
Abstract
Background
The purpose of this study was to investigate the presentation pattern, sinonasal symptoms, and quality of life (QOL) in patients with Churg-Strauss syndrome (CSS) vasculitis.
Methods
A cross-sectional study was performed. Twenty-five patients with CSS belonging to a patient self-help group participated. Main outcome measures included mode of initial presentation, treatment, rhinologic symptoms, and disease-specific QOL (Sinonasal Outcome Test [SNOT-22] scores) and comparisons were made with general rhinosinusitis and other nasally affected vasculitis patients ((Wegener's granulomatosis [WG]).
Results
Overall, 80% of CSS patients had active sinonasal symptoms at the time of the study. Twenty-eight percent of CSS patients reported worsening of their nasal symptoms as the main event leading to their diagnosis. Forty-eight percent of CSS patients had undergone nasal surgery. Nasal symptoms that are of particular relevance to this patient group are nasal obstruction (95%), rhinorrhea (95%), anosmia (90%), and excessive sneezing (80%). Other symptoms included nasal crusting (75%), purulent nasal discharge (65%), and epistaxis (60%). SNOT-22 scores were significantly higher than normal, reaching average values similar to those of patients from the general rhinosinusitis population.
Conclusion
Sinonasal symptoms are common at initial presentation of CSS, emphasizing the role of otolaryngologists in its diagnosis. Overall, CSS-related sinonasal morbidity is significant and comparable with that of the general rhinosinusitis population. It predominantly results from symptoms of allergic rhinitis, but a significant proportion of CSS patients also report milder forms of crusting, epistaxis, and of purulent sinusitis, symptoms which are more commonly attributed to patients with WG.
Nasal involvement of CSS is well documented, but it is rarely considered by physicians as a significant contributory factor to overall CSS-related morbidity. Neither the impact of sinonasal involvement on the quality of life (QOL) of CSS patients nor the nasal symptom pattern of this disease has been investigated in detail. This study aims to explore this area and further compare the findings to published data for WG, 3 the more common ANCA-associated vasculitis with significant nasal manifestations.
Methods
Ethical approval for this study was obtained from the Royal Free Hospital Medical School Research Ethics Committee, London, U.K. A postal enquiry was performed of 49 CSS patients who were members of the Stuart Strange Vasculitis Trust, a U.K. patient self-help group. This obtained basic information including circumstances leading to patients’ diagnoses of CSS and current treatment regimens.
Our symptom enquiry included a selection of relevant nasal symptoms as part of a rhinosinusitis disease-specific QOL instrument, the Sino-Nasal Outcome Test (SNOT-22). This was the widely used modification of the original SNOT-20 4 and was previously validated in the Royal College of Surgeons of England's National Comparative Audit of Surgery for Nasal Polyposis and Chronic Rhinosinusitis. 5 In addition, we included three additional symptoms that we have previously found relevant to patients with vasculitis 6 : epistaxis, nasal crusting, and nasal deformity. A symptom severity product (SSP) was calculated for each symptom. This was the product of severity scoring for each symptom on a scale from one to five and the percentage of CSS patients reporting the symptom. SSP values were compared with figures for WG patients from our previous study using the two-tailed t-test, Statistica Version 6. Finally, the SNOT-22 score average for the CSS group was compared with the preoperative general chronic rhinosinusitis (CRS) population average published in the National Comparative Audit (n = 2803; average, 42.0; 95% CI = 41.2–42.7) using the student t-test, Statistica Version 6.
Results
Group Demographics and Diagnosis Pattern
Twenty-five patients with CSS responded (51%); 10 (40%) men and 15 (60%) women. Twenty-three were white (92%), 1 was Asian (4%), and 1 was of African origin (4%). The average age at diagnosis was 55.4 years (range, 31.7–79.3 years; SD, 14.5). The average age at the time of the survey was 56.3 years (range, 33–81 years; SD, 14.6). The average reported delay in diagnosis was 18.5 months (range, 1–71 months) from presenting to the physician with worsening of symptoms that eventually led to the diagnosis. Ten (40%) patients reported worsening of their asthma or new pulmonary findings as the most prominent event. A significant proportion of patients (28%) reported that their initial diagnosis was mostly related to worsening of their nasal symptoms. The frequency of predominant presenting symptoms leading to the diagnosis of CSS with respect to the various bodily systems is summarized in Fig. 1
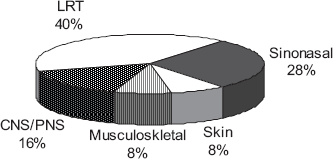
Predominant presenting bodily system in Churg-Straus syndrome patients leading to their diagnosis (n = 25). LRT, lower respiratory tract; CNS, central nervous system; PNS, peripheral nervous system.
Treatment Pattern
Six (24%) and four (16%) CSS patients were on prednisolone and azathioprine monotherapy, respectively. Twelve (48%) patients were taking two immunosuppressants (10 [40%] patients were taking prednisolone/azathioprine, 1 [4%] patient was taking prednisolone/methotrexate, and 1 [4%] patient was taking cyclophosphamide/methotrexate). One patient (4%) was on combination therapy of four different agents and two patients (8%) were on no immunosuppressants. Only eight (32%) of the CSS patients were using topical nasal steroids and none were using saline irrigation. Twelve (48%) CSS patients reported a history of nasal surgery. Seven patients had undergone nasal polypectomy and three patients had had nasal polypectomy with sinus surgery. One patient reported sinus surgery alone and one patient reported sinus surgery with septoplasty and turbinate diathermy. Overall, 40% of CSS patients had undergone nasal polypectomy and 20% had had sinus surgery.
Sinonasal Symptom Pattern and QOL
Active sinonasal symptoms were reported by 80% of CSS patients (20/25). Ninety-five percent (19/20) of these reported nasal obstruction and excessive rhinorrhea. Eighty-five percent (17/20) reported anosmia and 80% (16/20) reported excessive sneezing. As many as 75% of patients (15/20) reported some degree of nasal crusting, 65% (13/20) had purulent nasal discharge, and 60% (12/20) reported each of facial pain, postnasal discharge, and epistaxis to varying degrees. The SSP for each rhinologic symptom in CSS is shown in Fig. 2, with comparative data for patients with WG. The average SNOT-22 score of nasally affected CSS patients (n = 20) was 41.55. This did not differ significantly from that of the general CRS population 5 (SNOT-22 = 42.0; p = 0.68; t-test, Statistica Version 6).
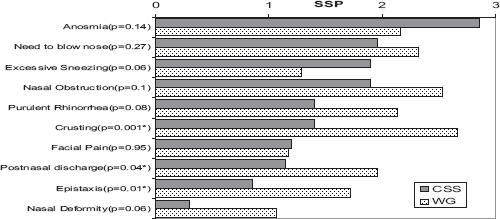
Rhinologic Symptom Severity Product values for Churg-Straus Syndrome (CSS, n = 20) and Wegener's granulomatosis patients (WG, n = 127) with nasally active vasculitis (*statistical significance; two-tailed t-test, Statistica Version 6).
Discussion
With up to 28% of patients presenting with worsening nasal symptoms, it is clear that rhinologists play an important role in the diagnosis of CSS. The significant delay in the diagnosis highlights the need to increase awareness of this condition. Despite this, it is likely that diagnosis will remain difficult in the ear, nose, and throat (ENT) setting, with the relatively common findings of nasal polyps and rhinitis being the main presentations, and negative ANCA testing in many more patients than is encountered in WG. From our experience, a careful enquiry of recent or adult-onset asthma is valuable. It is also worth remembering that although CSS is rare, complex, and with many of its clinical features rather unfamiliar to the ENT surgeon, it can at times present with external clinical signs such as vasculitic cutaneous lesions or CSS-related mononeuritis multiplex, which may include the cranial nerves. Similarly, simple routine clinical investigations can lead to the diagnosis in suspected CRS and polyp patients (Table 1). Once the diagnosis is made, referral to other clinicians opens up a whole new set of therapeutic possibilities, leading to significant improvements in patients’ QOL.
Clinical tests that may aid diagnosis of Churg-Straus syndrome (CSS) in suspected chronic rhinosinusitis/polyp patients
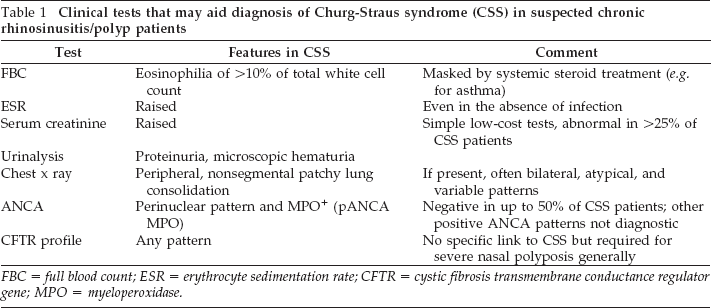
FBC = full blood count; ESR = erythrocyte sedimentation rate; CFTR = cystic fibrosis transmembrane conductance regulator gene; MPO = myeloperoxidase.
This study includes a good number of patients with a rare condition, and our sampling of patients from the community minimizes the selection bias that often affects cohorts from subspecialist units. On the other hand, there is an inherent reliance on patients’ memories and inability to clinically confirm the diagnosis of CSS in each patient. Even if this was possible, pinpointing the diagnosis with certainty remains difficult due to the poor sensitivity of laboratory tests and modest positive predictive values of the continuously evolving criteria for CSS diagnosis.7–9 Each patient from our study group confirmed that the diagnosis of CSS was reached by their hospital specialist, and we believe that patients suffering from such a serious disease belonging to a self-help group are likely to provide as accurate information as any retrospective search of medical notes.
In a retrospective case note review of vasculitis patients in Norfolk, U.K., 10 only 33% of 18 CSS patients were documented to have active nasal disease at the time of the study, and none were documented by their physicians to have had predominantly nasal symptoms at initial presentation. This is a sharp contrast to our patient-reported figures of 80% and 28%, respectively, indicating possible physician underestimation of nasal morbidity in CSS. Our study confirms the mostly rhinitic symptom pattern in CSS but it is somewhat surprising to see that 60–75% also report crusting and troublesome epistaxis, albeit in less severe forms than in WG with which these symptoms have been more commonly associated. The prevalence of nasal crusting in our community-based group of CSS patients is also much higher than a previously reported figure of 14.2% in a clinically selected series from a subspecialist unit. 11
In our experience, nasal polyps in these patients appear to respond to both systemic and topical steroids but this remains somewhat speculative and, to our knowledge, no prospective studies have been performed to investigate this aspect. The significant proportion of patients undergoing nasal surgery is undoubtedly related to the high prevalence of severely recurrent nasal polyps, confirming the important role of surgery in CSS. Polyps in CSS are typically of the histologically benign eosinophilic type, and the main purpose for biopsy in this situation is to exclude other nasal pathology. In fact, nasal biopsies in CSS are even less likely to confirm vasculitis than the modest positive rates seen in WG, and the clinician almost always needs to rely on other criteria outside the ENT region for CSS diagnosis.
We also find that although 80% of CSS patients report active nasal symptoms, only 32% were using topical nasal steroids. This may be a reflection of the modest efficacy of this treatment modality in CSS-related rhinitis leading to patient noncompliance. Alternatively, it could, perhaps, be a result of underprescription by the patients’ own physicians who may hold the general view that nasal symptoms are insignificant in this setting of multisystem disease. If the latter were true, the patients themselves seem to disagree, as evidenced by their high SNOT-22 scores. These scores show that sinonasal morbidity in CSS patients is on a par with that of the general CRS population, which has already been shown to have a similar impact on patients’ QOL to other common chronic conditions such as diabetes mellitus and rheumatoid arthritis. 12
Conclusion
The diagnosis of CSS is challenging and often associated with significant delay. This is especially true in the ENT setting where patients predominantly present with the common symptoms of rhinitis and nasal polyps. The patient-reported prevalence of active nasal symptoms in CSS is higher than previously published figures, and although the symptom pattern is mostly rhinitic, it also includes crusting, epistaxis, and sinusitis to varying degrees. It is also concluded that CSS-related nasal disease impacts significantly on patients’ QOL to a degree that may be underestimated by the physicians who care for them.
Footnotes
Acknowledgments
The authors thank the Stuart Strange Vasculitis Trust, U.K. (![]() ) for allowing access to their members. The Stuart Strange trust was established in 1992 in memory of Stuart Strange, a patient who had started raising money for research into WG but sadly succumbed to the condition. It publishes a newsletter at least twice a year and provides support for patients suffering from the various vasculitides, including CSS. Referring patients to such help groups can help ease the tremendous isolation that is felt when diagnosed with such a rare condition.
) for allowing access to their members. The Stuart Strange trust was established in 1992 in memory of Stuart Strange, a patient who had started raising money for research into WG but sadly succumbed to the condition. It publishes a newsletter at least twice a year and provides support for patients suffering from the various vasculitides, including CSS. Referring patients to such help groups can help ease the tremendous isolation that is felt when diagnosed with such a rare condition.