
Abstract
Background
Mucociliary clearance is impaired in chronic rhinosinusitis (CRS). Clearance of sinonasal secretions is influenced by its rheological properties. The purpose of this study was to describe the rheological properties of sinonasal mucus in patients with CRS and correlate them with disease severity.
Methods
Twenty-three adult subjects with CRS underwent collection of sinonasal secretions. Samples were analyzed using the AR2000 cone and plate rheometer (TA Instruments, New Castle, DE) to determine the dynamic viscosity and elasticity. These properties were used to calculate mucus clearance indices. All patients completed the Sinonasal Outcome Test (SNOT-20). Recent sinus computed tomography (CT) scans were electronically reviewed and scored according to the Lund-McKay staging system.
Results
The mean dynamic elasticity and viscosity of sinus mucus at 1 Hz were 78.24 ± 103.4 Pa and 22.09 ± 29.62 Pa, respectively. The mean elasticity and viscosity values at 10 Hz were 118.9 ± 155.5 Pa and 32.36 ± 45.58 Pa, respectively. Three indices of disease severity (SNOT-20 score, Lund-McKay score, and nasal polyps) correlated with increased mucus viscoelasticity and/or worsened mucociliary clearance indices (MCIs).
Conclusions
This study establishes the range of rheological properties of sinonasal mucus in patients with CRS and suggests an association between disease severity and MCIs.
Mucus is cleared from the paranasal sinuses and nasal cavity by ciliated epithelial cells. Mucociliary clearance depends on ciliary function, properties of the mucus, and patency of the sinus ostia. In chronic rhinosinusitis (CRS), there is a hypersecretion of thick mucus and mucociliary clearance is reduced. 1
Rheology is the study of flow and deformation of complex fluids such as sinonasal mucus. Mucus is “viscoelastic” and possesses both liquid and solid-like characteristics. Viscosity refers to the capacity to respond to deforming forces by flowing. Elasticity refers to the ability to resist deformation by storing energy and recoiling. Viscoelasticity is conferred by mucins (high molecular weight glycoproteins) via covalent bonds, hydrogen bonds, and van der Waals forces. 2
Mucus must be viscous and elastic for effective clearance from the airway. Elasticity permits efficient energy transmission from cilia to mucus, and viscosity allows mucus to be displaced. 3 However, excessive viscosity and elasticity may impair clearance. In the frog palate model, an increase in viscosity resulted in a decreased mucociliary transport rate. 4 To a degree, a decrease in elasticity correlates with better mucociliary transport.5,6 However, some elasticity is necessary for cilia to transmit their kinetic energy to mucus and a further loss of elasticity results in slower transport.
Mucus is also cleared from the lower airway passages by coughing, which is analogous to the action of sneezing or nose blowing to clear sinonasal secretions. The sudden high velocity airflow temporarily reduces crosslinking within the mucus, causing it to propel forward. Mucus that is highly elastic will resist forward motion, resulting in recoil after the cough event. 3
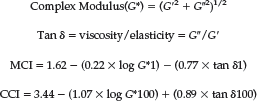
Using formulas developed from experimental models,4,7 the efficiency of mucociliary and cough clearance can be predicted using the viscoelastic properties of mucus. Rheometers can determine mucus viscosity and elasticity at a range of applied frequencies. Cilia beat with a frequency up to 10 Hz, or from 1 to 3 Hz when under a mucus load. 8 The mucociliary clearance index (MCI) is calculated using lower frequencies (1 rad/s, or ∼0.16 Hz), whereas the cough clearance index (CCI) is calculated using higher frequencies (100 rad/s, or ∼16 Hz) to approximate those generated in the airway during a cough or sneeze:
Most rheologically based studies have focused on lower airway processes such as asthma, and there are relatively few studies pertaining to sinonasal mucus.9–11 In CRS patients, mucus viscosity has been reported between 0.68 (±0.41) and 25.5 (±8.6) Pa, and elasticity has been reported from 10.6 (±8.4) to 253.6 (±57.5) Pa.9–11 Notably, these studies used an oscillating sphere magnetic rheometer, which analyzes only the portion of the specimen within immediate proximity to the sphere. Also, mucus samples were frozen after collection and stored for up to 24 hours before analysis, further contributing to potentially unreliable results.
For the present study, the AR2000 rheometer (TA Instruments, New Castle, DE) was used to analyze mucus samples. It is a sensitive cone-and-plate rheometer that uses very low strains to generate a signal, which is crucial for analyzing mucus without disturbing molecular bonds. In contrast to the oscillating sphere rheometer, the AR2000 rheometer analyzes the entire mucus sample between the cone and plate (Fig. 1). In addition, most samples (91%) in this study were analyzed within 45 minutes of collection, and all were analyzed within 3 hours.
Rheological abnormalities of lower airway secretions have been correlated with disease severity in patients with cystic fibrosis. 12 This investigation applies contemporary rheological measurements to the study of sinonasal secretions in patients with CRS and correlates these findings with clinical aspects of each patient's disease process.
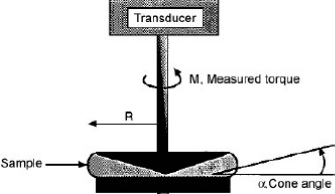
Diagram of sample analysis by cone-and-plate rheometer.
Methods and Materials
Description of Subjects
The study population consists of adult (age >18 years) patients attending routine appointments in the Otolaryngology–Head and Neck Surgery outpatient clinic and/or undergoing prescheduled endoscopic sinus surgery at the University of California, San Francisco Medical Center. All patients carried a diagnosis of CRS based on the definition set forth by the 2003 Rhinosinusitis Task Force. 13
Collection of Sinonasal Mucus in Outpatient Clinic
As per clinic routine, each patient was treated with intranasal phenylephrine and tetracaine sprays before undergoing nasal endoscopy. Patients whose examinations revealed collections of mucus within the sinus cavities or sinus drainage pathways were then informed of the study protocol and were offered participation. Sinonasal mucus was collected under endoscopic guidance with a sinus suction attached to a specimen trap. Two factors were used to determine the site of mucus collection during the study: abnormal appearance (color and perceived thickness) and ease of access. The specimen was immediately placed on ice pending transportation to the laboratory.
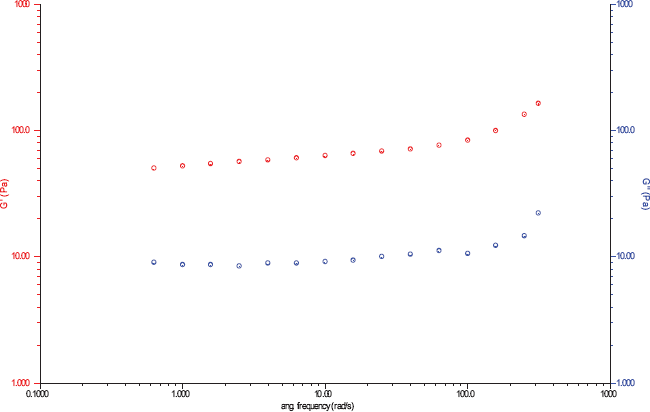
Frequency sweep of mucus specimen from 0.1 to 50 Hz. G′ (left) corresponds to elastic modulus. G″ (right) corresponds to viscous modulus.
Collection of Sinonasal Mucus in the Operating Room
Patients were informed of the study protocol and were offered participation in the preoperative holding area. All patients received intranasal oxymetazoline sprays. Sinonasal mucus was collected under rigid endoscopic guidance with a sinus suction attached to a specimen trap. Mucus was collected from either the sinuses or their drainage pathways at the time that significant collections were identified during the course of the planned surgery. The specimen was then placed on ice pending transportation to the laboratory.
Completion of the Sino-Nasal Outcome Test (SNOT-20)
At the time of each specimen collection, whether in the clinic or in the preoperative area, each subject completed the SNOT-20. Enrolled subjects who were seen multiple times completed a new SNOT-20 form with each specimen collection.
Review of Clinical Data
Each subject's medical record was reviewed by the study investigators to record gender, age, diagnosis of cystic fibrosis or asthma, number of prior sinus surgeries, and treatment with oral steroids, intranasal steroids, oral antibiotics, and sinonasal irrigations. If the subjects had undergone a sinus computed tomography (CT) scan within the past 6 months, the images were reviewed and the Lund-McKay score 14 was calculated.
Rheological Measurements
Each sample was analyzed with the AR2000 cone-and-plate rheometer. A 1-mL aliquot of the specimen was placed on the rheometer plate and allowed to equilibrate for 1 minute at 20°C. A range of oscillatory frequencies (0.1–50 Hz) was applied to the specimen at a constant strain of 1% to measure viscosity and elasticity (Fig. 2). Viscosity and elasticity were recorded at 1 and 10 Hz and also at 1 (∼0.16 Hz) and 100 rad/s (∼16 Hz).
Statistical Analysis
Statistical analysis was performed using SPSS software (SPSS, Inc., Chicago, IL), release 13.0. Data are presented as means ± SD. Student's t-test for independent samples and the Pearson product-moment correlation coefficient were used. This study was approved by the Committee for Human Research at the University of California, San Francisco.
Results
Twenty-three subjects, 11 men (48%) and 12 women (52%), were included in this study. Six subjects had secretions collected on two occasions, bringing the total number of samples to 29. Twenty-four collections occurred in the outpatient clinic and five occurred in the operating room. Mucus samples were encountered and collected from within the paranasal sinuses (maxillary, ethmoid, frontal, and sphenoid) and the sinus drainage pathways (middle meatus and sphenoethmoidal recess). The locations of mucus procurement did not differ for collections performed in the operating room versus the clinic (Table 1). Subject age ranged from 20 to 72 years (mean, 38 ± 13 years). The study population included 18 patients with nasal polyps (78%), 8 patients with cystic fibrosis (35%), and 17 patients with asthma (74%). Seventeen patients (74%) had undergone prior sinus surgery, and the number of prior surgeries ranged from 0 to 7 (mean, 1.8 ± 1.7).
Sites of mucus sample collections
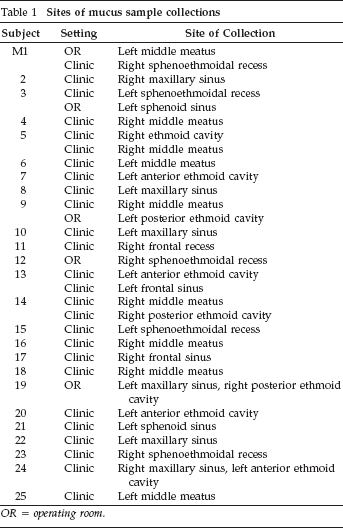
OR = operating room.
Excluding multiple collections on the same subject, the mean elasticity and viscosity of mucus at 1 Hz were 78.24 ± 103.4 Pa and 22.09 ± 29.62 Pa, respectively. The mean elasticity and viscosity values at 10 Hz were 118.9 ± 155.5 Pa and 32.36 ± 45.58 Pa, respectively.
Table 2 outlines the relationships between all predictor variables and the six measures of mucus viscoelasticity and clearance. The mean SNOT-20 score for the study cohort was 1.8 ± 1.2 and the median score was 1.3. Higher SNOT-20 scores (suggesting more severe symptoms) predicted increases in mucus elasticity and viscosity at 1 and 10 Hz. There was also a strong trend toward a lower MCI (indicating poorer clearability) that did not attain significance (r = 0.39; p = 0.06).
Subject characteristics and nasal mucus viscoelasticity and clearance
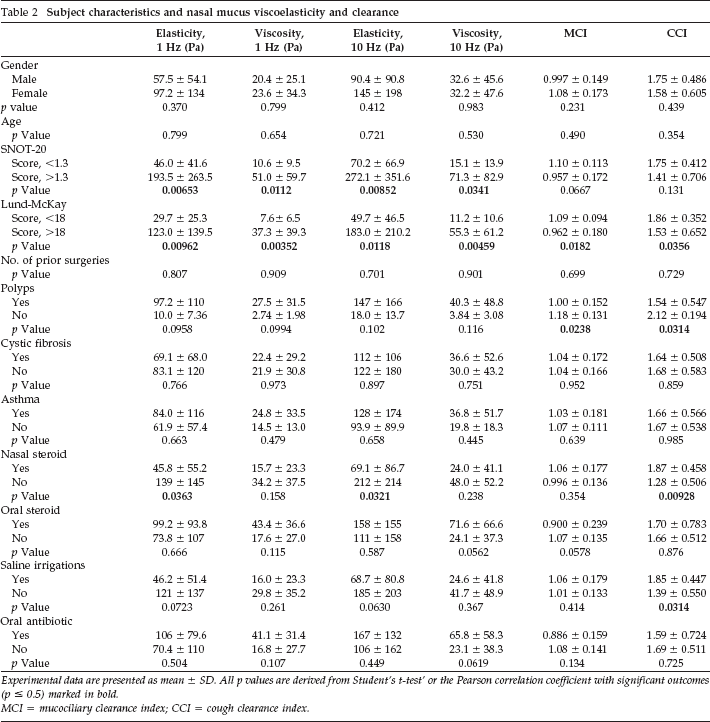
Experimental data are presented as mean ± SD. All p values are derived from Student's t-test’ or the Pearson correlation coefficient with significant outcomes (p ≤ 0.5) marked in bold.
MCI = mucociliary clearance index; CCI = cough clearance index.
Sinus CT scans were available for 18 subjects. The mean Lund-McKayscore for the population was 17 ± 4.6 and the median score was 18. A greater Lund-McKay score correlated with higher values for all measures of mucus viscoelasticity and predicted a worse MCI and CCI.
In the 18 patients (78%) with nasal polyposis, mucus showed a worse MCI (1.00 versus 1.18; p = 0.02) and CCI (1.54 versus 2.12; p = 0.03). The use of topical nasal steroids and saline irrigations correlated with lower mucus elasticity and improved CCIs. Age, gender, and the presence of asthma and cystic fibrosis did not correlate with viscoelasticity or clearability.
Two subjects underwent collection of sinonasal mucus from multiple sites during one visit and these samples were analyzed separately to gauge how much variance might be encountered within one subject. In both cases, the mucus was analyzed as having similar viscoelastic qualities (Table 3).
Rheological characteristics of sinonasal mucus taken from multiple sites in the same subject

MCI = mucociliary clearance index; CCI = cough clearance index.
Six subjects underwent collection of sinonasal mucus on two different occasions (mean = 25 days apart). For some subjects, the mucus clearability values did not change significantly (Table 4). In cases where a change in mucus clearability was observed, there were also changes in the SNOT-20 score that suggested an interim fluctuation in the disease severity. Subject 1 was tested before and after a functional endoscopic sinus surgery procedure and was noted to have significant improvements in SNOT-20 score (1.20 versus 2.75) and MCI (1.17 versus 0.69) postoperatively.
Rheological characteristics of sinonasal mucus taken from subjects on two different occasions
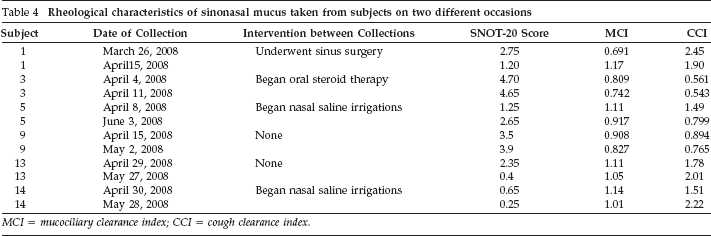
MCI = mucociliary clearance index; CCI = cough clearance index.
Discussion
The mean dynamic viscosity values of 22.09–32.36 Pa and the mean dynamic elasticity values of 78.24–118.9 Pa found in the present study of CRS patients are significantly greater than those found (viscosity of 1.6 Pa and elasticity of 31.8 Pa) in the most recent report in the literature, which used an oscillating sphere rheometer to analyze frozen sinonasal mucus specimens. 11 This discrepancy may be accounted for by several reasons. This study was performed using a cone-and-plate rheometer, which is able to analyze the viscoelasticity of the entire submitted mucus specimen. Also, we were able to analyze fresh specimens immediately after procurement instead of freezing them for later analysis, which likely disrupts the molecular bonds within mucus that dictate viscoelastic properties. Rheologic values from this study are much greater than the optimal viscosity of 0.2 Pa and elasticity of 20 Pa required for maximal transport rate in the frog palate model, 4 suggesting the impaired clearance of pathological secretions in CRS.
This study shows that increases in mucus viscoelasticity and impairment of mucus clearability (as measured by the MCI and CCI) correlate with the severity of sinus disease, as determined by SNOT-20 results, radiographic findings, and the presence of nasal polyps. Pathological mucus consists of greater concentrations of glycoproteins 15 and other molecules such as immunoglobulins and DNA. 11 Products of ruptured leukocytes such as DNA and actin filaments, along with immunoglobulins and lysozyme, form bonds to each other and the glycoproteins and increase mucus viscoelasticity. What remains unclear is whether treatments that alter the viscoelastic properties of mucus would result in improved mucociliary clearance and, subsequently, clinical improvement in CRS patients.
There are limitations with this study's design and data analysis. Mucus was suctioned from the sinonasal cavities in a subjective fashion depending on ease of access and appearance of secretions. No efforts were made to collect all visible mucus, and it is possible that a sampling bias occurred if the “selected” mucus differed from that left behind. However, in two patients mucus was sampled from discrete locations and, although this small sample size precludes quantitative analysis, rheologic properties were similar.
Because of a small sample size, a multivariate analysis was not performed. This raises the possibility of interference between predictor variables (i.e., subjects using nasal steroids and saline irrigations concurrently). Finally, because of the nature of this observational study, it is impossible to establish a causative relationship between mucus rheologic properties and sinusitis severity or treatment effects.
Conclusion
The viscoelasticity of sinonasal mucus can be accurately quantified using the cone-and-plate rheometer. Severity of disease as measured by symptom scores, imaging findings, and the presence of nasal polyps correlates with higher viscoelasticity and poorer MCIs.
Footnotes
Acknowledgements
Acknowledgment of financial support: none to report