
Abstract
Background
The etiology of sinonasal inverted papilloma (IP) is unknown. This study was designed to evaluate the possible risk factors associated with IP
Methods
This is a case-control epidemiology study in a tertiary referral center. Fifty patients with IP and 150 matched controls were interviewed using a questionnaire on suspected risk factors. Univariate analysis of the risk factors and calculation of the matched odds ratios, the corresponding 95% CIs, and p values was performed. Significant risk factors were further studied using conditional logistic regression analysis.
Results
Outdoor and industrial occupations were associated with IP. Tobacco smoking, drinking alcohol, history of allergic rhinitis, sinusitis, nasal polyp, non-sinonasal papilloma and non-sinonasal malignancy were not significant factors.
Conclusions
Outdoor and industrial occupations were associated with IP and may be potential risk factors. Future studies are warranted to further evaluate the individual type of occupation and chemical involved.
Keywords
Inverted papilloma is notorious for its high recurrence rate and association with malignancy. The etiology of IP is unknown. As identification of the associated risk factors may help in the prevention of this tumor, this article aims at studying the possible risk factors associated with IP.
Subjects and Methods
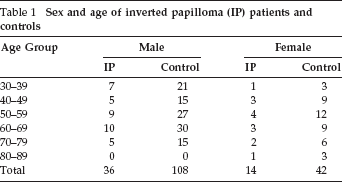
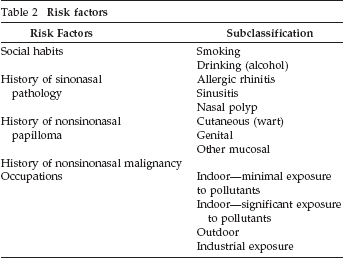
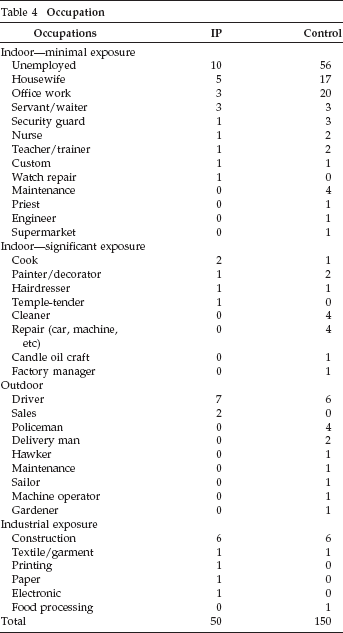
Fifty patients with IP seen from 1990 to 2007 were recruited for retrospective study from the rhinology clinic of the Prince of Wales Hospital. From January 2007 to June 2008, 150 controlled subjects were prospectively recruited from the general otorhinolaryngology clinic. The age and sex of patients were matched with the controls according to the categories listed in Table 1. To select a group of controls with clinical data closely representing that of the local population, patients presenting with sinonasal pathology, middle ear and mastoid pathology, and head and neck malignancy were excluded. All patients were interviewed using a questionnaire containing the history of exposure to the possible risk factors listed in Table 2. The severity of tobacco smoking habit was classified into light (<20 cigarettes/day) and heavy (>20 cigarettes/day). The severity of allergic rhinitis was classified according to a modified Allergic Rhinitis and Its Impact on Asthma classification (Table 3). 1 The occupations of the patients were classified into four different categories according to their nature and degree of exposure to pollutants (Table 4). Univariate analysis of the risk factors and calculation of the matched odds ratios, the corresponding 95% CIs, and p values was performed (chi-square exact test). The significance of the identified risk factors from the univariate analysis was further analyzed by conditional logistic regression using the forward stepwise (likelihood ratio) method. The power of the sample size for the study was assessed by the biostatistician using the nQuery Advisor (Elashoff 2000, Statistical Solutions, Ltd., Saugus, MA). When the sample size is 192, the logistic regression test (level of significance, 0.050 two sided) will have 80% power to detect an odds ratio of 1.50.
Sex and age of inverted papilloma (IP) patients and controls
Risk factors
Modified Allergic Rhinitis and Its Impact on Asthma (ARIA) classification of allergic rhinitis
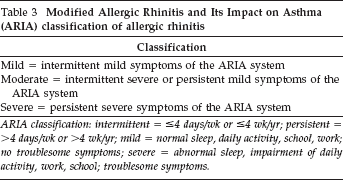
ARIA classification: intermittent = ≤4 days/wk or ≤4 wk/yr; persistent = >4 days/wk or >4 wk/yr; mild = normal sleep, daily activity, school, work; no troublesome symptoms; severe = abnormal sleep, impairment of daily activity, work, school; troublesome symptoms
Occupation
Results
Details of patients’ smoking habits are listed in Table 5. In all of the patient subgroups, the percentage of smokers was higher among the IP patients than among the controls. Using the chi-square test, only the odds ratios for heavy smoking was statistically significant (odds ratio, 3.05; 95% CI = 1.02–.00; p = 0.02). However, heavy smoking was not a significant factor when the data were analyzed by conditional logistic regression (odds ratio, 2.62; 95% CI = 0.64–10.66; p = 0.18).
Statistical analysis of the risk factors
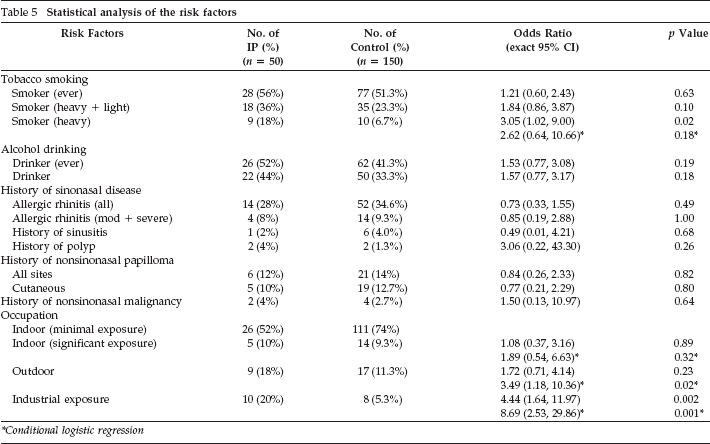
Conditional logistic regression
Details of patients’ drinking habits are listed in Table 5. The percentage of alcohol drinkers was higher among the IP patients than among the controls (44% versus 33.3%). None of the odds ratios for the drinking risk factor in the subgroups studied were statistically significant.
Details of patients’ previous history of sinonasal diseases are listed in Table 5. The overall percentage of patients with a history of allergic rhinitis was lower in the IP group than in the control group (28% versus 34%). The percentage of patients with sinusitis was lower in the IP group than in the control group (2% versus 4%). The percentage of patients with a history of nasal polyps was higher in the IP group than in the control group (4% versus 1.3%). None of these factors were statistically significant risk factors for IP.
Details of patients’ previous history of nonsinonasal (cutaneous, mucosal, and genital) papillomas are listed in Table 5. The percentage of patients with a history of nonsinonasal papillomas over the body was comparable in the two groups of patients (12% versus 14%). The percentage of patients with a history of cutaneous warts was also comparable in the two groups (10% versus 12.7%). These were not significant risk factors for IP (odds ratio, <1).
Details of patients’ previous histories of nonsinonasal malignancy are listed in Table 5. Two patients in the IP group had carcinoma of the colon. There were four patients with a history of nonsinonasal malignancy in the control group, including two with carcinoma of the breast, one with carcinoma of the cervix, and one with non–head and neck lymphoma. Although the odds ratio for the risk factor of history of malignancy was >1, it was not statistically significant.
Details of patients’ occupational risk factors are listed in Table 5. Ten patients (20%) in the papilloma group had industrial exposure, which included construction, textile, printing, paper, and electronics industries. Eight patients (5.3%) in the control group had industrial exposure, in the construction, textile, and food processing industries. By univariate analysis, the odds ratio of the risk factor of industrial exposure was 4.44 (95% CI = 1.64–1.97), which was statistically significant (p = 0.002). When all of these factors were further analyzed by conditional logistic regression, the outdoor occupation group (odds ratio, 3.49; 95% CI = 1.18–10.36; p = 0.02) and industrial exposure group (odds ratio, 8.69; 95% CI = 2.53–29.86; p = 0.001) were found to be significant risk factors (Table 5). Driver was the most common outdoor occupation in both the tumor and control group, accounting for 14% of the former and 4% of the latter. Construction was the most common industry in both the tumor and the control group, accounting for 12% of the former and 4% of the latter.
Discussion
The etiology of IP is unknown. Previously postulated etiologic factors include smoking, exposure to pollutants and toxic chemicals, nasal allergy, viral infection, sinusitis, nasal polyp, nonsinonasal malignancies, and genital and dermal warts.2–17 Tobacco smoking has long been suggested to be a significant risk factor for IP. Phillips et al. reported that 75% of their 112 patients had a history of significant use of tobacco. 2 Buchwald et al. reported 67% of smokers in their study of 82 patients. 3 Barbieri et al. studied 70 patients and found that 75% of the male patients were smokers. 4 Snyder et al. reported 50% smokers in 28 patients. 5 Although these studies showed a high prevalence of smokers in the IP patients, they were not analytical studies. The only reported case-control trial was performed by Deitmer and Wiener who compared the smoking habits of 47 IP patients with 47 matched controls and found no significant difference. 6 In our study, the percentage of smokers among IP patients (36%) was lower than the percentages reported previously. Although the odds ratios for heavy smoking subgroups was statistically significant by univariate analysis (Table 5), the significance of heavy smoking was not further substantiated by conditional logistic regression analysis. We also studied the patients’ drinking habits. Although the percentage of drinkers in the IP group was higher than in the control group, the odds ratio was not statistically significant (Table 5).
Inflammation, allergic rhinitis, sinusitis, and polyps have been suggested to play a role in the pathogenesis of IP. Roh et al. found that the inflammatory cell population was significantly greater in IP compared with other Schneiderian papilloma. 7 Snyder et al. reported a history of allergy in 21% of 28 patients. 5 Buchwald et al. reported 14% of hay fever or asthma in 82 patients. 3 Kramer and Som commented that although infection was frequently present in their 86 patients, there were too few epithelial papillomas to correlate adequately with the high incidence of nasal inflammation and infection. 8 Barbieri et al. found that 40% of the 70 IP patients they studied suffered from chronic sinusitis and sinonasal polyps. 4 Orlandi et al. reported a statistically significant increase in CT evidence of contralateral rhinosinusitis in patients with unilateral IP when compared with controls and those with unilateral malignancy. 9 However, no previous case studies had shown a causal relationship between these sinonasal pathologies and IP. Our study showed that the percentage of patients with allergic rhinitis was lower in the IP group than in the control group (28% versus 34.6%; Table 5). The percentage of patients with a history of sinusitis and polyps was comparable in the two groups (6% versus 5.3%). These figures were much lower than those reported by Barbieri et al. Since excluding patients presenting with sinonasal pathology in the controls recruited from our general otorhinolaryngology clinic may lead to inaccurate estimation of the rate of sinonasal diseases, more accurate estimation in future studies can be obtained by omitting this exclusion criteria and recruiting controls directly from the general population.
Several studies have reported the presence of human papilloma virus (HPV) in IP. Kashima et al. reported positive findings of two HPV-6 and six HPV-11 in 29 IPs. 10 Beck et al. reported an overall incidence of 62% of positive HPV in 39 IP. 11 Kim et al. found that 12.3% of their IP specimens showed HPV DNA (all in early grade lesions) and suggested that HPV infection occurs as an early event during the multistep tumorigenesis of IP. 12 Fu reported clinical evidence of seven genital warts and two skin warts in nine consecutive patients with nasal papilloma including five fungiform and four mixed fungiform and IPs and suggested that autoinoculation may play a role in the etiology of such tumors. 13 Contrary to Fu's report, our study showed that only 12% of the IP patients had histories of nonsinonasal papillomas, which included mostly warts of cutaneous origin and that this figure was comparable with that of the control group (14%; Table 5). The findings may be explained by the fact that our papillomas were inverting rather than squamous. Our findings may also imply that autoinoculation may not be a significant route of viral transmission in IP.
It is well known that IP has malignant transformation potential. Mirza et al. reviewed 63 case series and identified 163 (7.1%) cases of synchronous carcinoma of 2297 cases of IP. 14 Metachronous carcinoma were reported in 74 (3.6%) cases of 2047 cases of IP. 14 In our study, none of the patients with IP had synchronous or metachronous sinonasal malignancy. The relationship between IP and nonsinonasal malignancy has rarely been reported. Dictor and Johnson reviewed a cohort of 197 patients with IP and compared it with a matched cohort of 1583 patients with nasal polyps. 15 Nine cases of nonsinonasal head and neck malignancy were found in the former group compared with only seven cases in the latter. 15 The odds ratio for acquiring nonsinonasal squamous cell carcinoma of the head and neck was 10.3 (95% CI = 3.9–27.4). 15 In our study, only two IP patients (4%) compared with four controls (2.7%) had histories of nonsinonasal malignancy, and none of these malignancies were in the head and neck region (Table 5). Although the odds ratio for association with nonsinonasal malignancy was 1.50 (95% CI = 0.13–10.97), it is not statistically significant (p = 0.64).
It is still disputed whether exposure to pollutants and toxic chemicals is a significant contributory factor to the development of IP. Herrold reported the induction of epithelial papillomas of the nasal cavity in Syrian hamsters when diethylnitrosamine was administered i.p., intradermally, and by skin painting. 16 Majumdar and Beck reported an uneven distribution of the incidence of tumors in Sheffield, where 13 of 24 male patients (54%) worked in the steel industry. 17 They speculated that environmental factors may play a role. Deitmer and Wiener performed a case-control study on 47 patients with matched controls and found a significantly higher degree of occupational exposure to different kinds of smoke, dust, and aerosol in their case group. 6 They reported an odds ratio of 6.67 (error probability, 0.025) for exposure to inhalation to noxious substances. They speculated that noxious occupational exposure is one of the promoters of the pathogenesis of IP. Barbieri et al. found that occupational exposure to wood and leather dust, chromium and nickel vapors, and formaldehyde was associated with only 5% of the 70 patients studied. This proportion is too low to establish a causal relationship with IP. Our study found that 10 of 50 IP patients (20%) had industrial exposure in the construction, textile, printing, paper making, and electronic industries (Table 5). This figure was higher than that of the control group (8/150, 5.3%), which included construction, textile, and food processing industries. We found that the odds ratio of this risk factor for industrial exposure as a whole was statistically significant (logistic regression: odds ratio, 8.69; 95% CI = 2.53–29.86; p = 0.001). Construction worker was the most common occupation with industrial exposure in both the IP and the control group. The number of patients in each industry was too small to pinpoint a particular chemical or pollutant associated with IP. We also found that an outdoor occupation as a whole was also a statistically significant factor associated with IP (logistic regression: odds ratio, 3.49; 95% CI = 1.18–10.36; p = 0.02). In this category, being a driver was the most common occupation in both the IP and the control group. Additional multicenter studies with a larger patient number are required to evaluate the significance of being a driver and construction worker. One possible drawback of our study is the documentation of only the latest occupation of the patients at the time of IP diagnosis, which may have underestimated the effect of previous occupational exposure. Future studies should include detailed analysis of the occupational history, particularly for those retired and those with frequent change of occupation.
Conclusion
Outdoor and industrial occupations were associated with IP and may be potential risk factors. A multicenter study with larger patient numbers is suggested to further study the significance of the individual occupation and chemical involved.