise and make informed decisions about how to respond to clients’ needs. And finally, individual coaches should take personal responsibility for their own continuing professional development, familiarity with local laws on coaching parameters, and preparation of personal materials for mental health emergencies and therapeutic referrals.
Effective coaching can provide critically needed mental health support for the doctors who care for us all. Coaching research, personal preparation, and continuing professional development are important keys to effectively coaching distressed physicians.