
Abstract
Background
Determination of predictive factors and specific values of olfactory function after endoscopic sinus surgery (ESS) using objective diagnostic methods may support consultation of respective patients. This study was designed to assess the longitudinal olfactory functional outcome after ESS in patients with severe chronic rhinosinusitis (CRS) with nasal polyposis, to evaluate associated clinical factors and to provide statistical models for prediction of olfactory recovery.
Methods
One hundred sixteen patients with nasal polyposis refractory to medical treatment underwent ESS. Olfactory testing was performed preoperatively and 1, 3, and 6 months after surgery using “Sniffin’ Sticks” (Burghardt, Wedel, Germany). Using multivariate linear and logistic regression analysis, statistical models were generated to predict (i) the 6th-month composite threshold-discrimination-identification (TDI) score and (ii) the probability of attaining normal olfaction at 6 months.
Results
A significant stepwise increment of all olfactory function indices was found over time. Factors influencing final olfactory recovery were patients’ age, duration of olfactory deficit, previous paranasal sinus surgery, and aspirin-exacerbated respiratory disease. The first model explained 70% of the observed variation in postoperative TDI scores. The second model correctly classified 76% of the patients.
Conclusion
A significant progressive improvement of olfaction for at least 6 months was observed after ESS. The statistical models developed may be useful for consultation of ESS candidates in clinical practice.
Keywords
Patients and Methods
In this prospective study 116 consecutive patients undergoing surgery for CRSwNP were included. In all patients findings of preoperative nasal endoscopy were recorded using Malm's grading system. 5 Patients suffered from severe CRSwNP and were classified as Malm's stage 3 (polyps reaching the floor of the nasal fossa). CT scans were graded according to the Lund-Mackay CT scoring system. 6 All patients had a total score of >16 (range, 17–24); there was bilateral ethmoid disease with involvement of 3 or more dependent sinuses and of the ostiomeatal complex.
Historical data of the patients used were age, gender, presence of allergic rhinitis, aspirin-exacerbated respiratory disease (AERD), prior sinus surgeries, smoking, duration of olfactory dysfunction, and presence of taste dysfunction. Twenty patients reported lack of flavor perception that was temporally associated with their olfactory loss.
In all patients, CRSwNP was refractory to maximal medical therapy (antibiotics, oral and nasal steroids). Patients with persistent CRSwNPs underwent ESS by a single surgeon, according to the Messerklinger technique, 7 with use of a microdebrider.
Postoperative care included multiple visits at the outpatient clinic where nasal endoscopy and toilette as needed were performed. All patients were asked to stop smoking and to rinse their nose with 0.9% sodium chloride solution and were prescribed nasal steroids for 6 months after surgery. All patients stopped smoking after surgery. The care of patients who participated in this study was approved by the local Institutional Review Board. All subjects were volunteers and had given their consent to participate in the study after having been extensively informed about the study's aim, design, and clinical implications. The investigations were performed in accordance with the principles of the Declaration of Helsinki/Hong Kong.
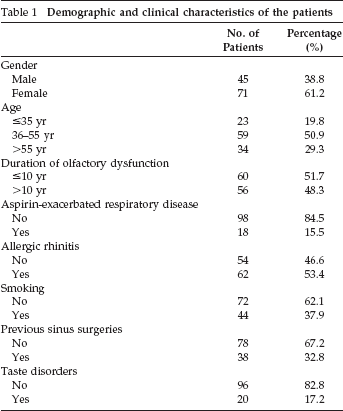
Demographic and clinical preoperative patient data are presented in Table 1. Olfactory tests were performed preoperatively and at 1, 3, and 6 months postoperatively bilaterally, using the “Sniffin’ Sticks” test package (Burghardt, Wedel, Germany) as described elsewhere in detail.8,9 The test battery included specific tests for odor threshold (OT), odor discrimination (OD), and odor identifications (OI).
Demographic and clinical characteristics of the patients
The obtained score at the end of each one of the three tests was an integral, ranging from 0 to 16. The scores of each one of the three tests were added to form the composite “threshold–discrimination–identification” (TDI) score,8,10 which ranged from 0 to 48, with values ≤15 considered consistent with anosmia, and values between 16 and 34.5 considered as hyposmia for the Greek population. 11
Statistical analysis of the data was performed using the Statistical Package for the Social Sciences, Version 11.0 (SPSS, Inc., Chicago, IL). The normality of continuous variables was tested with the Kolmogorov-Smirnov test. Repeated measures analysis of variance (ANOVA) was used to examine changes of indices of olfactory function; post hoc analysis was performed using Bonferroni's correction. One-way analysis of co-variance (ANCOVA) was performed to investigate the effect of the demographic and clinical characteristics of patients on olfactory function 6 months after surgery, adjusting for baseline scores. The marginal homogeneity test was used to determine changes of olfactory function from one measurement to another. The chi-square test was used to evaluate any potential association between patients’ demographic and clinical characteristics and the presence of normal olfactory function 6 months after surgery. Odds ratio with 95% confidence interval (CI) was estimated as the measure of association of patients’ characteristics with normal olfactory function. To assess the independent effect of patients’ characteristics on the TDI score and the presence of normal olfactory function 6 months after surgery, multivariate linear and logistic regression models were constructed, respectively. Statistical significance was considered for values of p < 0.05.
Results
Olfactory Function
The pre- and postoperative values of all olfactory indices are shown in Table 2 (see footnote * in body of Table 2). One-way repeated measures ANOVA showed significant stepwise increments of all indices over time (all p < 0.001). Post hoc analysis, using Bonferonni's adjustment, was performed next; OT, OD, OI, and TDI scores exhibited highly significant elevation (736.6, 77.7, 102.0, and 114.2% respectively; all p < 0.001) at the 1st postoperative month. Smaller but statistically significant improvements of these four indices were observed at 3 (29.7, 18.5, 15.6, and 19.0%; all p < 0.001) and 6 postoperative months (15.1, 10.8, 10.2, and 11.3%; all p < 0.001), compared with the previous measurement.
Olfactory function (mean values ± SD) of the patients who underwent endoscopic sinus surgery
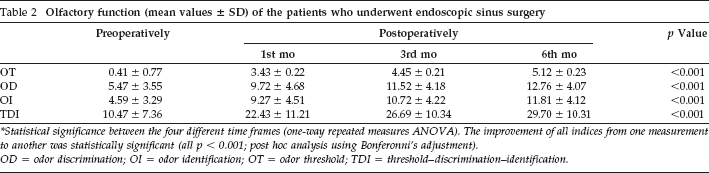
*Statistical significance between the four different timeframes (one-way repeated measures ANOVA). The improvement of all indices from one measurement to another was statistically significant (all p < 0.001; post hoc analysis using Bonferonni's adjustment).
OD = odor discrimination; OI = odor identification; OT = odor threshold; TDI = threshold–discrimination–identification.
After adjustment for the preoperative TDI score, univariate ANCOVA showed that the TDI score at 6 months was significantly lower in patients with long-standing (>10 years) olfactory loss (adjusted mean value ± SE; 27.16 ± 1.06 versus 32.06 ± 1.02, p = 0.002), AERD (21.25 ± 1.81 versus 31.24 ± 0.73, p < 0.001), and/or previous sinus surgery (25.29 ± 1.26 versus 31.84 ± 0.85, p < 0.001) in allergic patients (28.12 ± 1.02 versus 31.50 ± 1.10, p = 0.032) and in older patients (25.36 ± 1.26 in patients aged >55 years versus 30.63 ± 1.56 in patients aged ≤35 years and versus 31.83 ± 0.96 in patients aged 36–55 years; p = 0.010 and p < 0.001, respectively). The 6-month TDI score was independent of patients’ gender (p = 0.379), smoking (p = 0.626), and taste disorders (p = 0.262). The negative effect of older age (p < 0.001), longer duration of olfactory deficit (p = 0.017), presence of AERD (p < 0.001), and previous sinus surgery (p = 0.017) on 6th-month TDI remained significant in multivariate analysis. The regression equation, which describes quantitatively the relation of demographic and disease characteristics of the patients with severe CRSwNP who underwent ESS with the 6th postoperative month TDI score, is
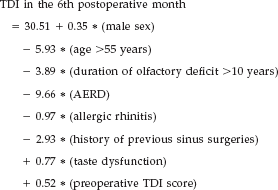
All variables (apart from the preoperative TDI score) are binary (no = 0 and yes = 1). Almost 70% of the variation in the 6th-month postoperative TDI score is explained by this model; the R 2 of regression was 68.2% (65.5% adjusted).
Using the Sniffin’ Sticks, patients’ olfactory function was categorized as anosmia, hyposmia, and normosmia, according to normative values for the Greek population 11 (Table 3). Marginal homogeneity test showed a significant improvement of each one of the four indices, from one measurement to another (all p < 0.001; Figs. 1 and 2).
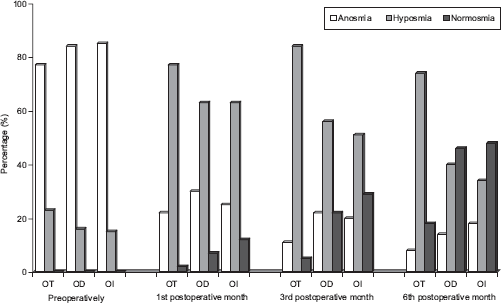
Odor threshold (OT), odor discrimination (OD), and odor identification (OI) scores of patients who underwent endoscopic sinus surgery pre- and postoperatively. The improvement of all indices over time was statistically significant (all p < 0.001; marginal homogeneity test).
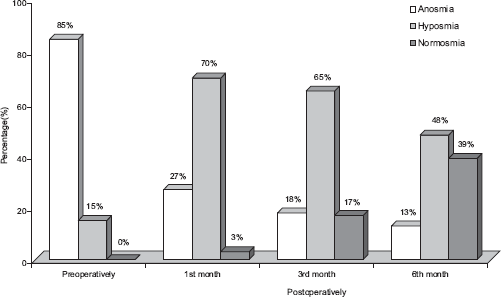
Olfactory function based on the threshold–discrimination–identification (TDI) score of patients who underwent endoscopic sinus surgery. The improvement of TDI scores from one measurement to another was statistically significant (all p < 0.001; marginal homogeneity test).
Olfactory function (A, H, and N) of patients who underwent endoscopic sinus surgery
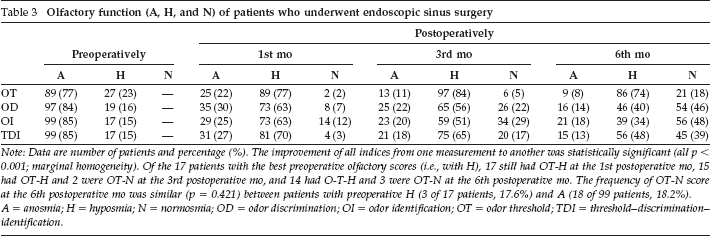
Note: Data are number of patients and percentage (%). The improvement of all indices from one measurement to another was statistically significant (all p < 0.001; marginal homogeneity). Of the 17 patients with the best preoperative olfactory scores (i.e., with H), 17 still had OT-H at the 1st postoperative mo, 15 had OT-H and 2 were OT-N at the 3rd postoperative mo, and 14 had O-T-H and 3 were OT-N at the 6th postoperative mo. The frequency of OT-N score at the 6th postoperative mo was similar (p = 0.421) between patients with preoperative H (3 of 17 patients, 17.6%) and A (18 of 99 patients, 18.2%).
A = anosmia; H = hyposmia; N = normosmia; OD = odor discrimination; OI = odor identification; OT = odor threshold; TDI = threshold–discrimination–identification.
Multivariate logistic regression analysis revealed that duration of olfactory deficit (p = 0.050), previous sinus surgery (p = 0.045), AERD (p = 0.048), and patients’ age (p = 0.048) remained strong independent predictors of normal olfactory function; a successful outcome was 2.6 (95% CI = 1.00–6.77) times more common in patients with short duration (>10 years) of olfactory deficit, 3.06 (95% CI = 1.11–9.67) times more common in patients without prior sinus surgery, 6.04 (95% CI = 1.10–36.46) times more common in patients without AERD, and 3.55 (95% CI = 1.01–12.43) times more common in young (≤35 years) patients. The probability (P) to attain normal olfactory function at the 6th postoperative month was calculated using the following statistical prediction model:
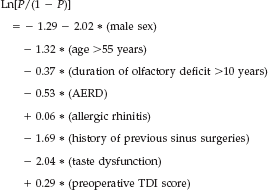
All variables (apart from the preoperative TDI score) are binary (no = 0 and yes = 1). This model correctly classified 76% of the patients. Positive predictive value of this model was 71% (95% CI = 54–83%), while the negative predictive value was 79% (95% CI = 67–87%); sensitivity was 64% (95% CI = 49–78%) and specificity was 83% (95% CI = 72–91%).
Discussion
There is a need for studies on predictive factors of olfactory function after ESS because current evidence is limited and contradictory.4,12,13 This deficiency may be attributed to the relatively limited availability of specific olfactory tests and the time burden needed for performing such tests. However, it is important to use an objective quantitative method to evaluate olfactory function, because many patients with CRSwNPs are not aware of their exact smell deficit. 14
In our study group, patients achieved a significant stepwise improvement of all olfactory function indices (OT, OD, OI, and TDI) over time. Improvement was more pronounced at the 1st postoperative month. This trend continued until the 6th month after surgery, when the major tissue remodeling changes inside the lamina propria end. 15 Additionally, out of the four indices of olfactory function, OT was the most sensitive over time, with the most pronounced change at the 1st postoperative month. OT may thus be affected earlier and more intensively than OD and OI abilities in the course of CRSwNP.
Patients in this study suffered from a severe CRSwNP (this is probably the reason why CRSwNP was resistant to medical therapy); 85% had anosmia, 15% had hyposmia, and no one had normal olfactory function preoperatively. At the 6th postoperative month, the percentage of patients with normal olfactory performance was almost 50% for OD and OI, but only 18% for OT, a finding suggesting that this index is more difficult to restore.
The use of different olfactory measures and different definitions of olfactory improvement has led to difficulty in interpretation of the published results. Reported success rates of ESS for olfactory rehabilitation in CRSwNP range from 50 to 70% depending on the measuring method.3,16–19 Klossek et al. 17 found olfactory recovery in 34.6% of patients after ESS, which is similar to our study. A number of studies have assessed olfactory outcome after ESS in CRSwNPs using Sniffin’ Sticks and generally agree with the findings of the present study.3,16,19,20
Nonetheless, there are contradictory findings about the time course of olfactory recovery after ESS in CRSwNP. Some studies suggest that CRSwNP patients find only brief and temporary olfactory improvement.2,21 Our results agree with results of other studies3,14,16,17 that suggest that ESS has a long-standing postoperative positive effect on olfaction in CRSwNP patients. A less invasive surgical procedure causes less damage to the olfactory neuroepithelium. The significant improvement in olfactory function after ESS may be explained, first, by the fact that surgery removes polypoid masses that obstruct airflow to the olfactory cleft and, additionally, by the fact that this removal helps the olfactory neuroepithelium to regenerate.14,15
We focused on specific prognostic clinical factors, which have not been quantitatively discussed before as independent predictors of the outcome of ESS on olfactory function in CRSwNP patients. Therefore, univariate ANCOVA showed that both TDI score and rates of normal olfactory function at the 6th postoperative month were significantly higher for patients with short (≤10 years) duration of olfactory deficit, 22 patients without previous sinus surgery, 22 patients without AERD, 23 and younger patients. Allergic patients 23 presented lower TDI scores at the 6th postoperative month. The TDI score at 6 months was independent of patients’ gender, smoking habits, 24 and taste disorders.
The biometric predictive model that we provided for calculation of the TDI score at the postoperative 6th month explains 68.2% of the observed score variation. In future studies, additional intra-, pre-, or postoperative parameters may be explored, to explain a larger part of the variation. It would be interesting to test applicability of our models in CRSwNP patients living in environments different from our study population.
The clinical relevance of the models is that they may enable otolaryngologists to answer their patients’ questions about the anticipated benefit for olfaction after ESS and may support clinical decisions on the holistic management of CRSwNP patients. Evaluation of olfaction by the Sniffin’ Sticks method may not only serve as an objective method for early diagnosis and treatment monitoring in clinical practice, but may also be useful in more reliably counseling patients and in supporting clinical management decisions tailored to each individual patient.
Footnotes
Other (Nonfinancial) Conflict of Interest: none