
Abstract
Background
Chronic rhinosinusitis (CRS) is a common disease with a complex pathophysiology involving a microbial component. Culture-independent molecular analysis represents a promising new approach to clarify the microbiology of CRS, but standardized, optimized sampling methods still have not been defined. This study was designed to compare nucleic acid extraction rates and recovery of bacteria for two methods of sampling the maxillary sinus, mucosal biopsy, and brushing.
Methods
Samples were obtained from 20 patients undergoing maxillary sinus surgery. Total extracted nucleic acid concentration and bacterial burden were compared between sample types.
Results
Total nucleic acid concentration varied across patients. No statistically significant difference in mean total DNA concentration from mucosal biopsy specimens or brushings was observed. However, compared with biopsy specimens, brush samples possessed a significant (p < 0.035) increase in bacterial copy number.
Conclusion
Endoscopically directed mucosal brushings of the maxillary sinus provide equivalent concentrations of total DNA to mucosal biopsy specimens but possess greater concentrations of bacterial DNA, likely because of the greater surface area sampled by this method. Given the additional advantage of lower risk associated with obtaining brush samples, we suggest they represent the preferred sampling method for future genomic sinus studies.
Keywords
Methods
Sample Collection
Approval was obtained from the University of California, San Francisco, Committee on Human Research. Consecutive consenting adults scheduled to undergo surgery entering the maxillary sinus were recruited from the Department of Otolaryngology–Head and Neck Surgery and the Department of Oral and Maxillofacial Surgery. Inclusion criteria were age of ≥18 years, with or without CRS. Exclusion criteria were a history of cystic fibrosis or primary ciliary dyskinesia. All patients completed a Sino-Nasal Outcome Test 20 survey (SNOT-20). 3 Lund-Mackay scores were calculated for all patients with preoperative computed tomography (CT) scans. 4
One maxillary sinus was sampled in each patient. Brushings were obtained using steam-sterilized Interdental Brushes (Acclean; Henry Schein, Inc., Melville, NY), guided into the maxillary sinus using blunt, up-angled forceps and a rigid Hopkins rod during endoscopic cases and using curved Kelly forceps during open cases. Two brushings were performed and immediately placed in 1 mL of RNALater (Qiagen, Inc., Valencia, CA) in an RNase/DNAse-free sterile BD Falcon tube (Thermo Fisher Scientific, Inc., Waltham, MA). Biopsy specimens of mucosa from the medial or posterior maxillary sinus walls were obtained using through-biting forceps and also were immediately placed in 1 mL of RNALater at room temperature in a Falcon tube. Samples were refrigerated at 4°C overnight before processing.
Nucleic Acid Extraction and Q-PCR Analysis
DNA was extracted using a combination of bead beating and the AllPrep kit (Qiagen, Inc.). Briefly, samples were transferred directly from the collection tube to Lysis Matrix B tubes (Qbiogene, Carlsbad, CA) using sterile forceps. The original collection tubes were then centrifuged at top speed for 10 minutes; RNALater was carefully removed and the remaining material was resuspended in 600 μL of buffer RLT from the AllPrep kit. This solution was added to respective brushes or biopsy specimens in lysing matrix B tubes before bead beating at 5.5 m s–1, for 30 seconds. Tubes were centrifuged at 2000 rpm and the supernatant was transferred to the DNA column of the AllPrep kit. The remainder of the extraction was performed as per the manufacturer's instructions. DNA concentrations were measured using a Nanodrop spectrophotometer (Thermo Fisher Scientific, Inc.). Q-PCR was performed on brushing samples using the primers 16SF 5′-ACTCCTACGGGAGGCAGCAG-3′ and 16SR 5′-TTACCGCGGCTGCTGG-3′, in a standard 40-cycle reaction, using an annealing temperature of 55°C.
Statistical Analysis
Paired t-test was used to determine statistically significant differences between brushing and biopsy samples using Graphpad. 5
Results
Twenty patients, average age 46 years (range, 18–73 years), 13 male and 7 female patients, were enrolled. Patient details are provided in Table 1. Samples were obtained from all patients, 13 of which were collected endoscopically and 7 through open surgical procedures. Total extracted DNA varied across patients but was typically higher for brushings (108.31 ± 151.13 ng μL–1) than for biopsy specimens (84.63 ± 93.73 ng μL–1). However, this difference was not statistically significant by paired t-test (p < 0.39; Table 2). There were also no statistically significant differences in total DNA yield between endoscopic and open approaches for brush samples (p < 0.15) or mucosal biopsy specimens (p < 0.36). In endoscopic cases alone (13 total), there were no significant differences in yield between patients with or without CRS sampled by brushings (p < 0.23) or biopsy specimens (p < 0.72). Among patients with CRS, there was no correlation between disease severity as assessed by SNOT-20 or Lund-Mackay CT score and either the total DNA yields from brushings or mucosal biopsy.
Patient characteristics and surgical procedures
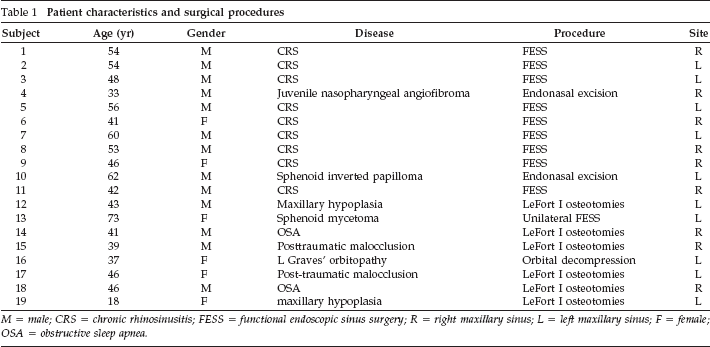
M = male; CRS = chronic rhinosinusitis; FESS = functional endoscopic sinus surgery; R = right maxillary sinus; L = left maxillary sinus; F = female; OSA = obstructive sleep apnea.
Total DNA concentration and bacterial copy number for samples in this study
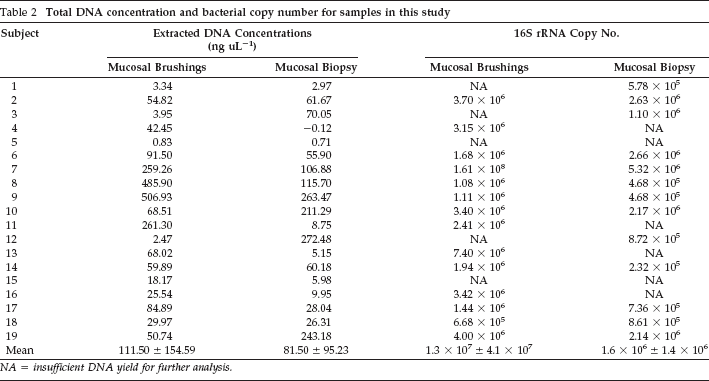
NA = insufficient DNA yield for further analysis.
A 16S rRNA Q-PCR reaction was performed for each sample to determine if bacterial burden differed between sample types. Brush samples possessed significantly higher bacterial copy number compared with biopsy specimens (p < 0.035). No significant correlation between bioburden and SNOT-20 score was exhibited, suggesting bacterial community composition rather than load may play an important role in disease severity.
Discussion
CRS accounts for a significant number of primary care visits, resulting in direct and indirect medical costs exceeding $2.4 billion annually. 6 Antibiotics, often broad-spectrum and empiric, are a major component of both therapy and overall cost. 2 A culture-independent understanding of the microbiology of CRS is necessary to refine therapy and thereby reduce the overall burden on society.
Gene expression microarrays have gained popularity in the study of CRS and have been used to measure human mucosal gene expression in specific disease states.7–10 PCR detection of fungi in patients with and without CRS has also previously been performed. 11 However, to date, culture-independent approaches have not been used to comprehensively describe the microbiology of CRS. To facilitate such approaches, the current study was designed to compare sinus-sampling approaches in an attempt to determine the optimal sampling strategy for future microbiological studies.
Our data show great variability in the total concentration of extracted DNA irrespective of the sampling method. This likely reflects variability in the microbial communities colonizing these niches as has previously been reported for other mucosal surfaces. 12 This suggests that multiple samples should be collected from individuals to ensure availability of sufficient material for analysis. Although the mean DNA concentration from biopsy samples was typically lower than that from brushings, the difference was not statistically significant. However, we have previously found that mucosal airway brushings produce a higher yield of nucleic acid than mucosal biopsy in bronchoscopically derived clinical bronchopulmonary specimens (Huang et al., unpublished data, 2010). Theoretically, brushings sample a broader surface area than a directed mucosal biopsy. The lack of a significantly higher DNA concentration from brushings appears to be caused by the high variability in DNA concentrations obtained across samples. This may reflect “patchiness” of colonization in the sinuses or operator variability in sample collection or processing.
Regardless, the majority of samples extracted provided sufficient genomic material for downstream molecular assays such as Q-PCR or microarray-based microbiological studies. This is encouraging when compared with a recent study, in which >80% of healthy maxillary sinuses examined with saline lavage and standard culture methods did not yield detectable bacteria. 13 Surgical approach and presence or absence of CRS, as well as CRS severity (as assessed by SNOT-20 and Lund-Mackay CT) scores exhibited no statistically significant effect on the final DNA yield or bacterial burden. These data suggest that disease severity is more likely to be related to the presence of specific types of microbes rather than the microbial burden per se. Comparative analysis of both types of samples showed that brushing samples possessed significantly greater bacterial burden compared with biopsy samples, likely because of the greater surface area samples by this approach. Given this increased recovery of bacterial burden and the lower risk associated with mucosal brushings, they are therefore the preferred method of sampling the maxillary sinus for culture-independent microbiological analyses.
Footnotes
Acknowledgment
The authors thank Homer Boushey, M.D., for initiating this collaborative study. They also thank Wendy Ma, B.S.; M. Anthony Pogrel, D.D.S., M.D.; Janice S. Lee, D.D.S., M.D., M.S.; Radhika Chigurupati, D.M.D.; Eric J. Kezirian, M.D.; Ivan H. El- Sayed, M.D.; and Jane T. Liu for their assistance with this study.