
Abstract
Background
Endoscopic management of sphenoid sinus disease has great potential for surgical complications. A variety of endoscopic surgical techniques have been described for entering the sphenoid sinus. The utility of these surgical techniques is based on the position of the superior turbinate attachment to the sphenoid face (Parson's ridge). We introduce a novel computerized tomography (CT) grading system for the attachment of the superior turbinate to the sphenoid face. Using this new grading system, we recommend a safer systematic approach for entry into the sphenoid sinus.
Methods
A grading based on the attachment of the superior turbinate to the sphenoid face at the level of the natural sphenoid ostium was developed. A total of 53 patients were enrolled. Types A, B, and C refer to the superior turbinate attachment at the medial, middle, or lateral third of the anterior sphenoid face, respectively, and type D refers to orbital attachment of the superior turbinate. The surgical approach used (superior turbinate intact [STI] or superior turbinate resection [STR]) was recorded and correlated to the type of superior turbinate attachment.
Results
The overall incidence of the various superior turbinate attachments were 40% (41) for type A, 41% (42) for type B, 18% (19) for type C, and 1% (1) for type D. STR was used in 38 sides (44%) and STI was used in 48 sides (56%). Spearman correlation study showed that the closer the superior turbinate attachment was to the orbit the more likely STR was used as the choice of entry into the sphenoid (p < 0.001).
Conclusion
To perform a safe sphenoid entry it is pertinent to evaluate the superior turbinate attachment to the sphenoid face before making a decision on the method of entry.
Keywords
With the introduction of endoscopic sinus surgery in the 1980s, improved definitions and safer surgical approaches to the sphenoid sinus started to emerge. The best choice of approach tends to vary depending on the experience of the surgeon, the presence of ethmoid disease or skull base tumor, or if the sphenoid sinus disease is isolated 8 (Table 1). The sphenoid ostium has consistently been found medial to the superior turbinate attachment on the sphenoid face. This constant landmark has markedly helped the endoscopic sinus surgeon in identifying the sphenoid sinus and not confusing it with a large posterior ethmoid cell. Kim et al. reported that the sphenoid ostium can be found lateral to the superior turbinate attachment in ∼17% of cases in a cadaveric dissection study published in 2001. 7 This finding was challenged by Millar and Orlandi who found the sphenoid ostium medial to the superior turbinate attachment in a 100% of their 47 cadaveric specimens. 9 They concluded that Kim et al. probably fractured and medialized some of the superior turbinates during mucosal stripping before dissection. In our experience we have never come across a single patient with the sphenoid ostium lateral to the superior turbinate attachment. The endoscopic entry to the sphenoid originally described by Stammberger, in his description of the Messerklinger technique, and later modified by many authors, including Bolger and Lanza, was by performing a partial resection of the superior turbinate through the superior meatus. 10 Bolger et al. in 2001 described the “parallelogram” on the sphenoid face when dissecting through the posterior ethmoid: skull base superiorly, orbit lamina papyracea laterally, superior turbinate medially, and the superior turbinate basal lamella inferiorly. 11 They recommended that the point of entry into the sphenoid should be in the inferior medial half of the parallelogram and, preferably, with a gentle curette rather than forceful puncturing. This, they felt, would avoid a sharp instrument from sliding against the orbit and injuring the optic nerve or carotid artery along the lateral sphenoid wall. The main drawback with this method is that it does not take into account for variations of the superior turbinate attachment to the sphenoid face. A lateralized attachment would potentially leave a very small distance between the turbinate attachment and the orbit to allow for safe entry into the sphenoid, i.e., it would significantly narrow the parallelogram. Using the parallelogram method for sphenoid entry in such a situation can result in injury to the vital lateral structures by entering very lateral into the sphenoid sinus. In extreme situations the superior turbinate can attach to the medial orbital wall leaving the sphenoid face completely within the sphenoethmoid recess. In this situation, using the parallelogram (superior turbinate intact [STI]) technique can be extremely dangerous and an alternative approach (superior turbinate resection [STR]) to the sphenoid sinus should be utilized, i.e., gentle resection of a small portion of the inferior part of superior turbinate using a through-cut instrument without disturbing the upper portion. The surgeon would then enter the sphenoethmoid recess, identify the natural sphenoid ostium, and enlarge it in an inferomedial direction to gain entry into the sphenoid sinus. We use the term STI technique when entering the sphenoid sinus from the posterior ethmoid using a parallelogram method and STR technique when entering via the sphenoethmoid recess after resecting the inferior portion of the superior turbinate. Table 1 summarizes different surgical methods of entering the sphenoid sinus, some of which are now of historical interest.
Summary of different surgical approaches to the sphenoid sinus
CSF = cerebral spinal fluid; STI = superior turbinate intact; STR = superior turbinate resection.
Materials and Methods
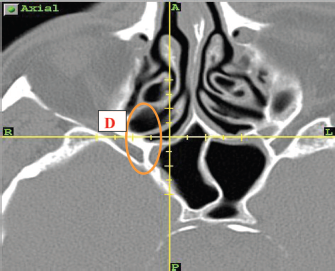
We used a novel computerized tomography (CT) classification system for the sphenoid face. The sphenoid face was divided into thirds in the axial plane at the level of sphenoid natural ostium. The standardized measuring plane was a line drawn on an axial cut at the level of sphenoid natural ostium from the nasal septum to the medial orbital wall laterally. We classified a side as type A if the superior turbinate attached the sphenoid face within the medial one-third, type B if the superior turbinate attached the sphenoid face in its middle one-third, type C if it attached to the lateral one-third, and type D if the superior turbinate attached directly to the orbit (Table 2 and Figs. 1–4).
Classification of superior turbinate attachment to the sphenoid face

Axial computed tomography cut at the level of sphenoid natural ostium showing type A superior turbinate attachment.
Axial computed tomography cut at the level of sphenoid natural ostium showing type B superior turbinate attachment.
Axial computed tomography cut at the level of sphenoid natural ostium showing type C superior turbinate attachment.
Axial computed tomography cut at the level of sphenoid natural ostium showing type D superior turbinate attachment.
After obtaining ethical approval, we analyzed preoperative axial and coronal CT scans of 53 consecutive patients (106 sides) undergoing endoscopic sinus surgery. We excluded all sides that had previous surgery to the sphenoethmoid region.
During surgery the operating surgeon examined the axial and coronal CT and graded the sphenoid face using the sphenoid face grading system described previously. A decision was then made on the method of entry that would be the safest after taking into account the type of sphenoid face and how close the superior turbinate attachment was to the orbit. Correlation was then made between the sphenoid face type and the actual method of entry utilized using Spearman rank order test. Statistical analysis of all data reported in this study was performed using SPSS 16.0 (SPSS, Inc., Chicago, IL).
Results
Fifty-three patients were enrolled in the study. The mean age was 52 years (range, 16 -84 years) with 30 males patients (57%) and 23 (43%) female patients. There were no perioperative complications related to the surgery.
Sphenoid Face and Entry Type
Left Side (Table 3).
All left sides of 53 patients enrolled were eligible for grading because the area of interest had no previous surgery.
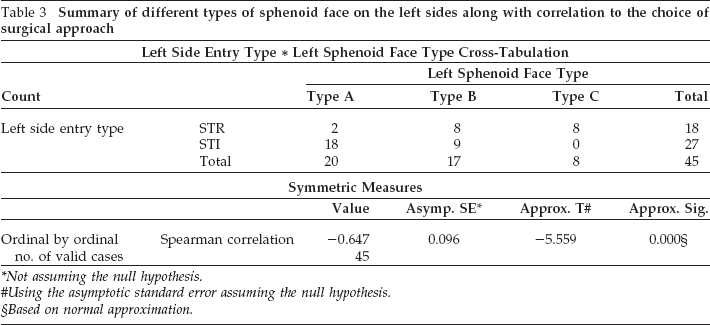
Summary of different types of sphenoid face on the left sides along with correlation to the choice of surgical approach
Not assuming the null hypothesis.
Using the asymptotic standard error assuming the null hypothesis.
Based on normal approximation.
Type A sphenoid face was the most common (22 sides or 41%) followed by type B (21 sides or 40%) and type C (10 sides or 19%). There was no type D found on the left side (0%).
Right Side (Table 4).
Only 50 sides were eligible for the study. Three sides had had previous surgery in the spheno-ethmoid area and were excluded from the analysis. The results were as follows:
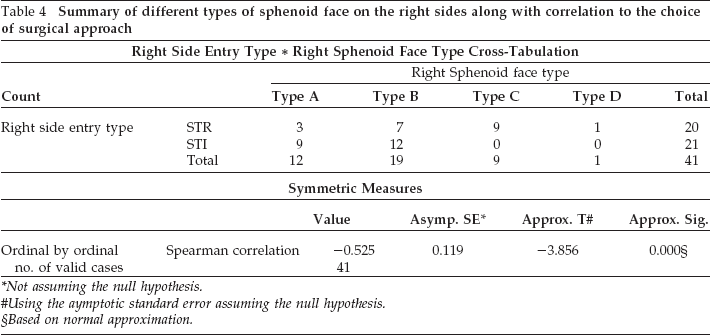
Summary of different types of sphenoid face on the right sides along with correlation to the choice of surgical approach
Not assuming the null hypothesis.
Using the aymptotic standard error assuming the null hypothesis.
Based on normal approximation.
Type A: 19 sides (38%)
Type B: 21 sides (42%)
Type C: 9 sides (18%)
Type D: 1 side (2%)
Overall Incidence
The overall incidences of each superior turbinate attachment type for all sides put together were 40% (41) for type A, 41% (42) for type B, 18% (19) for type C, and 1% (1) for type D.
Entry Type
Left Side (Fig. 5).
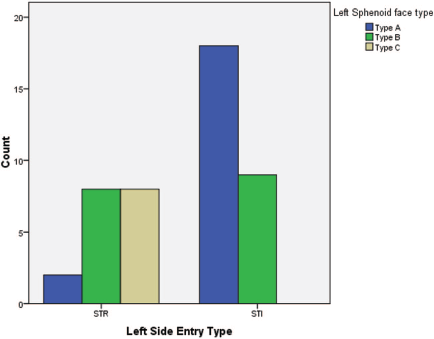
Bar chart comparing number of each superior turbinate attachment type versus type of entry on the left sides.
Entry into the sphenoid on the left side was required in 45 (85%) patients. The decision for entry was strictly clinical. The type of entry (STI versus STR) was determined by the surgeon based on the anatomy of the area. STI technique was the most common and was used in 27 patients (60%) and STR was used in 18 patients (40%).
Right Side (Fig. 6).
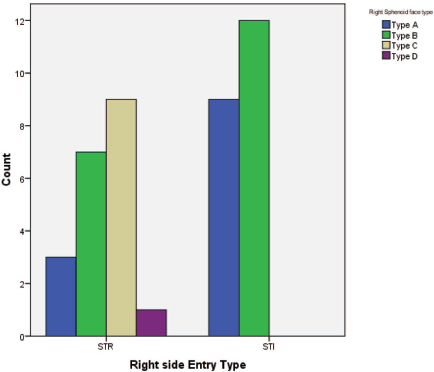
Bar chart comparing number of each superior turbinate attachment type versus type of entry on the right sides.
Entry into the sphenoid sinus on the right side was required in 41 patients (77%). Twenty-one patients (51%) required the STI technique and twenty patients (49%) required the STR technique.
Overall.
STR as a surgical approach to the sphenoid was used 44% (38 patients) of the time while the STI approach was used 56% (48 patients) of the time.
Association between Sphenoid Type and Entry Method
Using the Spearman test, a statistically significant correlation was found between the sphenoid face type and the choice of entry into the sphenoid on both sides, i.e., the closer the sphenoid ostium to the orbit, the more likelihood of choosing the STR method of entry. A value of p < 0.001 was noted on both sides (see Tables 2 and 3 and Figs. 4 and 5).
Discussion
Since the introduction of the Messerklinger technique in the 1980s 12 our understanding of the paranasal sinus anatomy and physiology has improved dramatically. This has been possible because of advancements in sinus surgical instrumentation, endoscope technology, image guidance, and increasing surgical experience. Transecting part of the superior turbinate to access the sphenoid sinus was part of the original description of the Messerklinger technique. Both Min et al. as well as Metson et al. described complete amputation of the superior turbinate during the endoscopic approach to the sphenoid sinus to improve visualization and access.13,14 We feel that this is unnecessary and that every effort should be made to preserve both the middle and the superior turbinates when treating benign chronic sinus disease. Interfering with the vertical attachment of the superior turbinate to the skull base can risk olfaction as well as increase the risk of creating a cerebral spinal fluid leak. 15 The olfactory neuroepithelium is concentrated in the medial and superior part of the superior turbinate and trauma to the area adds to the risk of stripping and damaging this specialized mucosal covering. We feel that it is safer to use through-cutting instruments to remove a small portion of the inferior vertical superior turbinate in a type C or D attachments for entry into the sphenoid sinus via the natural ostium.
It is also important to consider the angle of attachment of the superior turbinate to the sphenoid face. An acute angle may result in a type A attachment superiorly and a type C attachment inferiorly on the sphenoid face. This is appreciated better on a coronal cut along the sphenoid face and can further aide in determining the proper technique of entry into the sphenoid sinus. Additional studies should be conducted on the prevalence and types of superior turbinate angulations. We strongly recommend that the surgeon correlate the axial and coronal CT cuts along the sphenoid face to determine the type and angle of attachment so that a safe decision can be made for entry into the sphenoid. A type C or D superior turbinate attachment should almost always favor an STR technique.
The principal objective of our study was to highlight the fact that a safe sphenoid entry method requires a careful assessment of the superior turbinate attachment to the sphenoid face on CT. We also wanted to introduce a novel grading system to allow for standardized terminology and technique. In the future, additional studies should be conducted, including testing for inter- and intraobserver variability to validate our grading system.
Conclusion
Careful assessment of preoperative axial and coronal CT scanning is essential for safe sphenoid entry. We recommend that the operating surgeon be aware of the type of superior turbinate attachment to the sphenoid face and the angle of the attachment before making a decision on the technique (STI versus STR) for entering the sphenoid sinus.