
Abstract
Background
Invasive fungal sinusitis is a progressive disease that can often extend beyond the nasal cavities and paranasal sinuses into surrounding soft tissue and bone. Aggressive antifungal therapy and surgical debridement are the mainstays of management. The pterygopalatine fossa and infratemporal fossa are two regions that are commonly involved in patients with invasive fungal sinusitis. When fungal disease extends to the infratemporal fossa, surgical debridement can be challenging. Traditionally, open approaches have been used for the management of disease in these areas. Advances in endoscopic skull base surgery may allow for less invasive approaches for the management of disease in the infratemporal fossa. This article describes a transnasal endoscopic approach to the infratemporal fossa for debridement of invasive fungal sinusitis.
Methods
Patients with invasive fungal sinusitis extending into the infratemporal fossa were treated with endoscopic debridement. Records of these patients were reviewed.
Results
Endoscopic debridement was performed in four patients with infratemporal fossa extension of invasive fungal sinusitis. Responsible organisms included Aspergillus, Mucor, and Candida. Adequate access and excellent visualization of the infratemporal fossa were obtained in all patients. The endoscopic anatomy and surgical technique are presented.
Conclusion
Endoscopic approaches have been used to manage a variety of disease processes that extend beyond the confines of the paranasal sinuses. Invasive fungal sinusitis disease with extension into the infratemporal fossa can be safely debrided via a transnasal endoscopic technique. The approach provides excellent visualization with low morbidity.
Keywords
Spread of fungus beyond the walls of the maxillary sinus into the preantral and retroantral fat pads is a well-described pattern of fungal invasion. This pattern of spread can occur in the absence of frank bony erosion via communicating vessels. 2 Once the retroantral fat pad has been infiltrated, fungus can then spread throughout the pterygopalatine and infratemporal fossae (Fig. 1). Surgical access to these regions can be difficult and has traditionally been achieved using a variety of open approaches. 3 This report details a transnasal endoscopic approach to the infratemporal fossa used in four patients with invasive fungal sinusitis. The endoscopic approach provides excellent visualization and access while decreasing the potential morbidity in comparison with open surgical approaches.

Preoperative axial computerized tomography image showing left maxillary sinus opacification and obliteration of the retroantral fat plane (black arrowhead) and extension of disease into the pterygopalatine and infratemporal fossae. The normal retroantral fat plane is shown on the right (white arrow).
Materials and Methods
Records of patients who underwent endoscopic debridement of invasive fungal sinusitis in the infratemporal fossa were reviewed.
Surgical Technique
The pterygopalatine fossa is a pyramidal-shaped space posterior to the maxillary sinus and anterior to the pterygoid plates. It is contiguous with the infratemporal fossa laterally via the pterygomaxillary fissure (Fig. 2). The lateral limit of the infratemporal fossa is the mandibular ramus. Exposure of the infratemporal fossa is facilitated by first obtaining exposure of the pterygopalatine fossa medially. Our preferred approach for entry into the pterygopalatine fossa is through the sphe-nopalatine foramen.

The pterygomaxillary fissure (arrow) allows communication between the pterygopalatine fossae medially and the infratemporal fossa laterally.
The procedure begins with a standard endoscopic middle meatal approach to the maxillary sinus. To allow complete removal of disease within the maxillary sinus, a wide antrostomy is made, requiring removal of the majority of the medial maxillary sinus wall. Partial resection of the inferior turbinate may also be indicated to improve visualization of the entirety of the posterior maxillary sinus wall.
The sphenopalatine foramen is then localized by identifying the sphenopalatine artery. Elevation of a mucosal flap along the nasal surface of the perpendicular plate of the palatine bone reveals the sphenopalatine artery, exiting the foramen just posterior to the crista ethmoidalis. 4 A Kerrison rongeur is then placed in the space between the anterior wall of the foramen and the artery itself, and bone removal of the posterior maxillary sinus wall is performed laterally. Alternatively, a drill can be used to remove the bony posterior maxillary sinus wall to access the pterygopalatine fossa without entry through the sphenopalatine foramen.
The internal maxillary artery can be identified within the pterygopalatine fossa, and electrocautery or clips can be used to control the vessel. In our experience, the artery is frequently thrombosed in patients with invasive fungal sinusitis and may not need to be controlled. It is usually not possible to identify individual neural elements within the pterygopalatine fossa because of the extensive necrosis that is frequently seen in patients with invasive fungal sinusitis. In patients without sensory deficits and limited pterygopalatine fossa disease, injury to the maxillary division of the trigeminal nerve can be avoided by keeping the dissection inferior to the level of the sphenopalatine foramen. 5 Debridement of the contents of the pterygopalatine fossa is then performed using a combination of the microdebrider and cutting forceps. Debridement can proceed aggressively in areas that are obviously necrotic.
The pterygoid process forms the posterior extent of the pterygopalatine fossa, and dissection laterally from the pterygoid process exposes the lateral pterygoid plate and the origin of the lateral pterygoid muscle (Fig. 3). This is the medial extent of the infratemporal fossa. Removal of the posterior maxillary sinus wall is continued further laterally using Kerrison rongeurs, curettes, or a drill. This allows exposure of the infratemporal fossa. Preoperative imaging will often determine the amount of lateral exposure needed.
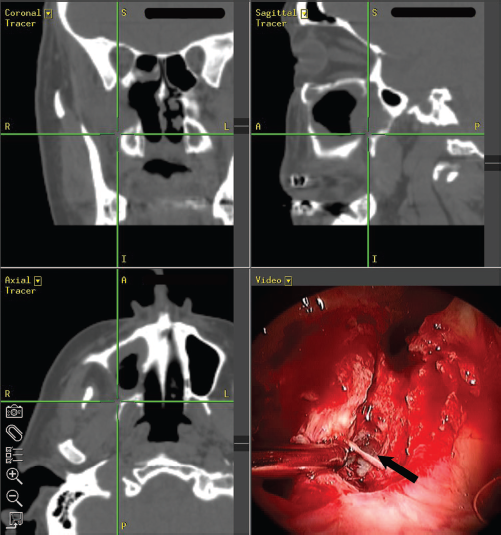
Intraoperative computerized navigation image shows entry into the right infratemporal fossa. Suction tip points to posterior maxillary sinus wall. The origin of the lateral pterygoid muscle from the lateral pterygoid plate is shown (black arrow).
When access to the lateral extent of the infratemporal fossa is required, it is often possible to remove the majority of the posterior wall of the maxillary sinus with curved instruments and angled endoscopes (Fig. 4). Although it was not necessary in the cases presented here, lateral exposure can be augmented by performing a Caldwell-Luc approach to facilitate the placement of instruments at the far lateral extent of the maxillary sinus.

Axial computerized tomography image showing that the majority of the posterior wall of the maxillary sinus has been removed, allowing access to the lateral extent of the infratemporal fossa (arrow).
The use of computerized navigation can be helpful in guiding the dissection. More recent advances in intraoperative navigation have allowed computerized tomography (CT) and magnetic resonance imaging (MRI) to be used simultaneously for navigation. This combination can be helpful in determining the extent of surgical debridement required. After CT-based navigation is used to direct bone removal, the MR-based navigation can guide the extent of surgical debridement performed within the soft tissue regions.
Results
Four patients with infratemporal fossa extension of invasive fungal sinusitis underwent endoscopic debridement (Table 1). Presenting symptoms included cheek swelling, headache, diplopia, and facial numbness. All patients were immunocompromised from at least one underlying comorbid disease. Patient age ranged from 51 to 70 years (mean, 63 years). Follow-up time ranged from 12 to 445 days (mean, 144 days).
Patient data
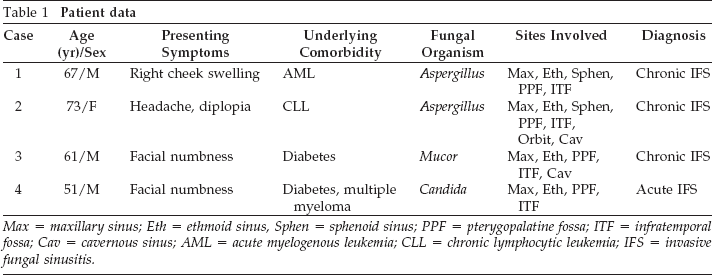
Max = maxillary sinus; Eth = ethmoid sinus, Sphen = sphenoid sinus; PPF = pterygopalatine fossa; ITF = infratemporal fossa; Cav = cavernous sinus; AML = acute myelogenous leukemia; CLL = chronic lymphocytic leukemia; IFS = invasive fungal sinusitis.
In all patients, all extracranial foci of disease were accessible using the transnasal endoscopic approach. Wide exposure was obtained of the infratemporal fossa in all patients, allowing wide debridement of disease in this area. Multiple debridements were necessary in most patients (range, 1-6 debridements; mean, 3.75). All procedures were performed with computer-guided navigation. All of the patients tolerated the procedures well, and there were no intraoperative complications.
Patient 1 was alive and disease free 6 months after his most recent endoscopic debridement. Patients 2 and 3 developed intracranial extension of their disease after management of the sinonasal and other extracranial sites of disease. The extent of intracranial extension in these patients precluded further surgical management. At the time of last follow-up, patient 2 continued to be on systemic antifungals for the persistent intracranial foci of disease; patient 3 has been lost to follow-up. Patient 4 died with disease after being placed on comfort care because of deterioration of overall health caused by graft versus host disease. None of the patients had evidence of residual disease in the infratemporal fossa at the time of last follow-up.
Discussion
Invasive fungal sinusitis can follow an aggressive course and often extends beyond the paranasal sinuses. Three forms of the disease have been described based on differences in the clinical course and histological appearance. These include acute fulminant invasive fungal sinusitis, chronic granulomatous invasive fungal sinusitis, and chronic nongranulomatous invasive fungal sinusitis. 6 The latter two progress over a longer time period than the acute invasive form, but all three forms can be associated with extensive disease and an aggressive course. In addition, the chronic forms can often be seen in immunocompetent patients. The clinical importance of distinguishing between the granulomatous and nongranulomatous forms is unclear, with authors describing similar prognosis and treatment for both forms. 7
When invasive fungal disease involves the infratemporal fossa, surgical exposure can be difficult. Traditional open techniques using a variety of anterior and lateral skull base approaches have been used effectively to manage infratem-poral fossa lesions. 3 These approaches provide adequate visualization of the contents of the infratemporal fossa but require lengthy surgical procedures and can be associated with significant morbidity. External lateral approaches involve dissection of the facial nerve and internal carotid artery, placing these structures at risk. In addition, the mandibular manipulation necessary with lateral approaches may lead to sequelae of trismus and malocclusion. External anterior approaches to the infratemporal fossa require extensive soft tissue dissection and osteotomies.
Advances in endoscopic equipment and techniques have allowed surgeons to apply endoscopic techniques to the management of pathology extending beyond the paranasal sinuses. In recent years, there have been several reports of endoscopic approaches to the pterygopalatine fossa.5,8,9 The pterygopalatine fossa communicates laterally with the infra-temporal fossa, but reports of endoscopic infratemporal fossa surgery have been much more limited. 10 These reports have centered on resection of juvenile nasopharyngeal angiofibromas with infratemporal fossa extension. 11
Only Robinson et al. provided a detailed description of the surgical technique used. 10 These authors used a two-surgeon approach for endoscopic resection of benign tumors of the infratemporal fossa. The approach included an incision through the septum to allow insertion of instruments from the contralateral nasal cavity. The second surgeon could then apply traction to the tumors using this septal incision. Our experience extends the indications for endoscopic approaches to the infratemporal fossa and illustrates that even the most lateral areas of this region can be reached with a transnasal endoscopic approach. In addition, a single-surgeon approach without septal incisions was adequate in all of the cases presented. It appears that resection of tumors requiring traction benefit from a transseptal approach, 10 whereas resection of lesions such as invasive fungal sinusitis can be approached without the septal dissection.
The endoscopic approach to the infratemporal fossa provides several advantages compared with alternative techniques. First, excellent visualization is afforded by the illuminated, magnified optics. Second, decreased morbidity may result from limiting dissection of uninvolved areas, avoiding external incisions, and eliminating the need for osteotomies.
Endoscopic approaches also greatly facilitate ongoing surveillance with office or bedside endoscopy and make it possible to perform repeat debridements with relative ease. Multiple debridements are frequently required in patients with invasive fungal sinusitis, and external approaches to the infratemporal fossa would make repeat debridements of this region more difficult.
Exposure as far laterally as the mandible was achieved using the surgical technique described. It is important to have available a variety of curved instruments and angled endo-scopes to access lateral disease. In addition to angled forceps, curved microdebrider blades were found to be very useful in performing debridement of the lateral areas. It is also important to collect specimens using a trap to have adequate amounts of tissue for culture and histological analysis.
The internal maxillary artery and its branches course throughout both the pterygopalatine and the infratemporal fossae. Controlling these vascular structures can prove to be challenging with endoscopic approaches. Vascular control is best attained using cautery or vascular clips. A variety of endoscopic bipolar forceps are now available, facilitating selective control of vascular structures in these areas. In patients with invasive fungal sinusitis, disease progression can lead to vascular thrombosis and may eliminate the need for formal control of these vessels. This was found to be the case in two of the patients presented. Debridement of these regions proceeded with sharp dissection using the microdebrider, and no significant bleeding was encountered.
It is difficult to determine the optimal treatment for patients with chronic invasive fungal sinusitis, which was observed in three of our four patients. Most reports describe surgical debridement in conjunction with long-term antifungal medications.7,12 There is no clear consensus regarding the extent of surgical debridement that is necessary to achieve favorable outcomes. Recommendations in the literature vary from aeration of the involved sinuses to complete surgical removal of diseased tissue. 7 Although radical resections may allow for more complete disease resection, they can be associated with greater surgical morbidity. In addition, it is unclear whether radical resections improve prognosis in these patients. In general, surgery does not lead to complete eradication of pathogenic fungal organisms. Instead, reduction of fungal load through surgery provides time for medical therapy and reversal of immune dysfunction to have an impact on the course of disease. 13 Endoscopic approaches allow appropriately aggressive resections while minimizing surgical morbidity.
In our series, several of the patients had poor outcomes despite aggressive surgical and medical management. Based on endoscopic evaluation and MRI studies, disease in the infratemporal fossa was successfully cleared in all patients in this series. Intracranial extension of disease developed in two patients despite aggressive surgical and medical treatment. Residual microscopic disease, in conjunction with an ongoing immunocompromised state, may have contributed to disease progression in these patients. One other patient chose to not undergo additional treatment because of overall worsening of his health status related to graft versus host disease and died with disease after being placed on comfort care. Despite these poor outcomes, our experience shows that the surgical approach described provides excellent visualization and access to all areas of the infratemporal fossa. The endoscopic approach allows for effective debridement of disease in the pterygopalatine and infratemporal fossa regions in patients with invasive fungal sinusitis.
Conclusions
Invasive fungal sinusitis can commonly involve the infratemporal fossa by way of direct extension from the pterygopalatine fossa. The infratemporal fossa can be safely debrided via an endoscopic transnasal technique. The endoscopic approach has several advantages over traditional open approaches including lower morbidity and lower risk of seeding disease at uninvolved sites. The approach also makes it easier to perform surveillance for disease resolution or recurrence after treatment. Increased experience with this approach may permit endoscopic management of a greater variety of pathologic entities involving the infratemporal fossa.