
Abstract
Background
Primary ciliary dyskinesia (PCD) is a clinically uniform entity, although cilia motility and structure can vary among patients, making diagnosis difficult. Chronic sinusitis, bronchiectasis, sinus hypoplasia, secretory otitis media, and low fertility are common in PCD patients. The aim of this work was to correlate nasal ciliary activity with clinical and structural abnormalities in PCD. A secondary aim was to evaluate the usefulness of high-resolution digital high-speed video (DHSV) in the diagnosis of PCD.
Methods
We analyzed nasal mucociliary transport and cilia ultrastructure by electron microscopy and studied nasal ciliary beat frequency (CBF) and beat pattern using high-resolution DHSV imaging in 34 healthy volunteers, 25 individuals with PCD (including 11 with Kartagener's syndrome [KS]with situs inversus), and 27 with secondary ciliary dyskinesia (SCD).
Results
Nasal mucociliary transport was defective in the PCD and SCD patients. Ciliary immotility was observed in only six KS patients and was correlated with the absence of dynein. We observed a correlation between partial dynein deficiency and an uncoordinated, stiffly vibrating ciliary beat. Cilia activity and structure were normal in the SCD patients.
Conclusion
Nasal mucociliary transport showed a sensitivity of 100% for the diagnosis of PCD but has low specificity. High-resolution DHSV imaging has high sensitivity and specificity for the diagnosis of PCD. Video analysis is probably more useful than the study of mucociliary transport and cilia ultrastructure in screening for PCD. The absence of dynein was correlated with ciliary immotility and was more common in KS patients.
Keywords
Although a clinically uniform entity, PCD is seen to consist of a number of subgroups when examined by electron microscopy. Dynein deficiency affects 70–80% of patients, but cases of patients with PCD and KS with normal ciliary ultrastructure have been reported. 5 Given that a number of ciliary abnormalities are also observed after infections and inflammations, which is referred to as secondary ciliary dyskinesia (SCD), the diagnostic value of a single ultrastructural abnormality or even normality is limited. 6 Mucociliary function can be deficient in patients with alterations in cilia or mucous, and thus the study of mucociliary transport appears to be inadequate for use in distinguishing between PCD and SCD. Electron microscopy is an imperfect method for evaluation of the functional capacity of ciliated epithelia. Several other diagnostic tools have been used. 7 Recently, new high-resolution digital high-speed video (DHSV) imaging has allowed the precise beat pattern, in addition to the ciliary beat frequency (CBF), to be viewed in different planes, in slow motion, and frame by frame, 8 which may be helpful in the diagnosis of PCD. 9
The aim of this study was to assess the use of DHSV imaging for correlating the CBF and pattern with clinical and structural abnormalities responsible for PCD. A secondary aim was to evaluate the usefulness of DHSV imaging in the diagnosis of PCD and SCD.
Methods and Patients
Preparation and Culture of Human Ciliary Airway Epithelial Cells and CBF Measurement Using DHSV Imaging
Samples of ciliary airway epithelial cells were obtained from the middle nasal concha using curettage 10 without local anesthesia, in a period during which acute infection was absent. The experiments were approved by the local ethics committee, and written consent was obtained before sampling. Medication was discontinued 48 hours before nasal brush biopsy.
The tissue sample was immersed in 1 mL of Dulbecco's modified Eagle's medium (DMEM; Cambrex, East Rutherford, NJ) supplemented with 10% fetal calf serum (FCS), 2 mM of glutamine, penicillin (100 U/mL), and streptomycin (100 μg/mL), and turned over until partial dissolution occurred. Then, 150 μL of each nasal epithelium biopsy specimen was plated on tissue culture plates (12-well Corning Costar 3513), which had been coated with 0.5% gelatin (Panreac Química, Madrid, Spain) to promote adherence of the ciliated cells. The CBF of healthy individuals and of SCD, PCD, and KS patients was measured at room temperature (23–27°C) within 30 minutes after biopsy. To corroborate the results, each nasal biopsy specimen was plated on tissue culture plates coated with human collagen (type IV, Vitrogen-100; Cohesion Technologies, Palo Alto, CA) and incubated in DMEM at 37°C in a humidified atmosphere of 5% CO2 in air for 24 hours, and the CBF was measured again.
Samples were imaged with a DHSV imaging technique using an Eclipse TS100 microscope (Nikon, Tokyo, Japan) with a 40× Nikon phase-contrast objective, providing a final optical gain of 400×. The method used for CBF measurement was based on previous published methods by Salathe et al. (1999)11,12 with appropriate modifications. Briefly, a Multimetrix XA3051 power source (Desintec S.L., Valencia, Spain) was used with transillumination provided by visible and red-filtered 150-W halogen lamps (Desintec). The light path was directed through the multi-image module to a CCD camera (CV-A33 CL digital quad high-speed progressive scan camera; JAI UK Ltd., Unbridge, UK) with a resolution of 649 (horizontal) × 494 (vertical) pixels and a maximum resolution velocity of 120 frames/s. Video signals were digitized and processed with an HP Workstation (xw6200, Xeon 3.4 GHz; Hewlett-Packard, Madrid, Spain) with an acquisition device for images (PCIe-1429, full-configuration Camera Link image acquisition, National Instruments Spain, Madrid, Spain). Using software we developed (DESINSOFT-BIO 200; Desintec), contrast-enhanced video images were selected, and the light intensities of the selected pixels were recorded on a frame-by-frame basis. In addition, the magnitude spectra from a fast Fourier transform of the pixel intensity signal were computed online and displayed on the workstation monitor, to provide direct feedback on the quality of the recorded intensity signal. The frequency and time resolution of the CBF measurement were 0.5 Hz and 2 seconds, respectively. We analyzed the variations of intensity of six different regions (3 × 3 pixels) of the cilia in individual cells in a minimum of 10 cells/patient. The classification of the ciliary beat pattern was based on that of Chilvers et al. 13 with modifications. We considered five different modes: (1) immotile cilia; (2) coordinated, stiffly vibrating ciliary beat pattern; (3) uncoordinated, stiffly vibrating ciliary beat pattern; (4) uncoordinated beat pattern; and (5) normal ciliary beat pattern. We classified the pattern as vibrating when the amplitude of bending in the cilia was reduced.
Nasal Mucociliary Transport
Nasal mucociliary transport was assessed using a radioisotopic technique involving serum albumin labeled with metastable technetium-99 (99mTc) according to previously published protocols. 14 Nasal mucociliary transport velocities of >4 mm/minute were considered normal.
Ciliary Ultrastructure
Biopsy samples were obtained from the middle nasal concha and processed as described previously. 15 Ciliary ultrastructure was classified according to the latest ranking of Afzelius 5 for dynein and microtubular abnormalities. We studied at least 100 ciliary cross-sections per patient. Dynein arms (inner, outer, or both) were considered absent (no outer or inner dynein arms) when the mean number of dynein arms counted in all cross-sections was less than two per cross-section. Inner dynein arms were considered absent when the mean count was <0.6 arms/cross-section; and outer dynein arms, when the mean count was <1.6/cross-section. Biopsy specimens were considered to have few outer or inner dynein arms when the mean count was less than seven or less than three per cross-section, respectively. In comparison with normal cilia, cilia with short dynein arms had a small projection of dynein from the microtubule. Ciliary orientation was considered normal when deviation from the ciliary axis was less than 28°. The 9 + 2 microtubule pattern was considered altered when alterations were present in >30% of the cilia16,17 (Fig. 1).
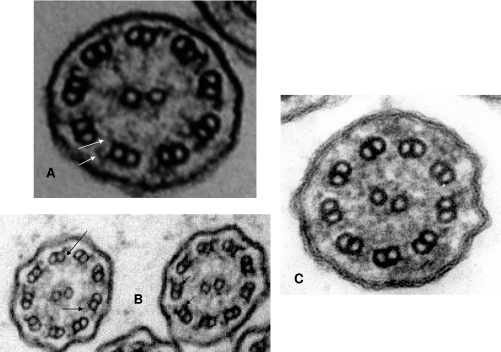
Cross-sections of ciliary axonemes showing ultrastructural alterations in primary ciliary dyskinesia (PCD) cilia compared with normal cilia. (A) Normal cilia with dynein (arrows). (B) Deficiency of inner dynein arms (arrows), corresponding to case 3 (Kartagener's syndrome [KS]) in Table 4, with ciliary dyskinesia. (C) Absence of dynein, corresponding to case 1 (KS) in Table 4, with cilia immotility.
Patients
A total of 34 healthy volunteers were included in the analysis, to determine the normal CBF and ciliary beat pattern in our population. To compare the CBF and ciliary beat pattern between PCD and KS patients, 14 PCD and 11 KS patients were included. PCD patients included those without SI, whereas those with SI were considered to be KS patients. Patients were classified according to their clinical features. A deficit of sinus pneumatization was classified as hypoplasia or aplasia of the frontal sinus (patients <15 years of age were classified as not applicable). Other clinical features included pansinusitis (total or partial occupation of all sinuses; patients <15 years were classified as not applicable), bronchiectasis, secretory otitis media, polyposis, family history of chronic respiratory disease, respiratory allergy, and infertility in patients >18 years of age. Male infertility was determined by a spermiogram, with the patient's consent; otherwise, the patient was classified as not applicable. Female patients were considered infertile after failure to become pregnant after trying for 3 years; otherwise, the patient was classified as not applicable (Table 1).
Ciliary beat frequency (CBF), clinical demographics, and ciliary ultrastructure of patients diagnosed with primary ciliary dyskinesia (PCD), and Kartagener's syndrome (KS)
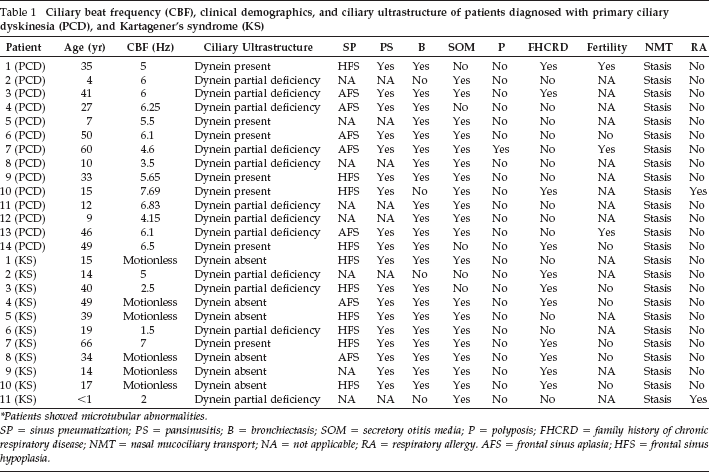
* Patients showed microtubular abnormalities.
SP = sinus pneumatization; PS = pansinusitis; B = bronchiectasis; SOM = secretory otitis media; P = polyposis; FHCRD = family history of chronic respiratory disease; NMT = nasal mucociliary transport; NA = not applicable; RA = respiratory allergy. AFS = frontal sinus aplasia; HFS = frontal sinus hypoplasia.
Diagnoses were made based on clinical features, ciliary ultrastructure, high-resolution computed tomography (for SI detection, sinus pneumatization, sinusitis, and bronchiectasis), and nasal mucociliary transport. In the 25 patients, ciliary activity analyzed by DHSV was dyskinetic or absent. A sweat test was performed in children, to exclude cystic fibrosis. For 27 patients previously diagnosed with PCD (Table 2), the diagnosis was revised to SCD, because normal ciliary beat pattern and frequency were obtained by DHSV imaging. A previous diagnosis of PCD was confirmed in patients with chronic respiratory infections by determining deficient nasal mucociliary transport on two occasions, spaced 6 months apart.
Ciliary beat frequency (CBF), clinical demographics, and ciliary ultrastructure of patients diagnosed with secondary ciliary dyskinesia (SCD)
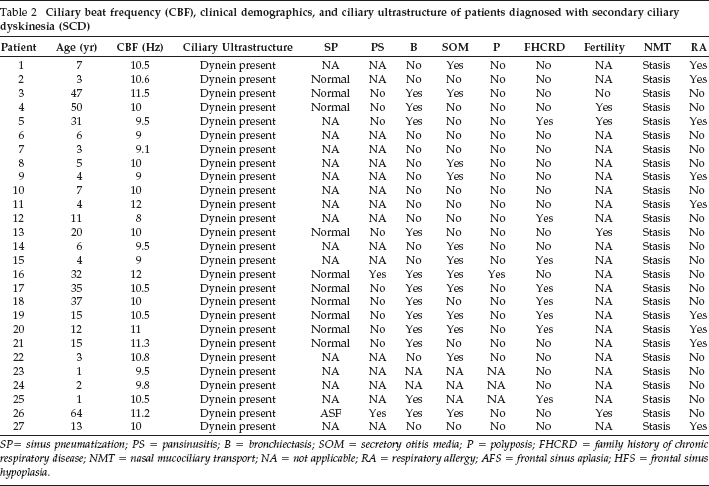
SP= sinus pneumatization; PS = pansinusitis; B = bronchiectasis; SOM = secretory otitis media; P = polyposis; FHCRD = family history of chronic respiratory disease; NMT = nasal mucociliary transport; NA = not applicable; RA = respiratory allergy; AFS = frontal sinus aplasia; HFS = frontal sinus hypoplasia.
Statistics
The data are presented as means ± SEM for n experiments. The statistical analysis was performed by analysis of variance (ANOVA) followed by Bonferroni's test, using GraphPad software (GraphPad, San Diego, CA). Significance was accepted for p < 0.05.
Results
The clinical characteristics of the PCD and KS patients are summarized in Table 1, and those of the SCD patients are summarized in Table 2. The study results are summarized in Table 3.
Synopsis of the results
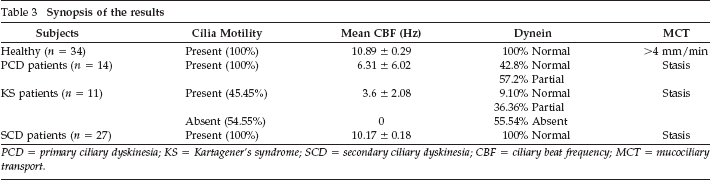
PCD = primary ciliary dyskinesia; KS = Kartagener's syndrome; SCD = secondary ciliary dyskinesia; CBF = ciliary beat frequency; MCT = mucociliary transport.
CBF and Pattern in Healthy Volunteers and in PCD and KS Patients
In 34 healthy volunteers, the mean CBF was 10.89 ± 0.29 Hz with a coefficient of variation (CV) of 2.66% (Fig. 2). By optical microscopy, a normal ciliary beat pattern was observed, characterized by a planar motion with a forward power stroke and a backward recovery stroke in a coordinated mode. No ultrastructural alterations were seen.
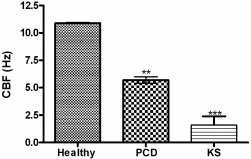
Ciliary beat frequency (CBF) in 34 healthy individuals, 14 primary ciliary dyskinesia (PCD) patients, and 11 Kartagener's syndrome (KS) patients. CBF was measured using digital high-speed video (DHSV) imaging as described in the Methods section. Results are expressed as means ± SEM (**p < 0.01, ***p < 0.001).
CBF and Pattern in PCD Patients
In the 14 PCD patients, the mean CBF was 6.31 ± 0.38 Hz with a CV of 6.02% (Fig. 2). Six PCD patients (42.8%) were classified as having dynein, but with a low CBF. Eight patients were classified as having a partial dynein deficiency. No PCD patient had an absence of dynein or immotile cilia. Stasis in nasal mucociliary transport was common to all of the PCD patients. There was 100% correlation between dynein alterations and an uncoordinated, stiffly vibrating ciliary beat. In four patients, cilia containing dynein showed a normal ciliary beat pattern, but low CBF. Two cases with cilia containing normal dynein showed an uncoordinated ciliary beat pattern (Table 4). The CBF of cilia from PCD patients did not change after 24 hours in primary ciliary cell culture.
Assessment of ciliary beat frequency (CBF), ciliary beat pattern, and microtubule and dynein abnormalities by digital high-speed video imaging and transmission electron microscopy in primary ciliary dyskinesia (PCD) and Kartagener's syndrome (KS) patients

The English in this document has been checked by at least two professional editors, both native speakers of English. For a certificate, see www.textcheck.com/certificate/AqRsZh
CBF and Pattern in KS Patients
In our cohort of 11 KS patients, 5 patients showed ciliary movement (Tables 1 and 3). Four of these (KS patients 2, 3, 6, and 11) also displayed partial dynein deficiency, with CBFs of 5, 2.5, 1.5, and 2 Hz, respectively. In KS patient 7, the cilia had dynein and a CBF of 7 Hz, which was higher than the mean CBF (3.6 ± 2.08 Hz) for the five KS patients with ciliary movement. An absence of dynein and immotile cilia were observed in the other six KS patients (54.5%). Only one KS patient (9%; KS patient 7; Table 4) had normal dynein and a coordinated, stiffly vibrating ciliary beat pattern. Therefore, absence of dynein and immotile cilia were more common in KS patients than in PCD patients (Table 4).
In all KS patients, nasal mucociliary transport was absent. Ciliary immotility was observed in 100% of the KS patients who had a total absence of dynein, whereas patients with partial dynein deficiency exhibited an uncoordinated, stiffly vibrating ciliary beat, with the exception of patient 7, who showed a coordinated, stiffly vibrating ciliary beat pattern (Table 4). The mean CBF of cilia from KS patients was 1.6 ± 0.79 Hz (Fig. 2) and did not change after 24 hours in primary ciliary cell culture.
SCD Diagnosed in 27 Patients Previously Diagnosed with PCD
The diagnosis of 27 patients previously diagnosed with PCD based on the absence of nasal mucociliary transport (stasis) was revised to SCD. The mean CBF of cilia from these patients was 10.17 ± 0.18 Hz, nearly the same as that in the healthy volunteers, and the ciliary beat pattern was normal. All SCD patients had cilia with dynein and no microtubular abnormalities.
Discussion
In this study, we used DHSV imaging to examine the associations between the CBF and pattern and the clinical, structural, and genetic abnormalities responsible for PCD. The first step in the diagnosis of PCD was to detect the absence of nasal mucociliary transport. In our study, as in recent previous reports,18–20 stasis in this single test showed 100% sensitivity for a diagnosis of PCD (Table 1), but the specificity was low, because all patients with SCD also showed stasis. The mucociliary stasis observed in SCD derives in most cases from alterations in the quantitative and qualitative composition of airway secretions, but can also be caused by transient dyskinesia associated with microtubular abnormalities that are reversible with appropriate treatment.21,22
The PCD and KS patients had clinical features in common, as described previously. 5 However, in our study, SI was more frequent in patients exhibiting an absence of dynein. Thus, it may be that in patients with minor dynein deficiencies of the cilia, some motility is retained by both respiratory and nodal cilia, and SI may not appear. 16 As in other studies, 4 infertility mainly affected male patients; female patients were also affected, but to a lesser degree.
To improve the diagnosis of PCD, we developed a DHSV imaging technique that allowed us to define the CBF and pattern associated with specific dynein and microtubular abnormalities. However, except for 9 + 0, microtubule pattern variations are of little or no value in the diagnosis of PCD and are considered secondary. Dynein arm deficiencies appear to be congenital and are more common.7,16 Our results regarding CBF in healthy volunteers were in agreement with previous reports of frequencies between 9 and 15 Hz.23,24 We observed that the absence of dynein (no outer or inner dynein arms) was partnered with immotile cilia in six KS patients (100% correlation). On the other hand, combined defects in inner and outer dynein arms (few or short) were found in three PCD and three KS patients, who had a mean CBF of 3.83 Hz. When we separately considered inner and outer dynein arm defects, we found a mean CBF of 5.31 Hz in the six patients, with no difference between inner versus outer dynein arm defects. A study with a larger number of patients is needed to corroborate these results, because other studies have correlated ciliary motility with specific deficiencies in the inner or outer dynein arms.13,25–27
As described in the Methods section, we considered two groups, patients with PCD and patients with KS. The PCD patients showed defects in the inner dynein arms, the outer dynein arms, or both arms, as well as the presence of normal dynein, but dynein was not absent from any of the patients in this group (Table 4). However, 6 of the 11 KS patients had a total absence of dynein, which explains the low mean CBF in KS patients.
Our patients displayed four different ciliary beat patterns: (1) immotile cilia, with a 100% association with the absence of both inner and outer dynein arms; (2) an uncoordinated, stiffly vibrating pattern, which correlated with defects in the inner dynein arms, the outer dynein arms, or both; (3) an uncoordinated pattern with normal dynein, found in two PCD patients; and (4) a normal ciliary beat pattern with a low CBF, in patients with dynein present. We found no isolated alterations of microtubules and no abnormalities of ciliary beat pattern or frequency that could be attributed to such abnormalities.
Conclusions
Our results show that the DHSV imaging technique has high sensitivity for the detection of abnormalities in the CBF and pattern, with high specificity for differentiating between PCD and SCD. This is a rapid technique that can reliably guide the diagnosis of SCD and PCD. In contrast, mucociliary transport has low specificity for this purpose. The absence of dynein was correlated with ciliary immotility and was more common in KS patients. Thus, SI would be expected to correlate with immotile cilia and absence of dynein.