
Abstract
Background
There is growing evidence of positive correlations between asthma (AS) and obesity in adults and children. Leptin is an obesity gene product secreted by white adipose tissue; elevated serum levels are found in obese adults and children. Recently, leptin has also been found to be associated with allergic rhinitis (AR). However, the links between serum leptin, atopic AS, and AR remained undetermined. Because AS and AR share common allergic inflammatory mechanisms, our aim was to determine if there were any differences in serum leptin levels between asthmatic children and nonasthmatic children with AR.
Methods
We studied 114 children (67 boys and 47 girls): 68 with mild intermittent-to-moderate persistent atopic AS (AS children) and 46 with mild-to-moderate persistent AR without AS (AR children; overall mean age, 8.51 years; range, 5–18 years). Body mass index (BMI), serum leptin, pulmonary function, and atopy parameters (serum IgE and eosinophil levels) were measured.
Results
Compared with AR children, AS children had higher body weights (kg), body mass indices (kg/cm2), and serum leptin levels (ng/mL). Multiple linear regression analyses showed that serum leptin concentrations differed significantly for girls, being overweight and between disease groups (AS and AR children).
Conclusion
Our results indicate that a higher serum leptin level has stronger association with mild-to-moderate persistent AS compared with AR. Hence, serum leptin may be a stronger predictor for childhood AS compared with AR. Among the asthmatic children, higher serum leptin levels also showed stronger associations with female gender and being overweight.
However, the causality between obesity and AS, still has not been well established. Asthmatic and obese patients might share similar predisposing factors, such as sedentary life styles, dietary factors, immunologic factors, hormonal factors, genetic predispositions, systemic inflammation during clinical disease progression, and reductions in lung compliance.9,10
The atopic march hypothesis suggests that AS and AR might share similar allergic inflammatory mechanisms. The America Academy of Allergy, Asthma and Immunology reported that up to 78% of patients with AS have allergic rhinitis (AR) and 38% of patients with AR have AS. 11 The Allergic Rhinitis and Its Impact on Asthma guidelines 12 had proposed the concept of “one airway one disease”; however, there are some differences between AR and AS.
Based on the hypothesis of an obesity–AS relationship, serum leptin is also thought to be associated with AS. Leptin is a 16-kDa adipocyte-derived protein hormone, which is encoded by the ob gene and produced by white-adipose tissue. Leptin is thought to play a key role in body weight regulation. It acts on the hypothalamus to induce satiety, inhibiting food intake, increasing energy expenditure and metabolism. Recently, leptin has been reported to be involved in up-regulating immune responses. Leptin enhances the proliferation of CD4+ T cells, mast cells, and macrophages and promotes Th1 immune responses with increased production of proinflammatory mediators, such as tumor necrosis factor (TNF) α, interleukin (IL)-6, and interferon γ, which are associated with AS. 13 Leptin can also activate the transcription factors activating protein I and nuclear factor-κB in endothelial cells, which result in airway inflammation and airway narrowing with limitation of airflow. 14 Serum leptin is elevated with increasing body fat percentage and body fat mass; thus, it is increased in obese individuals. 15 This is probably caused by of leptin resistance and hypertrophic and hyperplastic adipocytes.9,16
High serum leptin levels were associated with increased risk of AS in children and adults.17,18 Recent studies also found that patients with AR had significantly higher serum leptin levels than normal control subjects.19–22 However, the roles of serum in children with AR and AS have not been investigated; our aim was to determine if there were any differences in the serum leptin levels between asthmatic children and nonasthmatic children with AR.
Methods
Study Population
Our study was performed at the outpatient Allergy and Asthma Clinic of the Department of Pediatrics, Medical Center of Chung Shan Medical University. From January 2004 to December 2005, 114 children (67 male and 47 female patients; overall mean age, 8.51 years; range, 5–18 years) were enrolled after written informed consent had been obtained from their parents. All subjects were divided into 2 groups, this included 68 patients with mild intermittent-to-moderate persistent atopic AS (AS children; 38 boys; 30 girls; mean age, 8.74 years) and 46 patients with mild-to-moderate persistent AR, but without AS (AR children; 29 boys; 17 girls; mean age; 8.16 year). All AS children were considered to be atopy with allergic sensitization to at least one aeroallergen or food allergen. All cases of AR involved in this study are classified as a perennial or persistent type. Each patient had been evaluated for at least 2 years before the final clinical diagnosis was established. Among the nonasthmatic children with AR, those with abnormal pulmonary function tests and subsequent AS occurrence were excluded.
Measurements
Demographic characteristics were recorded, body height and weight were measured, and BMI values were calculated as the ratio of the patient's body weight to body height squared (weight [kg]/height 2 [m2]). Overweight was defined according to the BMI limits provided by Department of Health, Taiwan, R.O.C, for different yearly ages.
Venous blood samples were collected and stored at –70°C until analyzed. Serum leptin, IgE, and eosinophil levels were measured. Serum leptin concentrations (ng/mL) were measured by enzyme-linked immunosorbent assay (ELISA) using a commercial kit with a monoclonal antibody specific for human leptin (DSL-10-23100 ACTIVE Human Leptin ELISA Kit; Diagnostic Systems Laboratories, Inc., Webster, TX).
Pulmonary function tests were performed on the first visit and during the symptomatic times by using a Microlab desktop spirometer (Micro Medical Ltd., Rochester, Kent, UK). Pulmonary function parameters included forced vital capacity (FVC), forced expiratory volume/1 second (FEV1), and FEV1/FVC. All asthmatic children had undergone appropriate pulmonary function tests. An FEV1 of < 80% of predicted value and FEV1/FVC ratio of <0.80 were considered as impaired lung function; moreover, bronchodilator response to an inhaled β2-agonist with improvements in FEV1 of ≥12% and ≥200 mL and a peak expiratory flow of ≥20% indicates the diagnosis of AS. All patients with AR also underwent lung function tests to rule out for AS. Patients with AR and abnormal pulmonary function tests were excluded.
Diagnosis of Atopic Diseases
The diagnosis of AS and severity classification was made according to the latest Global Initiative for Asthma guidelines: Global Initiative for Asthma Report, Global Strategy for Asthma Management and Prevention (updated December 2008). 23 The diagnosis of AR and severity classification was made according to the latest Allergic Rhinitis and its Impact on Asthma guidelines of 2008.
Statistical Analysis
Independent-samples t-tests were used to compare demographic data. General linear univariate models were used to evaluate relationships between serum leptin levels with sex (1, male; 0, female), being overweight (1, overweight; 0, not overweight), disease (1, asthmatic AR; 0, nonasthmatic with AR), and lung function status (1, impaired lung function; 0, normal lung function). Multiple linear regression analysis was also used to evaluate possible differences of leptin levels for sex, being overweight, atopic disease, and lung function status. Multiple logistic regression was used to evaluate AS as a dependent factor for estimating the associations between leptin, sex, being overweight, impaired lung function, and atopy parameters (IgE and eosinophil count). Sex, being overweight, and impaired lung function were considered categorical covariates. Correlations between serum leptin levels, body height, BMI, atopy (IgE and eosinophil count), and pulmonary function parameters (FEV1, FVC, and FEV1/FVC) were analyzed by Pearson's correlation test. The values of p < 0.05 were considered significant. All statistical analyses were done using SPSS for windows, Version 15.0 (SPSS, Inc., Chicago, IL).
Results
This study included 68 patients with AS and 46 nonasthmatic patients with AR. Their clinical characteristics are summarized in Table 1. Mean values for age and body height did not show any significant differences between the two groups. However, comparing the asthmatic children with those with AR, body weights (mean, 34.84 versus 30.79; p = 0.041), body mass indices (mean, 19.09 versus 17.71; p = 0.040), and serum leptin levels (mean, 12.59 versus 8.73; p = 0.045) were statistically different between the 2 groups. AS children had higher BMI indices and serum leptin levels than AR children. Surprisingly, AR children had significantly higher eosinophil counts than AS children (p = 0.024).
Patient characteristics
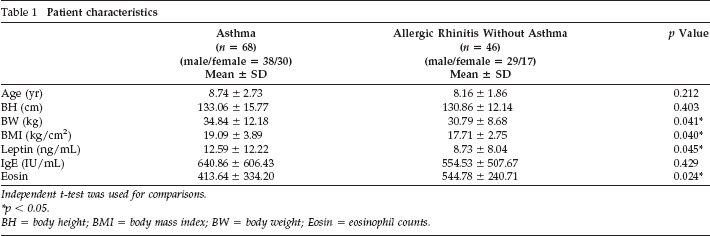
Independent t-test was used for comparisons.
p < 0.05.
BH = body height; BMI = body mass index; BW = body weight; Eosin = eosinophil counts.
After adjusting for pulmonary function parameters, multiple linear analysis was used with leptin as the dependent variable to assess its associations with sex, being overweight, disease status, and impaired lung function (FEV1 of <80% of predicted value and FEV1/FVC ratio of <0.80). Serum leptin concentrations showed statistically significant differences among sexes, being overweight, and disease groups (p = 0.004, <0.001, and 0.019, respectively; (Table 2) but had no significant difference between children with impaired lung function and those with age-appropriate lung function. Multiple linear regression showed that serum leptin levels were significantly higher for female patients, being overweight, and the AS group (Table 2). The percentage of overweight children in AS and AR groups were 47 and 35%, respectively. Among overweight children (n = 48), asthmatic females (n = 18) had nearly twice the serum leptin levels compared with nonasthmatic girls (n = 7; mean value, 28.93 ng/mL versus 15.57 ng/mL). However, this association was not found in overweight boys (mean value, 18.20 ng/mL versus 13.30 ng/mL).
Multiple linear regression analysis in the study group *
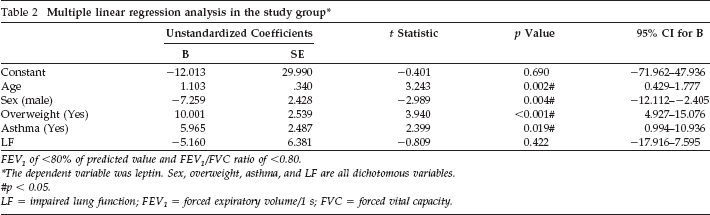
FEV1 of <80% of predicted value and FEV1/FVC ratio of <0.80.
The dependent variable was leptin. Sex, overweight, asthma, and LF are all dichotomous variables.
p < 0.05.
LF = impaired lung function; FEV1 = forced expiratory volume/1 s; FVC = forced vital capacity.
A multiple logistic regression model was used to determine predictors of atopic diseases (Table 3). These results showed that serum leptin levels had a significant, although weak, increased odds for AS (odds ratio [OR] = 1.10; 95.0% CI = 1.016–1.190; p = 0.018). However, there were no other significant factors, including sex, being overweight, or atopy parameters (IgE levels and eosinophil counts). Statistically significant correlations were found between serum leptin levels and age, BMI, and body height, but no significant associations were found between serum leptin levels and atopy and pulmonary function parameters (Table 4). Serum leptin levels also showed positive correlations with BMI in both sexes (Fig. 1).
Predictors analysis in the study group *
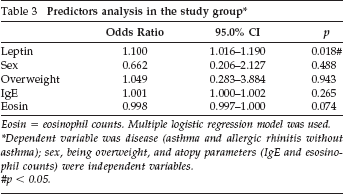
Eosin = eosinophil counts. Multiple logistic regression model was used.
Dependent variable was disease (asthma and allergic rhinitis without asthma); sex, being overweight, and atopy parameters (IgE and esosinophil counts) were independent variables.
p < 0.05.
Correlation coefficients between serum leptin and body height, BMI, atopy, and pulmonary function parameters

Correlation is significant at the 0.05 level (two-tailed).
Correlation is significant at the 0.01 level (two-tailed).
BH = body height; BMI = body mass index; Eosin = eosinophil counts; FEV1 = forced expiratory volume/1 s; FVC = forced vital capacity.
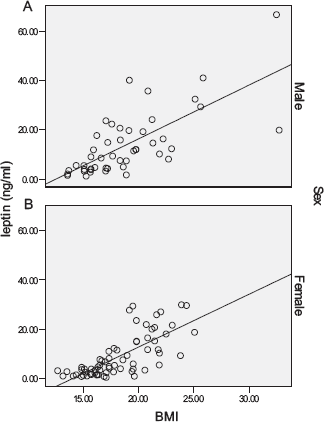
Association between serum leptin level and body mass index (BMI). Serum leptin levels showed positive correlation with BMI in both sexes (r = 0.719; p = < 0.001).
Discussion
Several studies have indicated that serum leptin levels were found to be significantly higher in patients with AR during allergen exposure and symptomatic periods.19–21 Hsueh et al. also proposed that adipokines, including leptin, adiponectin, and resistin, might be related to the severity of AR; nevertheless, serum leptin may serve as a predictor of disease severity in childhood AR.22,24 Our results indicate that an elevated serum leptin level has stronger association with mild-to-moderate AS compared with AR. We also found that higher serum leptin levels were more strongly associated with female gender and being overweight in those asthmatic children. In accordance with previous studies, the statistical association between higher serum leptin levels and AS was stronger in girls than in boys.16,17,25,26 This may be caused by a higher proportion of fat to overall weight in girls. However, eosinophil counts have been found significantly higher in AR children than in AS children. This may be because most AS children experienced more prominent clinical manifestation than AR children; thus, they are more likely to receive regular AS specialist treatment, especially treatment with corticosteroids, at a local medical department or hospital, which result in a decrease in serum eosinophil counts.
Our results showed that serum leptin level contributed significantly, but only weakly, to an increased odds for AS (OR = 1.10; 95.0% CI = 1.016–1.190; p = 0.018). This may have been caused by a limited study population size and a wide range of ages among the study participants. In addition, based on the atopic march hypothesis, we considered that among those nonasthmatic children with AR, some might subsequently develop AS in the future. This possibility reduces the differences of serum leptin levels and weakens the impact of leptin between the two groups. However, the serum leptin levels of both groups in our study were significantly higher than those in the control groups that have been previously reported (Guler et al.: 2.26 ng/mL [1.26–4.71]; mean age, 6.1 ± 3.4 years 18 ; Hsueh et al.: 2.87 ng/mL [1.12–5.85]; mean age, 6.18 ± 2.43 years 22 ; Kim et al: 2.10 ng/mL [0.71–4.49]; mean age, 9.8 ± 2.1 years 27 ). Serum leptin level have positive correlation with age and thus display a wide normal range. Therefore, we suggest that serum leptin could be a predictor for AS occurrence.
In a large cross-sectional study that enrolled 5876 adults, Sood et al. suggested that higher serum leptin levels were associated with current AS in women, especially in premenopausal women. Adult women in the highest quartile of serum leptin levels had an OR of 1.85 for current AS compared with an OR of 1.27 in men. 17 Nevertheless, the results of studies among children on these relationship between serum leptin levels and AS are not consistent. In a cross-sectional study, Guler et al. reported that higher serum leptin levels were associated with AS in boys but not in girls, although serum leptin levels are usually higher in girls than in boys, 18 which was in contrast to our findings. They further implied that a 1-U increase in log leptin was associated with a twofold increased odds for AS after adjusting for BMI. However, we did not find this relationship in our study (data not shown).
Consistent with the studies by Sood et al., 17 Guler et al., 18 and Jartti et al., 25 we noted that the relationship between BMI and AS remained significant after adjusting for serum leptin levels; i.e., the association between BMI and AS is not affected by leptin and, thus, leptin might be considered an independent predictor of AS.17,18,25 Our results showed that BMI was significantly associated with AS (OR = 1.13; 95.0% CI = 1.003–1.282; p = 0.045) and that this relationship remained after adjusting for leptin, sex, and being overweight (OR = 1.28; 95.0% CI = 1.001–1.626; p = 0.044).
Kim et al. found that serum leptin levels showed no differences among atopic AS, nonatopic AS, and control groups. However, serum leptin and adiponectin were found to be closely associated with some pulmonary function parameters, including FEV1 and forced expiratory flow at 25–75%. 27 However, we did not find this relationship in our study.
Our results also show that higher BMI was associated with AS but not with AR (Table 1) and that higher BMI was associated with higher serum leptin levels in both sexes (Fig. 1), which might induce the onset of AS or exacerbate the severity of AS. Our results agree with many previous studies showing that the prevalence of increasing BMI and subsequent overweight or obesity is associated with the increased prevalence of AS. Most prospective studies show that obesity is a risk factor for AS and have found positive correlations between baseline BMI and the subsequent development of AS. The risks of AS increase from 1.1-fold to threefold among the obese.28–30
Numerous epidemiological data implicate obesity for increasing the risks for AS, atopic disease, and autoimmune diseases. Obesity is recognized as a state of chronic, low-grade systemic inflammation and has been associated with reduced AS control. Proinflammatory cytokines and hormones, such as TNF-α, IL-6, interferon γ, transforming growth factor β1, and leptin, are markedly increased in obesity, which could contribute to airway hyperresponsiveness and inflammation.31,32 Huang et al. have confirmed the endothelial activation in obese children with significant elevated soluble intercellular adhesion molecule levels. 33 In obesity, lung compliance and lung function parameters, including functional residual capacity, FEV1, FVC, and tidal volume, are reduced. Comorbidities of obesity, such as gastroesophageal reflux disease, sleep-disordered breathing, dyslipidemia, hypercholesterolemia, type 2 diabetes and hypertension with diastolic heart failure, and pulmonary congestion, may provoke or exacerbate AS. 34
However, many aspects of the putative link between overweight/obesity and increased prevalence of AS are unclear and controversial. Two reviews concerning obesity and AS suggested that the overall impact of obesity on AS incidence and prevalence appears to be modest, and that this relationship depends on other factors such as age and sex.10,35 Nevertheless, Sutherland et al. reported that increased BMI was not associated with clinically significant worsening of impairment in subjects with mild-to-moderate persistent AS. 36
Our study has some limitations, including a limited number of study subjects, a wide range of ages among the study participants, and lack of a control group. In addition, all of our patients were under treatments during the study period. Their lung function results and serum leptin levels may be improved or altered, which would not reflect their actual physiological status.
In conclusion, we suggest that higher serum leptin levels have stronger association with mild-to-moderate AS, compared with AR. Therefore, serum leptin may be a stronger predictor for childhood AS compared with AR. Among the asthmatic children, higher serum leptin levels also showed stronger associations with female gender and being overweight.