
Abstract
Background
Postoperative irrigation after endoscopic sinus surgery and endoscopic modified Lothrop procedure is used to remove nasal crusts and to improve wound healing. To evaluate the optimal application protocol for irrigation of the frontal sinus, a prospective cadaver study was performed.
Methods
An endoscopic modified Lothrop procedure and complete sphenoethmoidectomy were performed in 19 heads. Each was irrigated with a 1.5% solution of water and different colors using nasal spray and a squeeze bottle filled with 50, 100, and 200 mL. Intensity of local staining and percentage of area were documented using standardized videoendoscopy after irrigation in “bending over the sink” or “vertex to floor” position. Grading was performed by two independent observers for 23 anatomic regions, including the stained circumference of maxillary and frontal ostia. To evaluate the influence of the anatomy, acoustic rhinometry was performed. ANOVA was used to evaluate effects of application methods and head positions using GenStat 8.2 (Lawes Agricultural Trust, Rothamsted Experimental Station, Harpenden, U.K.) using an appropriate block structure.
Results
With regard to the frontal sinus, we were able to show clear superiority of the squeeze bottle technique filled with 200 mL and applied in the “vertex to floor position.”
Conclusion
In a relatively fit and flexible patient the vertex to floor position using a squeeze bottle technique is advocated. There may be some patients, however, for whom this position is not feasible. In these patients “bending over the sink,” while inferior to the “vertex to floor” position, still ensures some irrigation of the frontal sinus.
Keywords
Endoscopic sinus surgery (ESS) is the accepted treatment of choice for chronic rhinosinusitis, which has failed maximal medical therapy. 5 After surgery, wide areas of bony surface without mucosal lining may be left for healing by secondary intention. Common problems resulting from this management are excessive granulation tissue and adhesion formation, the latter being observed in 17-20% of patients.5,6 These problems are most pronounced in the frontal recess as neo-ostia and tend to cicatrize because of scarring and granulation tissue. Recent publications have proved that conventional nasal spray fails to deliver topical medications reliably to the frontal recess.3,7
Surgical management of recalcitrant frontal sinusitis using the endoscopic modified Lothrop procedure has become increasingly popular. Previous studies have indicated a narrowing of the frontal neo-ostium by at least 25% in the first 12 months after surgery 8 and 80% of revision Lothrop procedures are caused by restenosis. To decrease the acute infection, 9 diminish local biofilms, 10 and thereby possibly improve outcome, an effective topical treatment is desirable. We hypothesized an improved irrigation using the squeeze bottle in comparison with the widely used nasal spray with an additional benefit resulting from a change of head position from bending over a sink to the vertex to floor position. In the “bending over sink” position the head is held 15-30° up from the horizontal plane (Fig. 1), whereas in the vertex to floor position, the vertex is held parallel to the floor with the head axis being 90° tilted to the horizontal plane (Fig. 2). The aim of this study was to evaluate four different application methods of topical aqueous solution at two head positions to determine the most effective method of nasal irrigation. Additionally, we wished to establish a reliable and valid way to analyze intensity and distribution of aqueous solution while avoiding the use of radionuclear techniques for future studies.

Bending over the sink position.

Vertex to floor position.
Materials and Methods
The paranasal sinuses of 19 cadaver heads were evaluated using standard computer tomography in the coronal plane with axial and sagittal reconstructions. An endoscopic modified Lothrop procedure and complete sphenoethmoidectomy were performed as described previously using powered in-strumentation.5 Afterward, heads were irrigated with a 1.5% solution of water and different colors (methylene blue, fluorescein, and food colors). A pilot study assured that staining with multiple colors was possible without interference of measurements.
In each head, a nasal spray (2 puffs; FESS Spray; FESS, Bondi Junction, Australia) and the squeeze bottle (Flo sinus care; ENT Technologies, Malvern, Australia) filled with 50, 100, and 200 mL were used. The angle between the opening of the nasal spray or the douche container and the nasal septum was ∼30-45° to the lateral side. Head positions evaluated were “bending over the sink” (head tilted 30° nose down; cf. Fig. 1) and “vertex to floor” position (Fig. 2). 3 To standardize the pressure applied to the nasal douche, the observer evaluated the maximal tolerable applied pressure for nasal douching of his nose. Afterward, the same pressure was used for irrigation of the cadaver head by the same observer (A.B.) in all cadaver heads with intermittent calibration of pressure when deemed necessary.
Staining was documented using standardized videoendoscopy11,12 with intensity of local staining and percentage of area stained graded by two independent, blinded observers. Gradings from both observers were evaluated to assess inter-observer reliability. Analogous to previous studies, staining was assessed using a staining index with two components; one with a 5-point graduated scale for color intensity (0-4; Table 1) and the other for the percentage area covered with blue color13–15 for 23 different anatomic regions on each nasal side, including the stained circumference of maxillary and frontal ostia.
Classification of staining and its verbal description
To evaluate the influence of the anatomy of the nasal cavity, C and I notch and volume of each nasal side were measured using acoustic rhinometry. Additionally, size and configuration of the middle turbinate, 16 as well as occurrence and localization of a septal deviation, were documented.
Acoustic rhinometry has previously been used to gain objective information about the size and configuration of the nasal cavity. 17 To determine if size of the nasal cavity influences staining, we used this method bilaterally measuring the cross-sectional area.
Statistics
Data were analyzed for normal distribution using the Kolmolgorov-Smirnov test. Intraobserver reliability was evaluated using intraclass correlation coefficient of absolute agreement. Two-way ANOVA was performed to evaluate effects of application methods and head positions using Genstats 8.2 (Lawes Agricultural Trust, Rothamsted Experimental Station, Harpenden, U.K.) with a level of significance of p < 0.05 (β = 20%). A specified block structure was used to account for pairing due to values obtained in the same cadaver on both sides. Intensity of staining and area stained (in percent) were analyzed. Analysis of residuals assured the use of an appropriate model.
Results were correlated with the parameter obtained by acoustic rhinometry, the diameter of the ostia, size of middle turbinate, and occurrence of septal deviation. Power analysis based on the pilot study, as well as previous reports,7,18 suggested a total of eight heads per treatment to show a benefit of at least 20% for the nasal douche. To obtain results under different anatomic conditions, we evaluated 10 heads.
Results
Area of Staining
Mean values for percentage of staining and stained circumference are illustrated with their respective standard error of the mean in Fig. 3, a-d, for different anatomic areas. ANOVA for stained area of the lamina papyracea revealed a significant difference between application methods (p < 0.001) and head positions (p < 0.006) with a significant interaction (p < 0.01). At the skull base, application methods resulted in a significant difference of area stained (p < 0.001), as did head position (p < 0.001), but no significant interaction was observed. The frontal sinus, the maxillary sinus, sphenoid sinus, and ethmoid sinus were also stained significantly differently according to the application method (p < 0.001) and the head position (p < 0.001). Again, a significant interaction of both factors was also observed (p < 0.001).
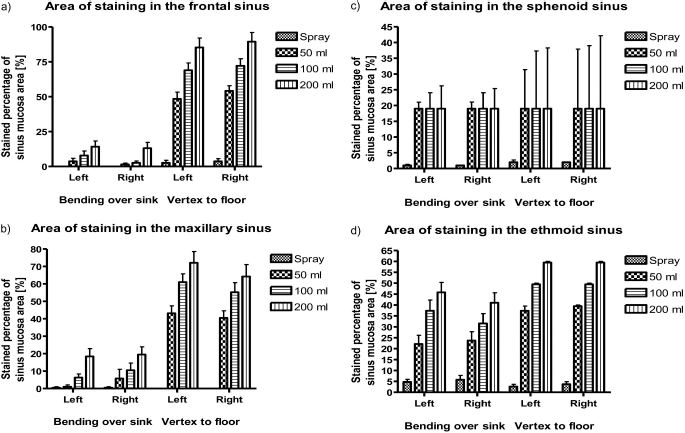
Mean ± standard error of the mean for the percentage of stained area of the (a) frontal sinus, (b) maxillary sinus, (c) sphenoid sinus, and (d) ethmoid sinus for each application method (nasal spray, squeeze bottle filled with 50, 100, or 200 mL, respectively) and both bending over the sink and vertex to floor positions.
Generally, percentage area stained was greater with the squeeze bottle than the nasal spray. Staining increased further with increased filling of the squeeze bottle and if applied in the vertex to floor position. Filling the squeeze bottle with 200 mL is sufficient for staining of the frontal cavity, ethmoid and maxillary sinus; however, the sphenoid sinus only shows a mean surface area of 20% staining using this regimen. Similarly, good results were obtained for staining of the lamina papyracea and the olfactory region (Table 2).
Percentage values of stained surface in relation to total surface of an anatomic region are given for the four treatment modalities (nasal spray, squeeze bottle with 50/100/200 mL)

Analysis of ostial circumference allowed comparisons to be made with regard to treatment of these regions. The frontal neo-ostium and maxillary ostia circumference showed significantly different staining both for application methods (p < 0.001) and head position (p < 0.001; Tables 3 and 4). The interaction of both factors was also significant (p < 0.001), indicating that the relative additional benefit of douching in the vertex to floor position decreases with increased filling of the squeeze bottle. Using the best combination of application methods and head position, 355.3° (98.7%) of the frontal neo-ostium circumference (postmodified Lothrop) was stained by the irrigating solution.
Staining of ostium circumference

Values of stained ostial circumference are given for the four treatment modalities (nasal spray, squeeze bottle with 50/100/200 mL) irrespective of the position used (pooled data).
Effect of head position on ostial circumference staining
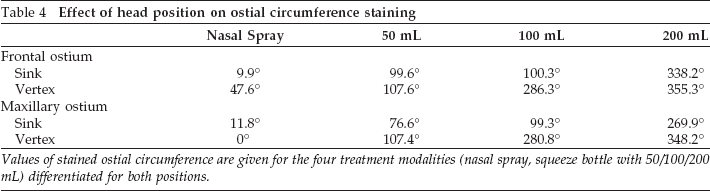
Values of stained ostial circumference are given for the four treatment modalities (nasal spray, squeeze bottle with 50/100/200 mL) differentiated for both positions.
Analysis of Staining Intensity
Analysis of staining intensity supported the general findings reported previously. Application methods resulted in significantly different staining intensity (p < 0.001) for lamina papyracea; olfactory region; and the frontal, maxillary, ethmoid, and sphenoid sinuses with much less variation of values due to the 5-step scale used.
Head position showed a significant effect for lamina papyracea staining intensity (p < 0.007) in favor of the bending over the sink position (Table 5). In contrast, the vertex to floor position resulted in significantly more intense staining of the frontal, maxillary, ethmoid, and sphenoid sinuses (p < 0.001). For the olfactory region, staining intensity was not significantly different between the two head positions. In short, the additional tilting of ∼105-120° forward from bending over the sink to vertex to floor position changes endonasal flow away from the lamina papyracea toward and into the frontal, ethmoid, and maxillary sinus.
Intensity of staining
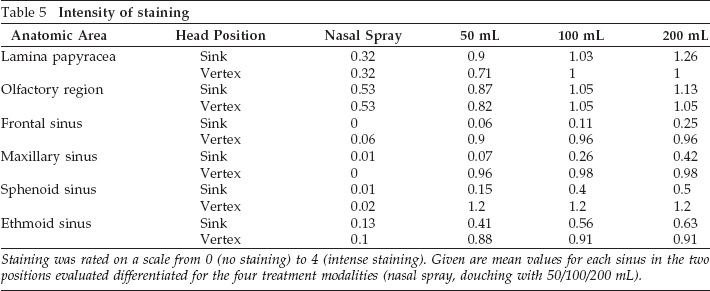
Staining was rated on a scale from 0 (no staining) to 4 (intense staining). Given are mean values for each sinus in the two positions evaluated differentiated for the four treatment modalities (nasal spray, douching with 50/100/200 mL).
A significant interaction of head position and application method was observed for the frontal, maxillary, ethmoid, and sphenoid sinuses (p < 0.001), again indicating that the relative additional benefit of douching in the vertex to floor position decreases with increased filling of the squeeze bottle. This interaction indicates that patients, who are unable to use the squeeze bottle in a vertex to floor position due to other co-morbidities) should use a 200-mL squeeze bottle to achieve the next best possible effect.
Significant nonparametric correlation occurred between septum classification and frontal sinus staining (p < 0.05) independent of application method, indicating a persisting effect of anatomy of the septum on sinus irrigation. No effect of nasal geometry, measured by acoustic rhinometry (C or I notch, volume of nasal cavity) on area of staining was observed. Intraclass correlation coefficient for interobserver reliability showed good agreement for classification of area (0.92) and intensity (0.95) staining.
Discussion
This study shows a significant improvement in both surface area stained as well as intensity of staining for the maxillary, ethmoid, and frontal ostia and sinuses as well as the olfactory groove and lamina papyracea with the use of a squeeze bottle filled to its maximum volume after an endoscopic modified Lothrop procedure with complete sphenoethmoidectomy. Additionally, this study shows that the head position of vertex to floor is superior in irrigating the frontal, maxillary, and ethmoid sinus in comparison with bending over the sink. In contrast, the olfactory groove was stained significantly better in a bending over the sink position. These effects were independent of variations in endonasal geometry. For postoperative treatment, vertex to floor position with a 200-mL squeeze bottle seems to be the best irrigation protocol, and the squeeze bottle in a bending over the sink position will reliably deliver topical medication to the olfactory grove.
Postoperative management regimens of patients who have undergone ESS for chronic sinusitis frequently include topical saline washes, and steroid nasal sprays and these treatments have been shown to improve outcomes.19–21 This may be partially due to the delivery of topical medications, removal of debris, and reduction in adhesion formation. Additionally, douching can be used as a route of drug delivery. This has the theoretical advantage of allowing the use of much higher concentrations of the active agents because of reduced systemic absorption of many pharmaceuticals, similar to that seen in the external auditory canal.10,22 Because of the recent biofilm theory in the etiology of chronic sinusitis22,23 reliable methods of applying highly concentrated, topical medication in the paranasal sinuses are of increasing importance. Furthermore, contradicting results of studies using topical medications to treat fungal sinusitis24,25 may in part be due to different application modes used in the studies.
According to various authors,6,26 mucosal regeneration is crucial for success of surgery. Key areas include the osteomeatal complex particularly between the middle turbinate and the maxillary ostium as well as the frontal recess. Using nasal sprays, only a small part of the medication is applied to the middle meatus. 27 Consequently, application to the middle meatus under endoscopic vision has been recommended. This would be associated with increased direct and indirect treatment costs in the postoperative care as well as potential mild patient discomfort. Improved application of topical medication after ESS could thus improve outcomes and reduce the prevalence of recurrent sinusitis.
To our knowledge, this study is the second to use cadaver heads with a simulated operation to evaluate multiple application methods and head positions and their impact on the extent and intensity of local irrigation. Parallel and independently, St. Martin et al. 28 showed only 20% of penetration into the maxillary sinus using a nebulizer system. Despite the obvious difference in methodology, our results indicate a treatment of 60-70% surface area of this sinus using a squeeze bottle in vertex to floor position.
With regard to the frontal sinus, we were able to show clear superiority of the squeeze bottle filled with 200 mL and applied in the vertex to floor position. However, if the elderly patient is unable to perform the vertex to floor position, bending forward over a sink will still ensure irrigation of the frontal sinus. Therefore, we regard this application method as being able to reliably deliver a topical, aqueous medication to the frontal sinus and the newly created ostium to improve wound healing and possibly reduce postoperative restenosis. The squeeze bottle can therefore be regarded as an ideal technique for irrigation of the sinonasal cavity after ESS.
Naturally, there are limitations to this particular squeeze bottle technique as well as to the vertex to floor position. Not all patients are able to tolerate significant volumes of saline solution irrigating their sinonasal cavities because it may cause them some discomfort. Additionally, as mentioned previously, the elderly or arthritic patient who is less flexible will have difficulty in bending completely over in the vertex to floor position as shown in Fig. 2. This may also present some difficulties for patients who are prone to syncope and we recommend that the appropriate advice is given to these patients before education on the technique.
Patients who have undergone complete sphenoethmoidectomies and a modified Lothrop procedure will have large exposed areas of raw bone that result in extensive crusting. Thus, appropriate saline douching of the sinuses is vitally important to reduce this crusting and improve postoperative healing. Some may criticize the use of cadaver specimens to evaluate nasal penetration of the various douching methods. Although the nasal and sinus mucosa of the cadaver head are maximally decongested, this should facilitate penetration of endonasal fluids by either sprays or douches, allowing comparison of the techniques. In addition, the results of this cadaver study can only be applied to postoperative irrigation of sinuses and not to patients who have not undergone surgery. Our results indicated a persistent effect of septal anatomy on the irrigation of the frontal sinus (shown, e.g., bythe side differences in Fig. 1, a-d). This strong correlation seen between septal anatomy and frontal sinus irrigation identifies the role of septal deflection in obtaining maximal sinus penetration of douches in the postoperative period. 27
We have previously reported a transient improvement in ciliary beat frequency by sodium chloride application using spray bottles. 18 Taking our current results into consideration, a more pronounced effect might be possible using the squeeze bottle because of the more extensive coverage of sinus epithelium during irrigation.
Conclusion
The squeeze bottle is a reliable method for irrigating the frontal neo-ostium and sinuses after endoscopic Lothrop procedure and complete sphenoethmoidectomy. Filling the bottle with 200 mL increases the irrigation of the frontal sinuses and other sinuses, with exception of the sphenoid, as does use of the vertex to floor position.