
Abstract
Background
The delivery of topical intranasal corticosteroid sprays has traditionally been the primary method of treating recurrent nasal polyposis. An emerging treatment for polyposis is budesonide nasal irrigations. Delivered at concentrations nearly 100 times greater than found in prescription nasal sprays, there have been little studies on the effects of budesonide irrigation on the adrenal axis. Therefore, we investigated whether irrigation with budesonide solution was associated with any increase in serum cortisol and 24-hour urinary cortisol levels.
Methods
Patients who previously had undergone endoscopic sinus surgery and were not taking prednisone for 3 months were prospectively enrolled in this study. Patients irrigated twice daily with 0.5 mg/2 mL of budesonide mixed with 240 mL of saline solution. Serum cortisol and 24-hour urinary cortisol were collected before drug administration and 6 weeks after continuous use.
Results
Ten patients completed this study. The average serum cortisol and 24-hour urinary cortisol before drug administration were 9.8 ± 5.4 μg/dL and 28.1 ± 15.1 μg/24 hours, respectively. After 6-week follow-up, the average serum cortisol and 24-hour urinary cortisol were 12.8 ± 3.5 μg/dL and 16.5 ± 5.6 μg/24 hours, respectively. Normal ranges for serum cortisol and 24-hour urinary cortisol are 5–25 μg/dL and 4–50 μg/24 hours, respectively.
Keywords
Rhinosinusitis is a common disorder accounting for an estimated 30 million physician office visits in the United States each year.1,2 Despite multiple attempted treatments, including an estimated 500,000 surgeries per year, 3 the disease continues to be a major health problem, both in expenditures and in poor quality of life.1,4
The medical management of chronic rhinosinusitis (CRS) focuses on treatment of the underlying inflammatory disorder. The use of topical and systemic corticosteroids is common among otolaryngologists, 5 given their inhibitory effects on inflammatory pathways.6–9 Intranasal corticosteroids are commonly used as first-line treatment modalities for patients with CRS. One such topical agent, budesonide, is a potent anti-inflammatory corticosteroid designed to have a high ratio of topical to systemic activity, and this agent has been proven safe and effective in multiple investigational studies10–16 when applied intranasally. Although systemic corticosteroids exert more potent control of the underlying inflammatory pathway in chronic sinusitis, these medications have significant side effects such as agitation, dyspepsia, elevated intraocular pressure, exacerbation of hypertension, weight gain, fluid retention, osteoporosis, avascular necrosis of the hip, and hypothalamic-pituitary-adrenal (HPA) axis dysfunction.
In a topical form, more potent forms of intranasal corticosteroid irrigations have bypassed traditional controlled trials, and physicians continue to use them without evidence of safety or efficacy. Therefore, this study was undertaken to assess the effect of topical budesonide saline irrigations on systemic cortisol levels.
Methods
Patients ≥18 years of age who had previously undergone endoscopic sinus surgery (ESS) and had evidence of recurrent polyposis were enrolled in this study. All recruited patients had not taken any form of systemic corticosteroids for at least 3 months before enrollment. Patients <18 years of age; pregnant women; and patients with immune dysfunction, known HPA axis dysfunction, or prior pituitary or adrenal surgery were excluded from this study. This study was approved by the Institutional Review Board. Patients were not paid for participation in this study. Patients were instructed to perform irrigation twice daily using budesonide, 0.5 mg/2 mL, mixed in 240 mL of saline solution (1 L of distilled water, 1 tsp of noniodinated salt, and 1 tsp of baking soda) using a commercially available irrigation bottle (NeilMed, Santa Rosa, CA).
Serum cortisol levels were drawn by licensed phlebotomists between the hours of 6 and 8 A.M. and were assessed at baseline (pretreatment) and at 6 weeks (posttreatment) during the study period. In addition to serum cortisol assays, patients were given preservative-free containers for 24-hour urine collections to assess cortisol and creatinine levels. Collections were performed at baseline and at 6 weeks. All patients adhered to the following urine collection protocol. On the morning of day 0, patients were instructed to void in the usual fashion without collecting any urine. For the remainder of day 0, patients were instructed to collect any urine in the container. On the morning of day 1 after awakening, patients were instructed to collect the morning (final) void in the container. Patients were instructed to seal and refrigerate the container when not being used for collection. After the final void, patients were instructed to return the container that day for processing.
Results
Seventeen patients were enrolled in this study. Ten patients completed the study. Of the 17 initial recruits, 7 patients were eliminated from analysis because of noncompliance with collection protocols or were eliminated due to administration of prednisone as a result of symptom breakthroughs. All patients had previously undergone ESS and had evidence of recurrent polyposis. Additionally, no patient enrolled in the study had taken any oral corticosteroid for at least 3 months before enrollment.
Overall, posttreatment cortisol assessment did not reveal any abnormal decreases in either serum cortisol or 24-hour urine cortisol levels (Fig. 1). Baseline serum cortisol levels (normal range, 5–25 μg/dL) were found to be 9.8 ± 5.4 μg/dL. After 6 weeks of twice-daily budesonide/saline irrigation, morning serum cortisol levels were 12.8 ± 3.5 μg/dL. Baseline 24-hour urinary cortisol levels (normal range, 4–50 μg/24 hours) were 28.1 ± 15.1 μg/24 hours. Baseline urine creatinine was 1.46 g/24 hours (0.63–2.50 g/24 hours). After 6 weeks of twice-daily budesonide/saline irrigation, 24-hour urinary cortisol levels were 16.5 ± 5.6 μg/24 hours. Posttreatment creatinine was 1.30 g/24 hours (0.63–2.50 g/24 hours).
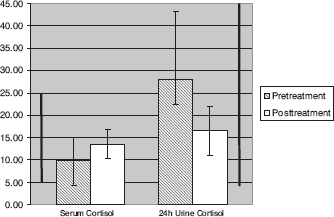
Graphic representation of pretreatment and posttreatment cortisol levels. Pretreatment serum cortisol levels were 9.8 ± 5.4 μg/dL. Posttreatment serum cortisol levels were 12.8 ± 3.5 μg/dL. Pretreatment 24-hour urinary cortisol levels were 28.1 ± 15.1 μg/24 hours and posttreatment 24-hour urinary cortisol levels were 16.5 ±5.6 μg/24 hours. Vertical bars represent reference ranges for serum cortisol (left) and 24-hour urine cortisol (right).
Discussion
The use of topical Food and Drug Administration (FDA)–approved corticosteroids is widespread5,17,18 and safe10–16,19 for the treatment of allergic rhinitis. Only mometasone, however, has been approved by the FDA for the treatment of nasal polyps, and no topical steroid spray has FDA approval for the treatment of CRS. In practice, the local delivery of corticosteroids is advantageous over the systemic deployment of corticosteroids because the adverse effects of systemic corticosteroids are theoretically avoided. The use of topical corticosteroids has been studied20–22 in a randomized fashion in the management of CRS and these studies have revealed overall improvements in CRS symptoms as well as improvements in inflammatory profiles, 20 mucociliary clearance, 22 and sinus ostia patency. 23
An increasing trend in the treatment of allergic rhinitis and CRS is the off-label use of corticosteroids such as otic formulations of ciprofloxacin/dexamethasone, ophthalmic tobramycin/dexamethasone, and budesonide respules in place of conventional, aerosolized corticosteroid sprays. These formulations continue to be used intranasally without evidence of safety. The high degree of vascularity in the nasal mucosa makes systemic absorption of these topically applied medicines a legitimate concern. Nevertheless, there are few data on the effect of nonaerosolized corticosteroid formulations in the sinonasal cavity and no data on the safety of budesonide irrigations. We undertook this study to assess whether budesonide respules (0.5 mg/2 mL) mixed in 240 mL of saline solution had any effect on the adrenal system when used twice daily for 6 weeks.
Cortisol is an endogenous corticosteroid that is commonly assessed as a screening index of HPA axis dysfunction. Cortisol is a glucocorticoid produced in the zona fasciculata and the zona reticularis of the adrenal cortex. Serum levels of cortisol vary depending on time of day with the highest levels recorded in the early morning and lowest levels shortly after the onset of sleep. Serum levels of cortisol are regulated by levels of adrenocorticotropic hormone (ACTH), which in turn is also regulated by the hypothalamic peptide corticotropin–releasing hormone. Cortisol, as well as exogenous corticosteroids, has a negative feedback effect on ACTH. The result of ACTH inhibition is the suppression of adrenal cortex production and release of endogenous corticosteroids or lowered cortisol levels. 24 It is this suppression and the resulting reduction of endogenous cortisol that is a primary concern of clinicians using exogenous corticosteroids on a long-term basis.
Cortisol levels are assessed primarily through serum and urine assays. Cortisol levels in serum exhibit diurnal variation, with the highest levels during 6 and 10 A.M. and the lowest levels occurring around 12 A.M. 24 Therefore, ranges for serum cortisol and time have been established. The range for serum cortisol during 6–10 A.M. are 5–22 μg/dL. In the urine, ∼1% of cortisol is secreted in the unconjugated form and the rest as metabolites. The normal range for urine cortisol is 4–50 μg/24 hours.
The safety of topical budesonide has been well established in the past 25 years of its use. A literature review performed by Boner 25 found only one study that identified an adverse effect of intranasal budesonide on the HPA axis, which was shown by decreased 24-hour urinary cortisol; the remainder of the investigations revealed no long-term effects on the HPA by budesonide.
Möller and colleagues 16 studied pressurized intranasal budesonide in 43 children with perennial rhinitis over 12 months and aqueous intranasal budesonide for an additional 6 months. No significant changes in statural growth and bone age were observed, and morning plasma cortisol and 24-hour urine cortisol levels were not changed during the treatment period. The authors concluded that long-term (1–2 years) treatment with intranasal budesonide was safe and did not result in HPA dysfunction.
A double-blinded, crossover study comparing budesonide, 200 μg; budesonide, 400 μg, and placebo was undertaken by Balle et al. 12 to assess clinical outcomes and adrenal effects. In addition to a low side-effect profile, aerosolized budesonide was found to have no effect on adrenal function in 36 patients, including the higher dose of budesonide. Similarly, Algorta and coworkers 14 recently performed a randomized crossover trial of two doses of topical budesonide to assess the safety and systemic bioavailability. Eighteen adults were enrolled and the effects on the HPA were assessed with plasma cortisol levels. No significant differences in cortisol levels in the two doses of topical budesonide was observed, and values obtained were within baseline reference ranges for serum cortisol.
Pichler and colleagues 10 compared the effects of intranasal topical budesonide, 400 μg, and intramuscular injections of 80 mg of methylprednisolone for the treatment of seasonal allergic rhinitis over a period of 3 weeks. Patients treated with methylprednisolone had significantly lower cortisol assays after 7 days.
Our study indicates that topical application of budesonide in the form of irrigation is safe and does not result in changes in the HPA axis as evidenced by normal posttreatment serum and 24-hour urine cortisol levels. This compares favorably with previous studies using FDA-approved aerosolized and aqueous formulation of topical budesonide. Because no patient in this study showed a decrease in posttreatment serum cortisol and 24-hour urine cortisol levels, provocation tests of the HPA axis (e.g., ACTH stimulation or cosyntropin stimulation) were not indicated.
The primary objective was to assess safety in adult patients using a specific dose of budesonide (0.5 mg/2 mL). We have not studied this irrigation in children or pregnant women; therefore, no conclusions can be drawn about the safety of budesonide irrigations in these patient groups. Additionally, known complications of systemic corticosteroids such as osteopenia, glaucoma, hyperglycemia, etc. were not specifically studied as well. Therefore, we can draw no conclusions about the relationship between long-term budesonide irrigations and these medication-related complications. However, we suspect that given the lack of evidence for cortisol level derangements, the likelihood of these complications is probably low.
The sample size in this study is a notable limitation. It is possible that our sample size was too small to detect any derangements in serum or urinary cortisol levels. We believe, however, that this would have been a concern were we to identify patients with data outside the reference ranges. As such, no patient had abnormal levels of serum cortisol, urine cortisol, or urine creatinine identified; therefore, there were no outliers in the data analysis.
It should be noted that the time frame for this study was 6 weeks. It is also possible that were budesonide irrigations studied for longer periods of time, there might be evidence of reductions in either serum or urine cortisol levels. Finally, one should note that budesonide respules are manufactured in three doses (0.25, 0.5, and 1.0 mg/2 mL); this study evaluated budesonide, 0.5 mg/2 mL; therefore, conclusions can not be drawn regarding the 1.0-mg/2 mL concentration and its safety. Follow-up studies on these patients could be performed to assess long-term safety of budesonide irrigations.
Conclusions
When used to irrigate the sinonasal cavity twice daily in patients with recurrent polyposis after functional ESS, budesonide at 0.5 mg/2 mL mixed in 240 mL of saline solution appears to be safe based on the results of serum and urine cortisol assays.