
Abstract
Background
Chronic rhinosinusitis (CRS) is an inflammatory disease in which bacteria are commonly implicated often in the form of a biofilm. Manuka honey has been shown in vitro to be an effective treatment against two common CRS pathogens both in the planktonic and in the biofilm forms. The purpose of this study was to determine if the application of manuka honey to respiratory epithelium would result in histological evidence of epithelial injury.
Methods
Using a rabbit animal model, a nonrandomized controlled trial of four treatment regimes was performed with two rabbits in each group. The left nasal cavity was irrigated with a 1.5-mL manuka honey solution once daily and the right nasal cavity was not treated. Groups 1–3 were treated for 3, 7, and 14 consecutive days, respectively, and killed the morning after the last treatment. Group 4 was treated for 14 consecutive days followed by a 14-day washout period and then killed the following morning. The nasal respiratory mucosa was immediately harvested after death. The mucosa was examined by light microscopy for histological change in comparison with the control side.
Results
Cilia were not measured quantitatively but were equally present on the treated and untreated mucosa. There was no histological evidence of inflammation, epithelial injury, or significant morphological changes.
Conclusion
The application of a manuka honey solution to rabbit nasal respiratory mucosa over different treatment intervals did not show evidence of histological epithelial injury.
Keywords
Chronic rhinosinusitis (CRS) is a common inflammatory disease that is multifactorial in etiology. There is sufficient evidence that bacteria, in either planktonic or biofilm form, are largely involved in causing chronic inflammation and it is plausible that bacterial biofilms are responsible for the persistence of disease in a significant proportion of patients.
Irrigation has been shown to be an effective method for the delivery of saline and topical antibiotic therapy to the postoperative sinonasal cavity.1,2 Honey is a natural product that has been used for hundreds of years to treat infection. Manuka honey has been recently shown in vitro to be an effective cidal agent for the treatment of Pseudomonas aeruginosa and Staphylococcus aureus in the form of a biofilm. 3 The current study sought to examine the histological effect of manuka honey on respiratory epithelium.
Methods
This investigation was approved by the Animal Care Committee at the University of Ottawa after successful Internal Scientific Merit Review by the Faculty of Medicine, Office of the Vice Dean (Research).
Manuka Honey Treatment
Eight New Zealand white rabbits were treated once daily with a 1.5-mL, 33% mixture of manuka honey with saline. A nonrandomized controlled trial of four treatment durations was performed with two rabbits in each group. The right nasal cavity of each rabbit served as the internal control and was not treated. The left nasal cavity received the manuka honey irrigation solution once daily. Groups 1–3 were treated for 3, 7, and 14 consecutive days, respectively, and euthanized the morning after the last treatment. Group 4 was treated for 14 consecutive days followed by a 14-day washout period and then euthanized the following morning (Fig. 1). The nasal respiratory mucosa was immediately harvested after death.
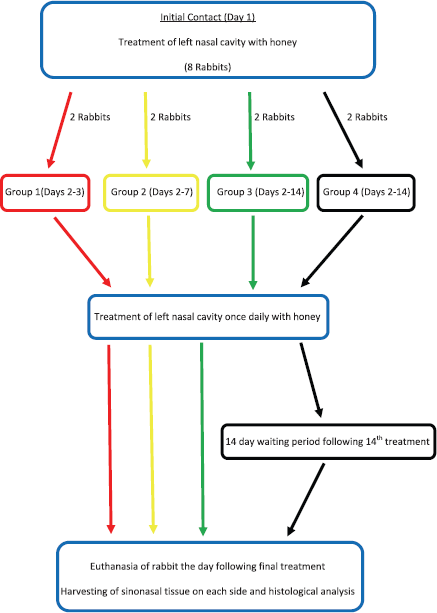
Experimental flowchart.
Mucosal Preparation
Four-micrometer sections of formalin-fixed, paraffin-embedded tissue were stained with hematoxylin phloxine saffron (HPS) stain and periodic acid–Schiff (PAS), and an immunohistochemical reaction for Ki67 was performed using monoclonal mouse anti-human antibody (Dakocytomation, Carpinteria, CA) with antigen retrieval done at a pH of 6.0 using a dilution of 1/100. Sections stained with HPS were placed onto regular slides and those stained with PAS and Ki67 were placed onto positively charged slides.
The HPS- and PAS-stained slides were then examined by a respiratory pathologist for the presence or absence of the following histological features associated with inflammation and tissue damage in both the control and the treatment groups: erosion, necrosis/apoptosis, overt regenerative epithelial hyperplasia, inflammatory infiltrate, edema, vascular congestion, altered pattern of mucin production by surface epithelium or the submucosal glands (PAS stain), and altered pattern of mucin production by the submucosal glands (PAS stain).
Tissue stained with Ki67 were analyzed by counting the number of positive-staining nuclei over 2 linear mm of epithelium with the help of an eyepiece for both the olfactory and the respiratory epithelium. Results of Ki67 staining were analyzed with a paired t-test for both the respiratory and the olfactory epithelium. A small fragment of freshly harvested tissue from rabbits 7 and 8 was fixed in glutaraldehyde, and along with a sample from the paraffin block of rabbit 5, they were postfixed in osmium tetroxide and epon-embedded for transmission electron microscopy (TEM) thin sections.
Cilia Motility Examination
The effect of a 33% manuka honey solution on ciliary motility was examined. Its effect on cilial beat frequency could not be determined; however, an estimate of its effect by visual observation with light microscopy was attained. Using a previously published technique 4 without using centrifugation, light microscopy was used to observe the cilia motility of mouse tracheal mucosa. On harvesting fresh tracheal mouse mucosa, it was covered in either 0.9% saline or a 33% manuka honey solution and observed at 400× magnification with light microscopy. This was done twice using two different fresh mouse tracheal mucosa samples.
Results
Light Microscopy—Morphological Analysis
The morphological evaluation did not show any histological evidence of epithelial damage. The epithelium was intact and the lining cells presented normal-appearing cilia/villi (Fig. 2). The PAS stain did not show any change in the pattern of mucin production by either the surface epithelium or the submucosal glands (Fig. 3). Because of the lack of histological evidence of mucosal injury as determined by light microscopy, further mucosal assessment with Ki-67 staining, TEM, and ciliary motility were then undertaken to assess for the presence of imperceptible damage.
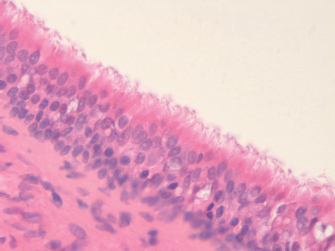
Photomicrograph showing normal epithelial histology and cilia (600× magnification, hematoxylin phloxine saffron [HPS] stain).
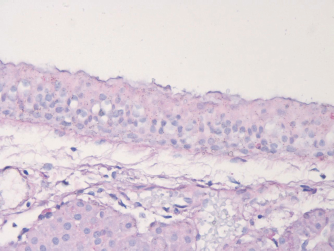
Photomicrograph showing normal histology (400× magnification, periodic acid—Schiff [PAS] stain).
Light Microscopy—Immunohistochemical Analysis
The olfactory epithelium presented positive nuclei from the base to the top, but most of the proliferating cells were at the base. The nasal epithelium usually presented proliferating cells at the base, with only five cases presenting nuclei at the top (two control/three treatment). The number of positive nuclei by group and type of epithelium is depicted in Fig. 4. There was no significant difference identified between the control and treated sides of the respiratory epithelium (p = 0.63); however, there was a statistically significant difference found for the olfactory epithelium between control and treated sides (p = 0.009).
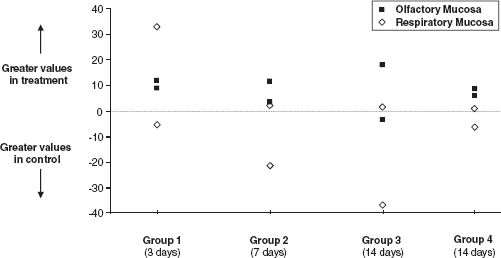
Graphical representation of values from the Ki67 staining for treated and control mucosa.
Transmission Electron Microscopy
Visual analysis of the TEM images from the mucosa of rabbits 5, 7, and 8 did not reveal evidence of epithelial damage (Fig. 5). The epithelium was intact and the lining cells presented normal-appearing cilia. There were no abnormalities in the cilial ultrastructure identified in any of the samples.
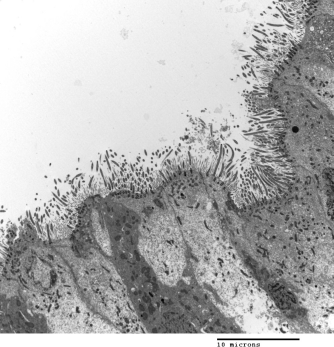
Transmission electron microscopy image showing normal mucosal ultrastructure (3000× magnification).
Ciliary Motility
Each of the samples attained from the trachea of the two mice allowed for the examination of ciliary motility. Both the manuka honey and the saline-treated mucosa from both mice showed an organized ciliary beat that was present for nearly 5 minutes. No differences between the samples treated with manuka honey or saline could be identified.
Discussion
CRS is a disease that is multifactorial in etiology. However, bacteria can commonly be identified in at least 50% of patient samples. A recent prospective study of >150 consecutive CRS patients with mucopurulence identified a nearly 30% rate of bacteria with biofilm-forming capacity as assessed by an in vitro biofilm formation assay. 5 For the most part, this form of bacterial infection has likewise been shown to have a deleterious effect on clinical prognosis when identified in a patient.6,7
Patients with CRS are often treated with systemic antibiotics in an effort to eradicate bacteria that are contributing to inflammation. However, in a patient who has undergone endoscopic sinus surgery, a topical therapy would be preferred because it may avoid the numerous possible side effects associated with systemic therapy while targeting the site of disease. Manuka honey may offer such an alternative. Given manuka honey has been shown to be effective against two common biofilm-producing organisms that occur in CRS, we sought to examine whether topically applied manuka honey would cause histological evidence of injury to respiratory mucosa.
In this study, we used a concentration of manuka honey that has been shown to be cidal in vitro against bacterial biofilms. 3 Various lengths of treatment time were used to assess differences in outcome because if this therapy is to be applied clinically, it is currently unknown for how long a patient would need to be treated. Thus, knowing if there is detriment through repeated exposure has clinical relevance. A potential weakness of the study is that greater concentrations of manuka honey were not tested because it is still unknown whether higher concentrations may be required for the eradication of other bacteria.
Nonetheless, regardless of treatment time in this study, there was no significant histological evidence of detrimental effects from the topical application of manuka honey to respiratory mucosa. However, the analysis for the olfactory mucosa revealed an unexpected difference between the treated and the control sides for positivity with the Ki67 stain. The significance of this finding is questioned given that the remainder of the histological analysis did not reveal evidence of regenerative activity or inflammation due to epithelial injury. However, consideration to monitoring for changes in olfactory function should be performed if this product is used in humans. Despite this one finding, given the lack of histological injury to respiratory mucosa from the tested manuka honey solution, this product may have the potential to be used in patients with CRS and proven bacterial infection, either in the planktonic or in the biofilm form.
Footnotes
Acknowledgments
The authors thank Steve Doucette, M.Sc., Ottawa Health Research Institute (OHRI) for preparing the statistical analyses; Kawal Deogun, M.L.T., Children's Hospital of Eastern Ontario (CHEO) for the preparation of the slides for light microscopy; and Jeff McClintock, M.Sc., Children's Hospital of Eastern Ontario (CHEO) for the TEM images.