
Abstract
Background
Although biofilms have been implicated in the pathogenesis of chronic rhinosinusitis (CRS), there is little evidence that their presence or absence has any effect on the outcomes of endoscopic sinus surgery (ESS). The aim of this study was to investigate the effect of biofilms on postsurgical outcomes after ESS.
Methods
A prospective, blinded study of 51 consecutive patients undergoing ESS for CRS was conducted. Preoperatively, patients assessed their symptoms using internationally accepted standardized symptom scoring systems and quality-of-life (QOL) measures, i.e., the 10-point Visual Analog Scale (VAS), Sino-Nasal-Outcome-Test 20, and global severity of CRS. Their sinonasal mucosa was graded using the Lund-Kennedy scale and the extent of radiological disease on computed tomography scans was scored using the Lund-McKay scale. Random sinonasal tissue samples were assessed for biofilm presence using confocal laser microscopy. At each postoperative visit, patients reassessed their sinus symptoms and completed QOL measures. Postsurgical state of their sinonasal mucosa was graded endoscopically.
Results
Bacterial biofilms were found in 36 of 51 (71%) CRS patients. Patients with biofilms presented with significantly worse preoperative radiology and nasendoscopy scores (p = 0.003 and 0.01, respectively). After a median follow-up period of 16 months postsurgery, biofilm-positive patients had statistically worse sinus symptoms (VAS, p = 0.002) and worse nasendoscopy scores (p = 0.026). They also required extra postoperative visits and multiple antibiotic treatments deviating from the standard postoperative care required by biofilm-negative patients.
Conclusion
This study has shown that patients with biofilms have more severe disease preoperatively and persistence of postoperative symptoms, ongoing mucosal inflammation, and infections. This study strengthens the evidence for the role that biofilms may play in recalcitrant CRS.
Keywords
Bendouah et al.16,17 detected the biofilm-forming capacity of bacteria recovered from individuals with CRS and correlated that with a dichotomous postsurgical outcome of favorable or unfavorable as assessed by questionnaire and endoscopy 1 year post–endoscopic sinus surgery (ESS) procedure. They found that Pseudomonas aeruginosa and Staphylococcus aureus biofilms were associated with a more unfavorable surgical outcome. A retrospective analysis conducted in our department on 40 CRS patients found that patients with biofilms were more likely to have symptoms and show evidence of ongoing mucosal inflammation after sinus surgery. 18 It is important to note, however, that this study used nonvalidated symptom scoring methods and nominal reporting of postoperative symptom and endoscopic outcomes.
The inherent limitations of these studies make it difficult to conclusively document the adverse affect of biofilms on postsurgical outcomes. To address these limitations, we conducted a prospective, blinded study of CRS patients undergoing ESS using internationally accepted, standardized symptom, radiological and endoscopic scoring systems, aiming to analyze the impact that biofilms have on postsurgical outcomes.
Methods
Study Design
This was a prospective, blinded study of patients undergoing ESS for CRS in the tertiary rhinology clinic of the senior author (P.J.W.) in Adelaide, South Australia. With appropriate approval from the Human Ethics Committee, 51 consecutive patients with evidence of CRS, who gave informed consent to participate, were recruited for the study. The diagnosis of CRS was made as per the Rhinosinusitis Task Force definition for the disease. 19 Patients <18 years of age and those with immunocompromised conditions were excluded from the study.
Preoperative Data Collection
Preoperatively, demographic and clinical information including age, sex, medical and surgical histories, allergies, and previous ESS procedures were recorded. Patients were asked to complete questionnaires to document the severity of their rhinosinusitis before surgery. Using the widely accepted and validated 10-point Visual Analog Scale (VAS) scoring system, 19 the patients graded their symptoms of nasal congestion/obstruction, nasal discharge, alteration in sense of smell, headache, facial pain/pressure, and sneezing, as well as their combined symptoms’ score. They assessed the effect of sinusitis on their quality of life (QOL) using the Sino-Nasal-Outcome-Test 20 (SNOT-20) symptom inventory and the “Global Assessment of Rhinosinusitis Symptom severity” 7-point VAS (GARS).19,20 The state of the patient's sinonasal mucosa was graded by the treating surgeon (P.J.W.) using the Kennedy-Lund scoring system. 21 All patients underwent preoperative computerized tomography (CT) scanning, which was scored using Lund-Mackay scoring system. 22
Perioperative Data Collection
All of the endoscopic sinus procedures were performed by the senior surgeon (P.J.W.) to ensure that all patients received the same standard of surgical care. Depending on the extent of their disease the patients underwent either a mini-functional ESS (maxillary antrostomy and ethmoidectomy) or a full-FESS (complete sphenoethmoidectomy and frontal sinusotomy). Intraoperative findings such as the presence/absence of pus, polyps, and eosinophilic mucin were documented. Swabs were sent from the sinonasal areas of all patients for microscopic examination and culture, for isolation of possible bacteria or fungi. Two random mucosal samples of ∼5–10 mm2 were taken from either the osteomeatal region or the sinuses of each patient. They were stored immediately in Dulbecco's modified Eagle medium (Gibco, Invitrogen Corp., Grand Island, NY) and transported on ice to the Adelaide Microscopy for analysis on the same day. Posterior ethmoid tissue from five patients undergoing transsphenoidal procedures for benign pituitary tumors was used as controls. None of these patients had clinical or radiological evidence of CRS and their samples were stored and processed in identical fashion to that of the patient group.
Tissue Preparation and Analysis
This was performed by an independent investigator (D.S.) who was not present during the procedure and thus was blinded to the operative findings of the surgeon. The specimens were processed and analyzed within 2 hours of collection using the Baclight stain-confocal scanning laser microscopy (CSLM) protocol described earlier. 23 As per the protocol, each tissue sample was washed thoroughly in three separate beakers of sterile Milli-Q (MQ) water to remove any planktonic bacteria. The sample was then immersed in 1 mL of sterile MQ water, to which 1.5-μL aliquots of component A (syto9) and component B (propidium iodide) of BacLight LIVE/DEAD kit (Invitrogen, Molecular Probes, Eugene, OR) are added. With this combination of stains, cells/bacteria with intact cell membranes stain fluorescent green, whereas those with damaged membranes stain fluorescent red. After incubation in darkness at room temperature for 15 minutes, each sample was rinsed in sterile MQ water to remove excess stain. The specimens were mounted on coverslips for analysis with a Leica TCS SP5 confocal scanning laser microscope (Leica Microsystems, Wetzlar, Germany). The entire area of the specimen was scanned for evidence of biofilm structures using a water immersion lens at both 20× and 63 × magnification. The entire thickness of each sample was imaged by means of z-stacks with slices at 0.5 μm. The recorded images were reviewed by three independent investigators (D.S., A.P., and A.F.) who were blinded to the clinical profile and surgical findings related to each patient.
Postoperative Data Collection
All patients received standardized postoperative care and follow-up by the senior surgeon (P.J.W.), who was blinded to the biofilm status of the patients. As per the standard postoperative care, the patients were assessed at 2 and 6 weeks and 6 and 12 months and 6 monthly intervals thereafter. Any other postoperative visit as required for the patient apart from the aforementioned standard care was also recorded. On each of these visits, the patients graded their symptoms and QOL on the same scales as they had done preoperatively (i.e., VAS, SNOT-20, and GARS). The patients also remained blinded to their biofilm results throughout the follow-up period. Their sinonasal mucosa was graded endoscopically for postsurgical changes at each visit, by the same surgeon (P.J.W.), who remained blinded to the biofilm status of the patient. Any change from the standardized postoperative surgical care was recorded.
Statistical Analysis
Statistical analysis was performed using GraphPad Prism 5.0 software (GraphPad Software, San Diego, CA). All data were considered nonparametric after normality tests were applied to assess if it followed a Gaussian distribution. For all statistical tests used, p = 0.05 was considered significant. Differences were analyzed using the following statistical tests: a chi-square or Fisher's exact test for dichotomous data, the Mann-Whitney U test for two-way independent samples. Interrater variability between the three image observers was assessed using Fleiss’ κ-statistic, calculated using Minitab 15 Statistical Software (Minitab, Inc., State College, PA).
Results
Demographic Factors
Of the 51 patients recruited for the study, 26 were men (50.9%) and 25 were women (49.01%). The median age of the population under study was 52 years with an interquartile range of 38–61 years. About two-thirds of the study population had suffered with sinusitis for >6 years and a similar proportion reported that they had symptoms “all the time.” Twenty-seven of the 51 patients had coexisting asthma, and 7 showed aspirin sensitivity. More than ⅔ of the study population were nonsmokers. Only 2 of the 51 subjects gave a current history of smoking and 14 had ceased smoking at different periods in the past.
At the completion of the study, the patients had a median follow-up of 16 months (interquartile range, 13–18 months). Fifteen patients had completed an 18-month postoperative period, 24 had completed 12 months, and 10 had completed a 6-month postoperative follow-up. Two patients were lost to follow-up in the early postoperative period of their follow-up.
Biofilm Status
Thirty-six of the 51 (70%) CRS patients enrolled in the study showed evidence of biofilms on CSLM. Using the Baclight–CSLM protocol, biofilms were identified as clusters and towers of immobile, irreversibly attached, intensely fluorescing, live green bacteria (∼0.5–2 μm diameter). None of the non-CRS control samples from the endoscopic endonasal pituitary surgeries showed the presence of biofilms. Calculation of Fleiss’ κ-statistic for interrater variability yielded a κ-value of 0.8274, which is deemed to represent almost perfect agreement. 24
Preoperative Data Analysis
Preoperative Severity of CRS
The preoperative measures of severity of sinusitis for the patients who showed biofilms (biofilm positive) are compared with those of patients who did not show any biofilms (biofilm negative) in Table 1. The subjective measures (total VAS of symptoms, total SNOT-20 score, and GARS 7-point VAS) did not differ significantly between the two groups, whereas the objective measures showed statistically significant differences, i.e., radiology scores, p = 0.003, and nasendoscopy scores, p = 0.01 (Mann-Whitney U test).
Preoperative measures of severity of sinusitis
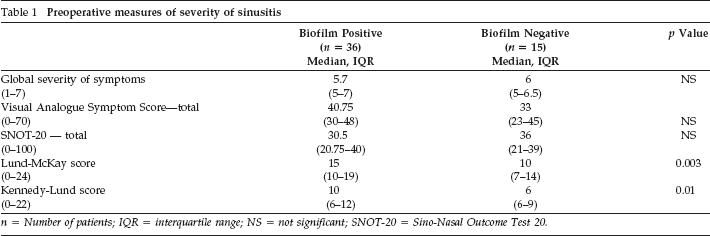
n = Number of patients; IQR = interquartile range; NS = not significant; SNOT-20 = Sino-Nasal Outcome Test 20.
Previous Surgery
Thirty-one (61%) of the patients enrolled in the study had undergone at least one previous ESS procedure. Of these 31 patients with revision surgeries, 23 (75%) showed evidence of biofilm and 8 (25%) did not. Twenty-three of the 36 (64%) biofilm-positive subjects had prior sinus surgeries, the average number of prior procedures being 1.9 (range, 0–7). Eight of 15 (53.3%) biofilm-negative patients had prior surgery, with mean value of procedures at 0.9 (range, 0–4). However, this difference in the number of prior surgical procedures between biofilm-positive and biofilm-negative patients was not statistically significant (p = 0.54, Fisher's exact test).
Nasal Polyps
Twenty-five of 51 patients had nasal polyps and 21(84%) of these patients showed biofilms. Twenty-one of 36 (58%) of the biofilm-positive patients had nasal polyps, and 4 of 15 (26.7%) of the biofilm-negative patients had polyps (p = 0.06, Fisher's exact test).
Perioperative Data Analysis
Type of Procedure
Among the 15 biofilm-negative patients, 5 underwent a mini-FESS, 10 required a full-FESS, and 2 of these 10 needed a modified endoscopic Lothrop procedure (MELP, frontal drillout). Only 3 of the 36 biofilm-positive patients underwent a mini-FESS, and 33 required a full-FESS. Twelve of these 33 patients also underwent an MELP, and out of these, 1 was a revision MELP. This difference in the extent of ESS (mini-FESS versus full-FESS) between the two groups was statistically significant (p = 0.04, Fishers test).
Perioperative Microbiology
Intraoperative swabs cultured bacteria in 25 of 36 (69.4%) biofilm-positive patients. Only 3 of 15 (20%) biofilm-negative patients showed positive bacterial cultures. This difference in perioperative bacterial cultures was statistically significant (p = 0.002, Fisher's exact test). S. aureus was isolated from 13 of the 25 biofilm-positive cases, followed by 5 cultures of Streptococcus pneumoniae, 4 of P. aeruginosa, 2 of Escherichia coli, and one each of Klebsiella, Proteus, Moraxella and coagulase-negative Staphylococcus. More than one bacterium was cultured in seven of the biofilm-positive cases. Among the three isolates from biofilm-negative subjects two were that of S. aureus and one was S. pneumoniae.
Fungus was isolated from 6 of the 36 biofilm-positive subjects by either staining or culture, but no fungus was isolated from any of the biofilm-negative patients. Three isolates were of Aspergillus, two were of Penicillium, and one was of Biopolaris. Eosinophilic mucin was identified on histology in 20 of the 51 (39.21%) patients. Eighty percent of these eosinophilic mucin–positive cases showed biofilms. The number of biofilm-positive patients (16 of 36) showing eosinophilic mucin was not significantly different from the number of biofilm-negative patients (4 of 15) showing eosinophilic mucin (p = 0.35, Fisher's exact test).
Postoperative Results
Follow-Up Visits
As a part of routine postsurgical care, the patients were assessed at 2 and 6 weeks, 6 months, and at 6 monthly intervals thereafter; however, during the period of the study it was found that 29 of 51 (57%) of the patients required extra visits to the rhinology clinic. Out of these 29 patients, 27 were biofilm positive. Thus, 75% (27 of 36) of the biofilm-positive patients required extra consults, which was statistically very significant (p < 0.001), when compared with only 13.3% (2 of 15) of the biofilm-negative patients requiring extra consults. The average number of visits that the patients had to come for is described in Fig. 1. Biofilm-positive patients had a mean of 1.9 ± 1.5 extra visits, which was significantly more (p < 0.001) than the 0.17 ± 0.03 extra visits required by biofilm-negative patients.
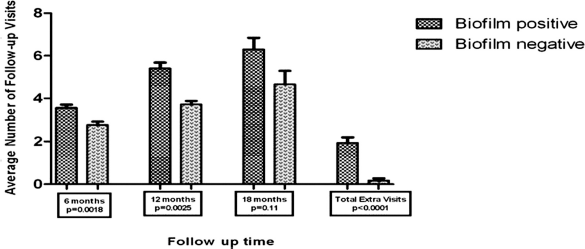
Average number of follow-up visits at 6, 12, 18 months follow-up.
Patients Lost to Follow-Up
Two of the patients were last assessed at 6 weeks postoperatively and did not return for any further follow-up visits. One of them had undergone a min-FESS and the other had a full-FESS. They were both biofilm negative and showed a nasendoscopy score of 0 on the 6-week follow-up visit.
Symptom Outcomes
Among the biofilm-positive patients, the median total sinus symptom score of 40.5 preoperatively showed some initial improvement to 19 (interquartile range, 14–29) at 2 weeks and 14 (9–25) at 6 weeks; however, subsequently, it started worsening to 17.8 (11–28) at 6 months and 17 (8–34) at 12 months. The biofilm-negative group had median total sinus symptom scores of 18.5 (9.7–32) at 2 weeks, 7.5 (5.5–11.5) at 6 weeks, 6 (5–13.75) at 6 months, 9 (6–17.5) at 12 months, and 6.5 (4–9) at 18 months. The effect of biofilms on these values was statistically very significant (p = 0.002), with specific p values at 6, 12, and 18 months being 0.006, 0.17, and 0.3, respectively (Mann-Whitney test; Fig. 2).
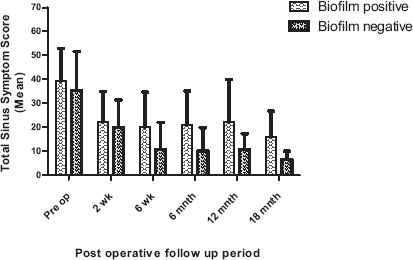
Postoperative symptoms visual analog scale total score at different follow-up periods.
Nasendoscopy Outcomes
The biofilm-positive patients had median (with interquartile range) Kennedy-Lund scores of 4 (3–7) at 2 weeks, 4 (2–10) at 6 weeks, 3 (2–7) at 6 months, 6 (2–10) at 12 months, and 8 (0.5–14) at 18 months. At the same follow-up period biofilm-negative patients had median nasendoscopy scores of 2.5 (0.75–4), 0 (0–2), 0 (0–2.25), 0 (0–3.8), and 0.5 (0–1). On comparing the two groups (Fig. 3) the difference was statistically significant (p = 0.026, Mann Whitney U test).
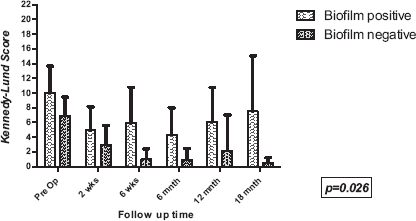
Comparision of Kennedy-Lund nasendosocpy scores between biofilm-positive and biofilm-negative patients during the follow-up.
QOL Outcomes
The median global assessment of severity of CRS score and median total SNOT-20 scores for the biofilm-positive and biofilm-negative patients are detailed in Table 2. The QOL measures were also statistically significant between the two groups, with the scores slowly creeping toward the preoperative baseline in the follow-up period.
Quality of life outcomes

CRS = chronic rhinosinusitis; SNOT-20 = Sino-Nasal-Outcome-Test 20.
Postoperative Bacteriology
Twenty-six of 51 patients showed evidence of mucopus on endoscopy during the postsurgery follow-up. A swab taken for microbiology evaluation from them and 25 of 36 (70%) biofilm-positive cases cultured bacteria postoperatively when compared with only 1 of 15 biofilm-negative patients (p < 0.0001, Fisher's exact test). Fourteen of these 25 biofilm-positive cases cultured bacteria on more than one follow-up visit. S. aureus was the most common bacteria isolated, accounting for >50% of the isolates, followed by P. aeruginosa, S. pneumoniae, Haemophilus influenza, Corynebacterium, and E. coli.
Discussion
This study is a prospective analysis of the impact of biofilms on the postsurgical outcomes of a consecutive cohort of patients and it has shown that biofilm-positive patients have worse objective disease and have poorer postoperative outcomes than biofilm-negative patients. Although the pathophysiology of CRS is thought to be multifactorial, the presence of bioflims may well contribute to the ongoing inflammation seen in the recalcitrant subgroup of CRS patients. This subgroup of patients continues to have persistent sinonasal inflammation and recurrent acute exacerbrations, despite long-term culture-directed antibiotic therapy and well-performed sinus surgery. Over the past 5 years with the detection of biofilms in CRS patients, it has been speculated that these structures may be responsible for propogating the recalcitrant and chronic nature of CRS.4,8,25,26 To date, however, the studies confirming this have been limited by their in vitro and retrospective design.17,18
Biofilms were detected in 71% of this CRS population using the Baclight-CSLM protocol standardized in our department. 23 The preoperative subjective measures assessing the sinusitis symptoms and QOL of the patients in the study did not differ significantly between the biofilm-positive and biofilm-negative groups. The biofilm-positive group had significantly worse Lund-Mckay radiology and Kennedy-Lund nasendoscopy scores when compared with the biofilm-negative group, indicative of a more severe preoperative disease in those patients.
The biofilm-positive group showed a tendency to have undergone more numbers of previous sinus surgeries, and almost 75% of the patients who were undergoing revision sinus surgeries showed evidence of biofilms. This supports the hypothesis that biofilms may play a role in perpetuating the recalcitrant nature of chronic sinusitis, with the patients requiring repeated surgical interventions despite maximal medical management. Additionally, patients with biofilm showed a tendency to undergo more extensive procedures, i.e., 92% underwent a full-FESS and 33% required a frontal drillout procedure, whereas only 67% of the biofilm-negative patients underwent a full-FESS and only 13% required a drillout procedure. This was once again reflecting the more severe disease seen in patients with biofilms, necessitating a more extensive surgical intervention.
More than one-half of the patients in our study required extra visits other than the standard care, commonly at 8–10 weeks, 12–14 weeks, and 8–9 months postsurgery. These extra rhinology consults occurred as a result of the patients developing sinus symptoms requiring medical opinion in between the regular visits or because of ongoing inflammation in the sinonasal region prompting the surgeon to review them at more frequent intervals. Throughout these consults both the surgeon and the patient were blinded to the patient's biofilm status. An impressive 93% of the patients who required these extra consults were biofilm positive. The fact that 75% of the biofilm-positive subjects in the study came for extra consults reflects the ongoing disease in these patients, which, in turn, resulted in increased medical attention. It led to an increased burden on the health care system, extra financial costs to the patient, and work days lost.
Among the biofilm-positive patients, the symptom scores and QOL measures (Fig. 2) showed initial improvement until the ∼6-month follow-up, but thereafter a slow deterioration was noted. The patients without biofilms, however, have shown a continued improvement in these measures and stabilization in symptoms by 12–18 months postsurgery. This statistically significant poor postoperative symptom outcome in patients with biofilms indicates that this subgroup of CRS patients continues to have an ongoing relapsing and recalcitrant course. We saw a significant correlation between the presence of biofilms and endoscopic evidence of ongoing mucosal inflammation. The patients with biofilms had ongoing infective episodes and ensuing inflammation resulting in mucosal edema, discharge, crusts, and even early polyp recurrences in a few cases.
Residual biofilms after surgery may reseed the regenerating epithelium and serve as a nidus for further biofilm formation. Once established, bacteria within a biofilm have altered phenotype/genotypes, making them extremely resistant to the host immune system and antibiotics. The biofilm may act as a stimulus for ongoing inflammatory response, as well as releasing planktonic forms of bacteria periodically as a part of its life cycle, leading to acute exacerbations on top of the chronic process. The high rates of intraoperative and postoperative bacteria cultured from the biofilm-positive group in our study may reflect this periodic planktonic transformation of biofilm bacteria. Fifty percent of the biofilm-positive patients cultured bacteria from both intraoperative and postoperative swabs, and ∼60% of these grew the same bacteria on multiple different occasions. S. aureus was the most common bacterial isolate followed by S. pneumoniae, P. aeruginosa, and H. influenzae. This was consistent with biofilm literature that suggests that although bacteria existing in biofilms are difficult to culture because of their lower growth and metabolic rates, biofilms may function as a source of planktonic cells through high cell yield and detachment.27,28
Conclusion
Patients who have biofilms on their sinonasal mucosa tend to have a greater severity of disease preoperatively and continue to have persistent and more severe disease postsurgery with ongoing mucosal inflammation and recurrent infections. This study supports a role for biofilms in perpetuating the chronic and recalcitrant nature of CRS.