
Abstract
Background
Endoscopic sinus surgery (ESS) has been the most important technical advance in surgical rhinology in the last 25 years. The technique is now used beyond its initial sinus confines but knowledge of the forces required to perform ESS is limited. Greater understanding of these forces will lead to improved surgical training and safety. The aim of this study was to quantify the magnitude of the forces exerted during punch osteotomy of the bony lamella of the paranasal sinuses and surrounding bony structures during ESS.
Methods
Fifteen formalin-fixed cadaveric heads underwent simulated ESS. Peak axial forces were measured using a pair of modified Blakesley forceps. Measurements were recorded during osteotomy of the paranasal sinus complex, skull base, and crests of the optic nerve and internal carotid artery. Statistical comparison between the mean forces was performed.
Results
A mean force of 6.06 N was required to breach the lamellae of the ethmoid sinus complex. This was significantly less than the mean force required to breach the skull base, excluding the olfactory cleft (17.80 N; p < 0.0001), crests of the optic nerve (15.43 N; p < 0.001), and internal carotid artery (13.15 N; p < 0.001). There was no significant difference between the ethmoid lamella and the lamina papyracea (6.13; p = 0.67).
Conclusions
Significantly greater force was required to breach the skull base and other safety critical areas encountered in ESS, than the bony lamellae of the ethmoid sinus complex. Although this result is reassuring, in vivo studies are now required to validate this relationship in the operative patient.
Keywords
Endoscopic sinus surgery (ESS) has been the most important technical advance in surgical rhinology. 1 It has allowed the conversion of traditional intranasal ethmoidectomy techniques into precise minimal access surgery, with the use of the Hopkins rod lens telescope. 2 Since the Messerklinger technique was popularized by Stammberger 3 and Kennedy 1 , further applications of the surgery have been realized, and the technology has extended to application beyond the nose and sinuses and its related pathologies.4,5
The technique of endoscopic sinus surgery requires a variable number of punch osteotomies through the thin intersinus septae of the ethmoid sinus. The extent of the surgery is individualized, according to the patient's disease severity. 3 Extensions of the surgery beyond the ethmoid and into the other paranasal sinuses are similarly disease determined.
Decisions regarding force application during endonasal surgery rely on the previous experience of the surgeon, gained during cadaver dissection training and live surgery. A surgeon has no other way of knowing whether the forces that are being applied are appropriate and, similarly, the surgeon trainer has only the display on the operative monitor to determine whether a trainee is using appropriate levels of force.
Although it is known that the thickness of ethmoid bone varies greatly,6,7 little is known about variation in tensile strength or the magnitude of surgical force necessary for ethmoidectomy. Two previous studies8,9 have shown forces ranging between 2 and 12 N are needed to breach ethmoid bone but neither of these studies were performed using surgical instruments. The aim of the current study is to investigate the magnitude of the axial forces exerted when punch osteotomies are performed within the paranasal sinuses and surrounding structures during ESS.
Method
Data
Fifteen cadaveric heads, fixed in formalin, were used. Force measurement data were obtained from a series of osteotomies performed on each of the cadaver heads. Each osteotomy was made by applying force to the instrument in an axial plane until the bony septa fractured, replicating forces generated during live patient ESS. The study assessed areas of the cadaver head that would routinely be breached during ESS as well as those that would not.
Force Measuring System
A pair of Blakesley forceps (Storz, Slough, U.K.) was modified with the addition of a custom-made load cell to each arm to measure the force applied through each of the arms (Figs. 1 and 2). The specific design has been previously described. 10 The load cells were calibrated to detect loads up to 19.61 N (2 kg) and were encased in epoxy resin for protection.
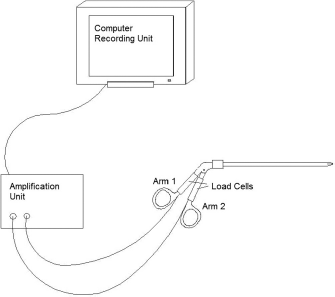
Schematic of the force measuring system.
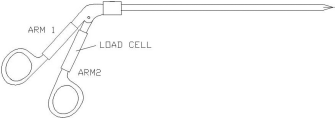
The modified Blakesley forceps (Storz, Slough, U.K.).
Data Recording
Signals from the load cells were software amplified and filtered before logging and display. Measurement was confined to loads in the axial plane in this study, continuing until a sinus septal break point occurred. An example of the type of force curves recorded is shown in Fig. 3. When gripping forces were required to stabilize the instrument, these forces were also recorded by the load cells but subsequently removed by subtraction to leave only the axial force.
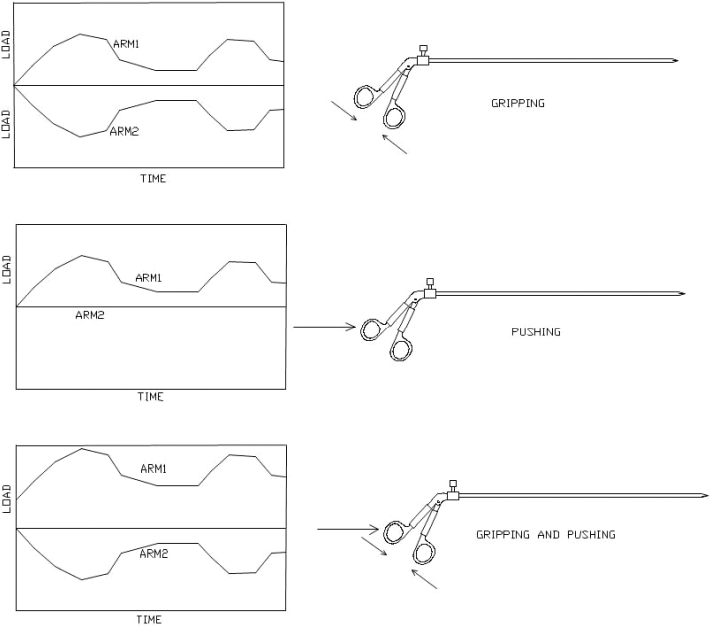
The force curves generated by the force measuring system.
Statistical Analysis
The data collected were analyzed using SPSS Version 14 (SPSS, Inc., Chicago, IL). Wilcoxon signed-rank tests were used to compare data between different anatomic areas.
Results
Of the 15 cadaveric heads used, 10 were men and 5 women (mean age at death, 82 years; range, 48–94 years). These provided 28 individual sinus complexes on which force measurements could be performed. Two sides were not suitable for assessment because of previously undertaken anatomic dissection. All of the cadavers had been deceased for <1 year at the time of the study.
Table 1 shows the mean force required to perform the osteotomies for each of the measured anatomic locations. In addition, an overall mean is given for associated regions within the cadaveric heads.
Bone partition and mean force (N) required for break point to occur
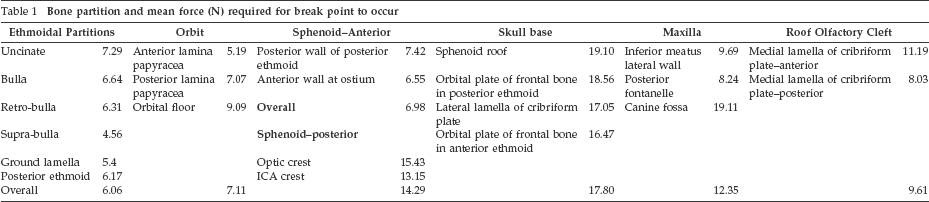
The majority of osteotomies usually performed during ESS fall within the lamella of the ethmoid sinuses. The mean force required to break septa in this area was 6.06 N (range, 4.56–7.29 N). On occasion, it may be required to access the sphenoid sinus, and the mean forces measured at this location were similar to those in the ethmoid complex: mean = 7.42 and 6.55, measured at the posterior wall of posterior ethmoid and the anterior wall at the ostium, respectively.
There was greater force required to penetrate areas not normally accessed during routine ESS. The forces required for skull base penetration, excluding the olfactory cleft, were on average 17.80 N; 80% of these penetrations required a force that exceeded the instrument maximum (19.61 N). There was a significant difference between this and the mean force required for penetration of the lamella of the ethmoidal sinuses (p < 0.0001). There was no significant difference between the forces required to penetrate the lamina papyracea and the ethmoidal sinus lamella (p = 0.670). Although there was no significant difference between the forces required to penetrate the anterior wall of the sphenoid sinus and the ethmoidal lamella (p = 0.074), the force required to penetrate the crests of the optic nerve (mean = 15.43 N) and the internal carotid artery (mean = 13.15 N) were significantly greater than that for the anterior sphenoid (p < 0.001). It was noted that clinical dehiscence of the ICA crest occurred in 30% of the specimens used.
Discussion
Surgery requires exacting control of instruments and an understanding of the forces involved. Forces are classified as contact or noncontact. Contact forces are those including friction, tension, and reaction. Noncontact forces include gravity and electrical forces. The force of a puncture osteotomy is a reaction force acting against a tension force within the bone and is therefore a contact force. Surgeons need to understand both types of forces to perform surgery effectively and safely.
This study shows that it is possible to measure the contact forces required to perform routine ESS, as well as those that would result in serious complications (Fig. 4). The results indicate that there is a significant difference between forces required to break through the sinus septae of the ethmoid complex compared with those giving rise to breach of the noncribriform skull base, crest of the optic nerve, and crest of internal carotid.
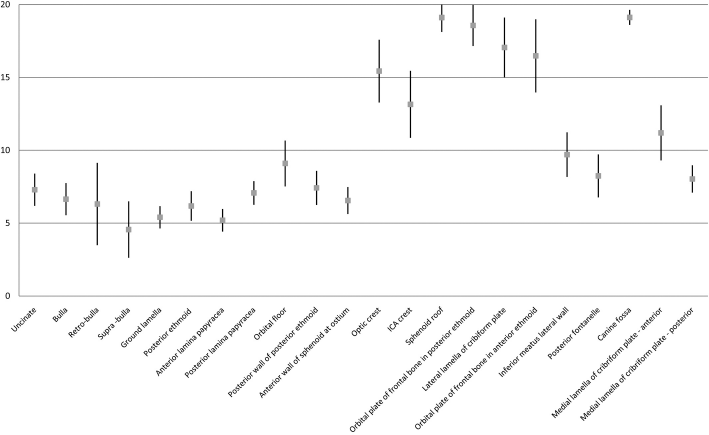
Anatomic site of osteotomy (mean force [N] with standard error bars).
Two other groups have published sinus osteotomy force data. Wagner et al. 8 bilaterally measured five formalin-fixed heads, using a torque sensor mounted on an endoscope to perform osteotomies. Waridel et al. 9 published results on 21 sectioned specimens preserved in 40% ethanol. A dynamometer was used to measure breaking force perpendicular to the osteotomy site. Comparison with these previous smaller studies shows some similarities (Table 2). In all of the studies the skull base requires the greatest force to penetrate. However, the means in other areas vary, recording the lowest penetrating force in different areas of the skull in each of the studies. This may result from variations in the techniques used to measure force. The current study used a modified surgical instrument, which measured force in an axial plane, and, therefore, represents the closest simulation to real surgery of the three studies.
Comparison of forces with other studies
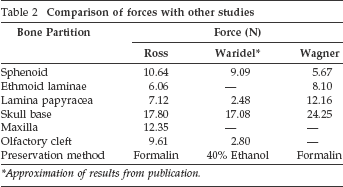
Approximation of results from publication.
Limitations
The cadaveric model preserved in formalin may not behave in the same manner as in vivo studies, because of the methods used to preserve the cadavers. Fresh freezing may provide a data source closer to the in vivo situation. The cadavers used are from an aged and, in some case, diseased population. This may have had an unpredictable effect on the bone density and strength of the sinus lamellae.
Future Direction
We anticipate a number of applications arising from the information gained from this study. The first application is to use real-time force measurement as a safety device during ESS. By knowing the normal limits of osteotomy forces, a feedback alarm system that would activate if the force applied was excessive could be developed. This would compliment current safety systems such as three-dimensional image guidance. As with facial nerve monitoring, it could be a useful adjuvant to safer surgery, particularly in training. The data recording system in this study is not currently viewed directly in the surgeons’ line of sight. There are no feedback mechanisms other than direct visualization of the recording monitor. It is planned, with further developments and feedback from this study, to improve this system. This will allow easy integration into current endoscopic systems and improve the surgeon's experience.
The second application is in relation to the future development of ESS. It has been proposed that robotic assistance will improve the procedure beyond its current form. 11 Robotic techniques are already favored in some centers for gynecological, general, and urological procedures. 12 Work on the development of these robots required research into the forces and tissue elasticity to create safety and feedback systems. We will need to build on the force data we have, to allow systems for robotic ESS to be developed. Having established that ex vivo data collection is possible, the next step is an in vivo study, which we are currently working toward.
Conclusions
This study shows that in a cadaveric simulation, the forces required to breach the ethmoid sinus complex partitions are less than those required to breach the skull base. These measurements will provide essential data for not only the development of safety systems, but also the future design of robot-assisted surgery and surgical training models.
Footnotes
Acknowledgment
The authors are grateful to Mr. Simon Denley for advice on statistical matters.
The authors had no conflicts of interest