
Abstract
Background
Elite swimmers are at increased risk of asthma, which has been related to chronic effects of pool chlorine environment. However acute effects of swimming on rhinitis remain unknown.
Objective
We aimed to assess the nasal response to exercise in competitive swimmers compared with competitive runners.
Methods
Measurements of nasal symptoms, peak nasal inspiratory flow, lung function, dyspnea, and of airway inflammation were obtained before and after a training session of 19 international-level swimmers and 13 professional runners. Exercise-induced rhinitis was defined as a fall in peak nasal inspiratory flow above 20% from baseline and atopy by positivity to skin-prick testing. Changes within groups were compared using paired t test and differences compared by analysis of covariance.
Results
Prevalence of exercise-induced rhinitis was similar between swimmers and runners, respectively 21% and 23%. Contrary to runners, swimmers experienced a decrease in nasal inspiratory flow levels and increase in sneezing, nasal congestion, itching, and postnasal drip after exercise. However, difference in changes was only significant for postnasal drip (p = 0.050). All subjects experiencing exercise-induced rhinitis were nonatopic. An overall improvement in nasal flows, sneezing, and itching after exercise was observed in atopic athletes, although no significant differences in changes compared with nonatopic athletes existed.
Conclusion
Swimmers, contrary to runners, experience a worsening of nasal function after training. Although these differences were only significant for postnasal drip, our results provide support to the existence of a “swimming-induced rhinitis” independent of the atopic status of the athlete.
Methods
International-level swimmers of the main team of Futebol Clube do Porto (n = 19) and professional runners enrolled on the Training Control Program of the Portuguese Athletics Federation living in northern Portugal (n = 13) were invited to participate. Subjects with history of upper respiratory tract infections in the previous two weeks were excluded, and all agreed to participate. No differences existed between swimmers and runners groups in prevalence of asthma or rhinitis, overall quality of life related with rhinitis, or consumption of antiallergic drugs (Table 1). Swimmers were younger and of lower-competing experience, but the same level of total physical activity. Measurements were obtained before and 5 to 10 minutes after the training session. Swimmers swam 6500 meters in an indoor swimming pool (water at 28°C, free chlorine levels 1.7 mgL–1) at high intensity (above 95% of Vo2max), and runners exercised on an outdoor track (4000 meters, at 9°C and 74% humidity, above 95% of Vo2max). Nasal symptoms (sneezing, runny nose, congestion, itching, and postnasal drip) were assessed using visual analog scales and peak nasal inspiratory flow measurements performed with a nasal inspiratory peak flow meter (In-Check Nasal, Clement Clarke, Harlow, UK) according to manufacturer's instructions. Exercise-induced rhinitis was defined as a fall in peak nasal inspiratory flow above 20% from baseline. 6 Spirometry was performed according to American Thoracic Society recommendations and dyspnea rated on the Borg scale immediately before each lung function measurement. Airway inflammation was assessed by fractional exhaled nitric oxide (FeNO), measured with the NIOX Mino system (Aerocrine, Stockholm, Sweden). Baseline rhinitis quality of life was assessed using the Rhinoconjunctivitis Quality-of-Life Questionnaire (RQLQ). 7 Atopy was defined by positivity to skin-prick testing to common aeroallergens. Subjects were asked to withhold antihistamines, leukotriene receptor antagonists, nasal steroid sprays, and long-acting β2-agonists for 7 days and of short-acting β2-agonists for 1 day before measurements. Inhaled steroids were not discontinued. Changes within groups were compared using paired t test, and differences between exercise and groups were compared by analysis of covariance with baseline value as covariate. Values of p < 0.05 were regarded as significant. The study was approved by the Hospital Ethics Committee, and all subjects or their parents provided informed consent.
Baseline characteristics of participants according to type of sport
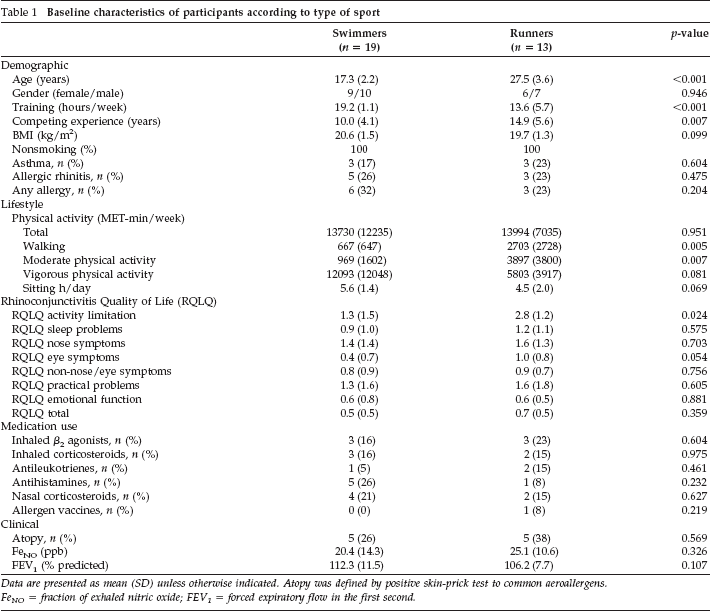
Data are presented as mean (SD) unless otherwise indicated. Atopy was defined by positive skin-prick test to common aeroallergens.
FeNO = fraction of exhaled nitric oxide; FEV1 = forced expiratory flow in the first second.
Results
The prevalence of exercise-induced rhinitis was similar between swimmers and runners, respectively 21% (4 out of 19) and 23% (3 out of 13). Contrary to runners, swimmers experienced a decrease in the nasal inspiratory flow levels and an increase in sneezing, nasal congestion, itching, and postnasal drip after exercise. However, difference in changes was only significant for postnasal drip (Table 2). Both swimmers and runners reported increased levels of dyspnea and decreased comfort after exercise, without differences between them. A significant decrease in exhaled nitric oxide was observed in runners after exercise, but not in swimmers.
Changes in nasal and lung function and in exhaled nitric oxide after training according to type of sport
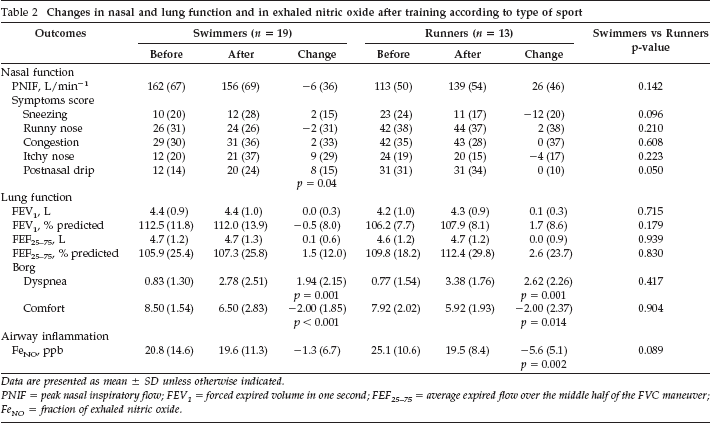
Data are presented as mean ± SD unless otherwise indicated.
PNIF = peak nasal inspiratory flow; FEV1 = forced expired volume in one second; FEF25–75 = average expired flow over the middle half of the FVC maneuver; FeNO = fraction of exhaled nitric oxide.
All subjects experiencing exercise-induced rhinitis were nonatopic. An overall improvement in nasal flows, sneezing, and itching after exercise was observed in atopic athletes, although no significant differences in changes compared with nonatopic athletes existed (Table 3). No significant differences in changes in nasal and lung function and in exhaled nitric oxide after exercise challenge according to atopic status were observed between groups (Table 3).
Changes in nasal and lung function and in exhaled nitric oxide after training according to atopic status
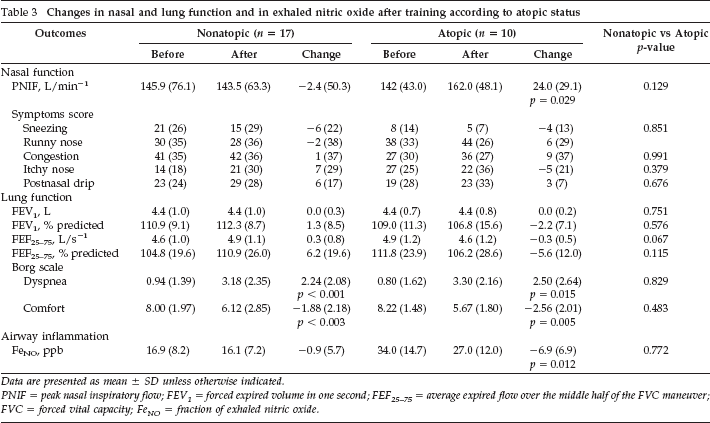
Data are presented as mean ± SD unless otherwise indicated.
PNIF = peak nasal inspiratory flow; FEV1 = forced expired volume in one second; FEF25–75 = average expired flow over the middle half of the FVC maneuver; FVC = forced vital capacity; FeNO = fraction of exhaled nitric oxide.
Discussion
Exercise-induced rhinitis is characterized by itching, sneezing, rhinorrhea, postnasal drainage, nasal congestion, and occasional anosmia provoked by exercise. 8 International-level swimmers, compared to runners, experienced decreased nasal flows and increased sneezing, nasal congestion, itching, and postnasal drip after exercise. However these differences were only significant for postnasal drip. These results provide further support to the existence of a swimming-induced rhinitis, at least in competitive athletes.
Our study has some limitations. First, failure to observe significant differences between groups in the other studied outcomes could have been due to insufficient sample size. Second, we were not able to standardize exercise load between swimmers and runners for obvious reasons. We cannot exclude that different volumes and intensities of exercise would have produced different results. Furthermore, generalization of our results is limited by our sample size.
Contrary to the asthma phenotype in swimmers, which seems to be partially dependent on the allergic background of the athlete, 9 swimming-induced rhinitis was independent of atopic status. A similar observation has been reported by Gelardi et al. who suggested a form of nonallergic swimmer rhinitis with prevalent nasal obstruction and neutrophilia, possibly due to chlorine exposure. 4 It is possible that specific mechanisms such as chemical exposure and nasal aspiration of water droplets during training and competition could contribute to nasal dysfunctional response associated with exercise in competitive swimmers compared with runners. Furthermore, this may correspond to a more difficult-to-treat phenotype, because it has been shown that weather- and temperature-sensitive vasomotor rhinitis may be refractory to intranasal corticosteroid use. 5
Contrary to our expectations and challenging current beliefs, atopic athletes experienced an improvement both in nasal flow and symptoms after exercise. Autonomic reflexes usually improve nasal efficiency during exercise reducing nasal resistance compared to normal breathing, due to an increase in nasal sympathetic tone, causing constriction of nasal blood vessels through α-adrenoreceptor stimulation. In contrast, isometric exercises produce little nasal effects in normal subjects, but induce a clear increase of nasal resistance in rhinitis subjects. 10 Although athletes refrained from medication, we cannot rule out delayed effects of antirhinitis drugs on the nasal response to exercise. Further studies on the effect of atopy on the burden of exercise-induced rhinitis will clarify this issue.
The current recommendation to refrain from exercise before FeNO measurements was recently challenged at least for swimming. 11 No immediate or delayed changes in FeNO following two training sessions during one day, independent of the swimmers’ atopic or asthma status occurred. This suggests that the potentially harmful effects of exposure to chlorine derivatives used for swimming pool maintenance are not reflected in acute changes of FeNO. In the present study, runners experienced a significant decrease in levels of FeNO after exercise, which was not observed in swimmers. This effect was independent of changes in lung function, suggesting the existence of a swimming-related factor impairing the normal response to exercise.
Exercise-induced rhinitis in athletes, particularly swimmers, can affect quality of life by interfering with sleep, decreasing the ability to concentrate, or reducing peak physical fitness. Standard diagnosis procedures should include field exercise challenge in the relevant sport environment with specific nasal evaluation. Ideally, as in other occupational diseases, these tests should be performed before therapeutic interventions. In summary, we found that swimmers, contrary to runners, experience a worsening of nasal function after training. Swimmers rhinitis seems to be independent of atopic status. Exposure to aerosolized water droplets and chlorine derivatives may have a role on the incidence of exercise-induced rhinitis.
Footnotes
Acknowledgments
We thank all subjects for their participation and the technical and administrative staff of Futebol Clube do Porto Swimming Section for logistical help. We thank Paulo Colaço and Tiago Jacinto for helping with data collection.