
Abstract
Background
Many researchers have focused on the definition and pathophysiology of localized mucosal allergy. However, there are few studies on its clinical characteristics and therapeutic outcomes. The goal of this study was to analyze the prevalence, epidemiology, clinical characteristics, and response to antiallergic medication of localized mucosal allergy patients compared with those in patients with allergic rhinitis.
Methods
Among 836 patients suspected to have rhinitis, 29 patients with localized mucosal allergy (group A) and 29 patients with allergic rhinitis (group B) were selected. Medical history, family history, symptoms, and their severity were obtained using a questionnaire. The change in minimal cross-sectional area (MCA) after provocation was measured by acoustic rhinometry. After 2 weeks of antihistamine medication, the changes in symptoms were compared between groups.
Results
The prevalence of localized mucosal allergy was ∼3.5%. There were no differences in patient history, symptoms, or symptom severity. The decrease in MCA after provocation was not significantly different. After two weeks of oral antihistamine (ebastine 10 mg once daily), group A reported significantly less symptom improvement than group B.
Conclusion
Because patient or family history and clinical picture are very similar in localized mucosal allergy and allergic rhinitis, clinicians should take more care in differentiating them. Based on the reduced effectiveness of an oral antihistamine alone, a combined regimen of oral and topical antihistamine or anti-inflammatory medication is recommended for patients with localized mucosal allergy.
Keywords
Materials and Methods
From January 2004 to February 2007, 836 patients (346 male and 490 female patients; 16–65 years old) suspected to have allergic rhinitis or PNAR by patient history and physical examination using nasal endoscopy were enrolled. Patient clinical characteristics, such as history of other allergic disease, family history of allergy, and the most uncomfortable time of the day, were obtained by questionnaire. Patients were classified according to the Allergic Rhinitis and Its Impact on Asthma 2008 classification of allergic rhinitis. 9 Patients who had other pathological conditions (such as chronic rhinosinusitis or septal deviation), had used an antihistamine, inhaled or systemic steroid within 1 month before the study, had unstable systemic disease, pregnant or lactating women, and those <16 years old were excluded from this study. The study was approved by the Institutional Review Board of Inha University Hospital before enrollment was initiated.
All patients underwent an allergic SPT with Dermatophagoides pteronyssinus (Allergopharma, Reinbek, Germany) antigen performed by the simple prick method. Histamine and normal saline were used as the positive and negative control, respectively. The response was graded as strongly positive (3 or 4+), weakly positive (1 or 2+), or negative (0+). Tests were performed throughout the year, at the time patients first visited our hospital complaining of symptoms. Minimal cross-sectional area (MCA) was defined as the smallest cross-sectional area of the nasal cavity. Changes in symptoms, such as nasal obstruction, rhinorrhea, and itching, after the allergen challenge were measured using a visual analog scale (VAS). The VAS was composed of a 10-cm line with marks at every 1-cm interval on which patients rated severity of their symptoms from 1 to 10. Sneezing was also assessed by VAS before the provocation and the number of sneezes was counted after the provocation. All tests were done by the same examiner.
For the nasal provocation test, 40–50 μL of D. pteronyssinus antigen diluted 1:10 in a 5-mL pump dosage sprayer was used for provocation, and an ECCOVISION acoustic rhinometer (E. Benson Hood Laboratories Inc., Pembroke, MA) was used for acoustic rhinometry. The temperature and relative humidity in the laboratory were maintained at 22°C and 50%, respectively. Patients were asked to sit calmly for at least 15 minutes and then completed the baseline VAS before the challenge. Baseline acoustic rhinometry was also performed before any challenge. Patients then received a 0.9% normal saline control challenge, and 5 minutes after the challenge, the VAS and acoustic rhinometry were repeated. Patients with a positive result (>29% decrease in MCA) were classified as a nonspecific hyperresponse group and were excluded from the study. Patients with a negative result waited an additional 10 minutes for the effects of the challenge to disappear before the D. pteronyssinus antigen challenge was performed. The VAS and acoustic rhinometry were repeated at 15 and 30 minutes after the challenge. No patient showed severe side effects such as bronchospasm during or after the challenge.
Localized mucosal allergy (group A) was defined as the presence of typical clinical symptoms of rhinitis, a negative SPT to D. pteronyssinus, normal serum-specific IgE level, and a positive provoked response (>29% decrease in MCA by acoustic rhinometry after local application of D. pteronyssinus antigen into the nasal cavity). Allergic rhinitis (group B) was defined as presence of typical clinical symptoms of allergic rhinitis, a strongly positive (3+ or higher) SPT to D. pteronyssinus, and a positive provoked response. Patients who showed no response (<25% decrease in MCA after D. pteronyssinus challenge) were classified as subclinical allergy and were excluded from the study.
In each group, patients who agreed to take medication according to our protocol were given an oral antihistamine (ebastine, 10 mg, once daily; BoRyung Pharmacy, Seoul, Korea). After 2 weeks on the medication, changes in symptoms were measured using VAS to evaluate responses to the medication.
VAS scores and results of nasal provocation test were compared between groups A and B. SPSS 16.0 program (SPSS, Inc., Chicago, IL) was used for statistical analysis, and the independent t-test or paired t-test were used to compare the data. Linear regression analysis was used to evaluate the correlation of symptom change and changes of total nose volume (TNV) or MCA. A p < 0.05 was accepted as statistically significant. The statistical power calculator was used to calculate the statistical power. 10 The two-tailed test and 5% of α-error level were used also.
Results
Among the 836 patients clinically suspected to have allergic rhinitis or PNAR, 29 (3.5%, 12 male and 17 female patients; 16–59 years old; mean age, 37.6 years) were diagnosed as localized mucosal allergy (group A). Twenty-nine age- and sex-matched patients with allergic rhinitis who met the study criteria were randomly selected as group B. Group A tended to have a larger proportion of patients with accompanying allergic disease and family history of allergy, but this was not significantly different between the groups (p > 0.05; Table 1). Ten patients (34.5%) in group A and 37.9% in group B felt most uncomfortable in the early morning.
Proportion of patients who had other allergic disease or family history of allergy among study participants
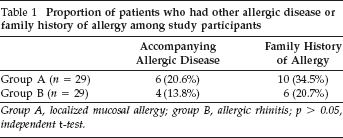
Group A, localized mucosal allergy; group B, allergic rhinitis; p > 0.05, independent t-test.
Grouping patients according to the Allergic Rhinitis and Its Impact on Asthma 2008 classification, 9 the intermittent moderate-severe subgroup was the most common in both groups (Fig. 1). Most patients reported nasal stuffiness and runny nose as the most severe or uncomfortable symptom in both groups, with no significant difference between groups (Fig. 2). Group A tended to have a larger decrease in MCA after nasal D. pteronyssinus provocation test than group B, but this was not statistically significant (group A, 34.1%, versus group B, 32.7%; p > 0.05). When the authors defined total nasal symptom score (TNSS) as the sum of all symptoms, the change of TNSS was well correlated with change of TNV and MCA (TNSS change and TNV change, R = 0.522 and p = 0.004; TNSS change and MCA change, R = 0.714 and p < 0.001; Fig. 3).
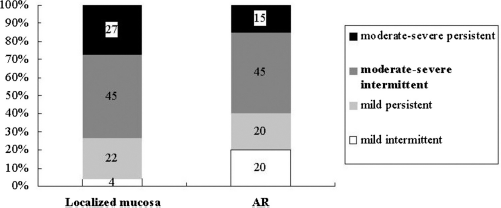
Proportions of patients according to Allergic Rhinitis and Its Impact on Asthma 2008 classification of allergic rhinitis.
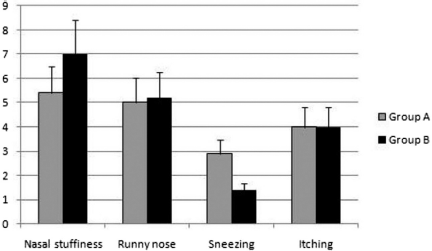
Severity of symptoms in each group before any intervention (*p < 0.05).
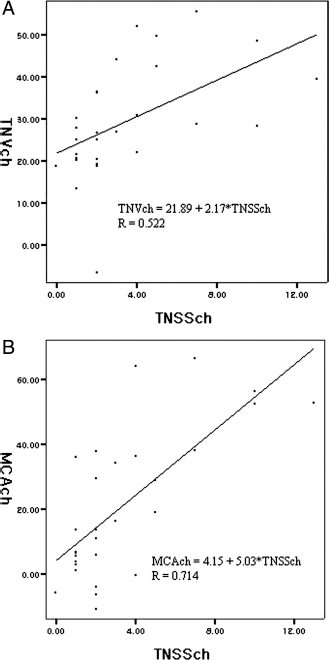
The correlation between change of symptoms and (A) change of TNV or (B) change of MCA. (TNSSch, change of total nasal symptom score, TNVch, change of TNV; MCAch, change of minimal cross-sectional area).
Twelve patients in group A and 13 patients in group B agreed to take an antihistamine according to the study protocol. The symptom changes in these patients were measured after 2 weeks on the medication. Although both groups showed meaningful improvement in their symptoms, patients in group A had significantly less improvement in runny nose and itching (Wilcoxon signed-rank test, p < 0.05; Fig. 4).
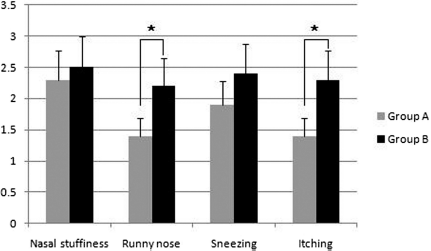
Change of nasal symptoms after 2 weeks of antihistamine medication (Wilcoxon signed-rank test, *p < 0.05).
Discussion
The proportion of localized mucosal allergy was ∼3.5% among patients with clinically suspected rhinitis. Rondon et al. reported that 54% of 50 patients with PNAR had a positive nasal provocation test, and only 12% had positive specific IgE serum levels. 3 Because differentiating allergic from nonallergic rhinitis is difficult in the office setting, it is important to get the prevalence of localized mucosal allergy in all patients with rhinitis, not just among patients with PNAR.
Following the identification of localized mucosal allergy by Huggins and colleagues, 4 many researchers have tried to characterize it in many different ways. Huggins et al. suggested the presence of clinical symptoms of rhinitis and an elevated level of specific IgE in nasal secretions after nasal provocation test using house-dust mite antigen. 4 Carney et al. claimed that in some patients with IR, mucosal mast cells and eosinophils were increased in histological specimens. 11
The pathophysiology of localized mucosal allergy remains to be elucidated, but there are many hypotheses on its etiology. It could be the result of “covert allergy,” which means sensitivity to an allergen not tested. 12 Although >40 different antigens were used when performing the SPT, the possibility that some insects, arachnids, crustaceans, or mollusks could be the etiologic antigen still exists. The authors used house-dust mite antigen because allergic responses to this antigen are quite common in Korea and the local allergic response existed to mite antigen without evidence of systemic allergy. In addition, because all patients had a positive response to house-dust mites in the nasal provocation test, we suggest that the etiologic antigen was house-dust mite.
The concept of site-specific immune response and a non–IgE-mediated allergy are also believed to play a role in localized mucosal allergy.13–17 Immunohistochemistry was not performed to assess this possibility because this study was focused on the clinical aspects only.
Excluding the possibility of poor technique in performing SPT, the absence of atopy may be explained by the quality of the allergen used. 8 In this study, the same allergen was used in both allergic and nonallergic patients, and because allergic patients showed an excellent response, the quality of antigen can be excluded as an etiologic factor.
Although the proportion of comorbid allergic disease or family history was slightly higher in localized mucosal allergy group, the difference was not significant. This correlates with results of Rondon et al., who concluded that there was no difference in family history, duration of symptoms, and city dwelling. 6 The timing of maximal discomfort was early in the morning in both groups. These similarities in clinical picture make differentiating localized mucosal allergy from allergic rhinitis very difficult.
In this study, patients felt that nasal congestion and runny nose were the most uncomfortable symptoms. This result is somewhat different from that of Rondon et al., who reported posterior rhinorrhea as the most uncomfortable symptom. 6 Because runny nose and posterior rhinorrhea could be different aspects of the same symptom, these results are not necessarily different.
The fact that the change in MCA after the nasal provocation test was not significantly different between groups emphasizes the importance of nasal provocation test as a diagnostic tool for all types of nasal allergy. In fact, the nasal provocation test should be the gold standard in diagnosing nasal allergy in the clinic, with exclusion of nonspecific nasal hyperreactivity by normal saline challenge. 18 Patients with localized mucosal allergy tended to show more decreased MCA after provocation than their allergic counterparts (although not statistically significant). Therefore, they could have a more severe clinical picture under specific provocation and thus require more careful management.
The mainstay of localized mucosal allergy treatment is topical anti-inflammatory regimens. 8 The topical antihistamine azelastine has been shown to be effective in treating allergic and nonallergic rhinitis.19–22 The use of capsaicin and ipratropium bromide has been reported to be useful in alleviating symptoms of nasal blockage and rhinorrhea.23,24 An oral antihistamine was used in this study. The authors selected oral antihistamines instead of topical ones because some covert allergy (described previously) or some unknown systemic mechanisms as well as non–IgE-mediated response could be responsible for localized mucosal allergy. To our knowledge, this study is the first to evaluate the effect of oral antihistamine in localized mucosal allergy. The fact that patients with localized mucosal allergy showed meaningful improvement suggests that there is an unknown systemic pathophysiological pathway that is blocked by the oral antihistamine. Because the clinical benefit of the oral antihistamine was weaker in localized mucosal allergy patients, combination therapy with oral and topical antihistamine or anti-inflammatory agent could be more effective in relieving symptoms.
In evaluating the therapeutic effect of oral antihistamine, only 12 patients in group A and 13 patients in group B participated in follow-up among 29 patients each. These numbers are small but large enough to make a meaningful comparison with regard to improvements of symptoms. Using the power calculation described in the Materials and Methods section, the calculated statistical power was 100%.
One weakness of this study is the short follow-up interval (2 weeks after medication); however, the short-term effectiveness of a medication is crucial in the outpatient setting because many patients judge effectiveness of medications in <2 weeks of taking it. This short-term effect is very important in improving compliance and rapport with patients, which, in turn, will allow for the desirable long-term treatment and results.
Conclusions
The prevalence of localized mucosal allergy among patients with rhinitis was 3.5%. Because the patient history, family history, and clinical picture of localized mucosal allergy are very similar to those in allergic rhinitis, clinicians should take more care in differentiating them. An oral antihistamine alone is less effective in patients with localized mucosal allergy; thus, a combined regimen of oral and topical antihistamine or anti-inflammatory medication is recommended.