
Abstract
Background
The “Candy Smell Test” (CST) has been introduced as a new testing method for the evaluation of the human sense of smell. In contrast to other established orthonasal smell tests, the CST addresses the retronasal application of odors, typical for food aroma effects during mastication and swallowing. The aim of this study was to evaluate the CST in a clinical setting in patients with olfactory dysfunction and normal controls against the Sniffin’ Sticks test. Furthermore, cutoff points for normal and pathological results in the CST should be determined.
Methods
The olfactory performance of 96 patients presenting with olfactory disorders and 71 healthy controls was evaluated with the CST—comprised of 23 different aromatized smell candies and the extended Sniffin’ Sticks test (threshold, discrimination, and identification). The control group was gender matched but included also younger persons.
Results
The tested subjects could easily understand the procedures and were motivated to participate. The CST correlated well with the Sniffin’ Sticks for all tested subjects and for patients (n = 96) and controls (n = 71). The proposed cutoff value to differentiate normosmia from hyposmia in the CST was a score of <16 (i.e., 16 correctly identified odors) of 23. A score below 13 in the CST was the cutoff value for anosmia.
Conclusion
The CST is an easy-to-handle reliable tool to investigate retronasal olfaction suited for clinical determination of normosmia, hyposmia, and ansomia. In addition, it can be used for investigation where self-application is necessary such as in large survey studies.
Renner et al. 12 introduced a new method for retronasal smell evaluation called the Candy Smell Test (CST). The authors were searching for a way to more easily test children but also adults and claimed that presenting odors in a natural way might increase the motivation to do the testing. To that matter, they presented sorbitol candies that were carrying 23 different aromas. Validating the CST against the full Sniffin’ Sticks test revealed a good correlation (r366 = 0.84) and enabled the separation of normosmic, hyposmic, and anosmic patients. As predicted the patients’ motivation in participating was high. The aim of this study was to evaluate the handling and the accuracy of the CST in a clinical setting, where patients with olfactory dysfunctions and healthy controls underwent the new testing method and compare it with the Sniffin’ Sticks.
Materials and Methods
Participants
The study was conducted at the Department of Otorhinolaryngology, Head and Neck Surgery of the University Medical Center Mainz, Germany. In total, olfaction was investigated in 167 persons. Ninety-six patients presented to the smell clinic with complaints of smell dysfunctions. The patient group consisted of 53 men and 43 women, with an age range of 12–81 years and with a mean age of 50 years. The main causes for a dysosmia were sinonasal (32%), postviral (27%), after head trauma (18%), and idiopathic (15%).
The control group consisted of 43 men and 28 women, age range between 16 and 76 years with a mean age of 36 years; here, individuals were included who were referred to the Outpatient Clinic or were in the ward of our Department for Otolaryngology complaints and reported normal olfaction. Exclusion criteria were rhinologic symptoms or symptoms of chronic rhinosinusitis in the control group and neurodegenerative disorders, oncologic diagnosis, or medications that may influence the sense of smell or taste in both groups. All subjects underwent a complete ear, nose, and throat examination, including nasal endoscopy. They filled out a demographic questionnaire, answered questions about smoking habits, and subjectively assessed their smell ability. Additionally, they underwent a detailed subjective olfactometry of TDI testing (Sniffin’ Sticks test), and afterward the CST. The patients and controls had signed an informed consent before participation in the study. The study was approved by the local Institutional Review Board of the University Mainz, Germany.
Sniffin’ Sticks Test
The Sniffin’ Sticks is a standardized orthonasally conducted olfactory function test 13 widely used in Europe. To date, there are ∼150 publications based on this test. It includes a 16-step n-butanol threshold test, a 16 odorant pairs discrimination test, and a 16 item odor identification test. Because the maximum score for each subtest is 16, the maximum composite score (TDI) is 48. The TDI score allows a classification of olfactory function as normosmic, hyposmic, or functional anosmic. 14 Recently, a study with a larger number of healthy individuals (>3000) was published with updated gender- and age-adapted normative values. 15
Candy Smell Test
The candies were industrially manufactured and all had the same size (0.9-cm diameter x 0.5-cm height) and texture. The fare material was 500 mg of sorbitol, which has a sweet flavor (60% of the sweetening capacity of sucrose) and is odorless. The smell candies have been described in detail in an article by Renner and coworkers. 12 It is a three-alternative forced-choice identification test. Twenty-three candies containing different odors were used sequentially by the participants that picked the candy from a flask and put it into the mouth like you would do in everyday practice. However, they were instructed not to sniff the candy before insertion into the mouth or to chew it afterward. While having the candy still in the mouth and using it as they would do with every other candy as well, they had to choose one of a set of four pictures of different items characterizing a specific odor, such as an apple or an orange as possible answers. There was no feedback to the subject whether their responses were correct or incorrect. After choosing one picture, subjects disposed of the candy and rinsed their mouths with water. Each correct answer was given 1 point, the total number of points was recorded as the CST score with a maximum of 23 points (equal to possible correct identifications).
Statistics
All statistical analyses were performed using SPSS .16.0 statistical software (SPSS, Inc., Chicago, IL). Spearman's ρ correlation analysis was performed to detect correlations between different parameters. All analyses were regarded as explorative. Consequently, all p values were given descriptively and a significance level was not fixed. For graphical demonstrations, box plots and scatter plots were used. The receiver operating characteristic curve (ROC) was exploited to be able to determine the sensitivity and specificity of different cutoff values for the CST.
Multivariate logistic regression modeling was performed to analyze the prognostic value of the parameters age, gender, and smoking in the CST performance. Therefore, subjects were classified into two groups (normosmic dysfunction versus olfactory dysfunction) using published TDI limits. 15 Additionally, cutoff points of the CST scores for hyposmia and anosmia were calculated.
Results
Test Subjects
In terms of gender no statistical difference could be detected between the two groups of subjects (p = 0.53, Fisher's exact test), but the subjects in the control group were younger (p < 0.01, unpaired t-test). Table 1 shows a description of the demographic data.
Demographic data of patients and healthy controls ± standard error of mean

Sniffin’ Sticks Results
The results of the Sniffin’ Sticks test (TDI score) were used as normative data. 15 Based on these results, individuals were allocated to one of the following age- and gender-adapted groups: normosmic, hyposmic, and functional anosmic. The mean TDI score in the patient group was 16.2, whereas the control group showed a normal olfactory performance with a mean TDI score of 33.2. The distribution of normosmia, hyposmia, and functional anosmia in the different groups is shown in Table 2.
Distribution of normosmia, hyposmia, and anosmia determined by the age- and gender-adapted threshold, discrimination, and identification (TDI) scores 15 ) and the number of correctly identified items in the Candy Smell Test (CST) in the patient group and the control group ± standard error of mean

CST Procedure
The duration of the CST was between 15 and 30 minutes. In the correlation analysis (Spearman's ρ) a negative correlation between the number of correctly identified candies and the answering time has been found (r = 0.636; p < 0.01). The handling of the CST was uncomplicated and the tested individuals had no problems understanding the instructions and seemed to be highly motivated to complete the testing. No adverse events occurred.
CST Results
Individuals with hyposmic or functional anosmic results in the Sniffin’ Sticks test also reached lower scores in the CST. Results of male and female participants showed no statistical difference in either group. A multivariable logistic regression analysis was performed with the diagnostic group (normosmic/olfactory dysfunction) after Sniffin’ Sticks testing as the primary outcome of interest. Only the subjective self-assessment (p < 0.001) and the CST result (p < 0.001) were relevant predictors for the diagnostic group.
Other variables, including age, gender, and smoking habits were not variables with prognostic relevance in the model (all p ≥ 0.35). The odds ratio for the CST result and the subjective estimation was 0.75 (CI, 0.63–0.88), and 24.58 (CI, 5.76–105.00), respectively.
Correlation between the Two Tests
Regarding the whole group of 167 individuals, the correlation coefficient (Spearman's ρ) between the TDI score and the number of correct answers in the CST was 0.84 (p < 0.01). In both subgroups (patients and controls) the correlation was also noticeable (p < 0.01), with a correlation coefficient of 0.60 and 0.46, respectively (Fig. 1).
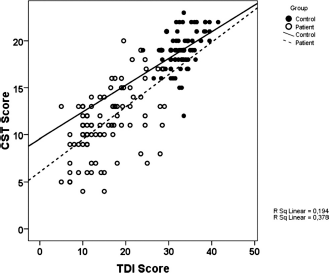
Correlation of the Candy Smell Test (CST) score and the threshold, discrimination, and identification (TDI) score split for the patient group and the control group including fitting lines for the control (continuous) and the patient group (dashed).
The correlations (Spearman's ρ) between the CST and the subtests of the Sniffin’ Sticks were as follows: CST and Sniffin’ Sticks threshold test, 0.796 (p < 0.01); CST and Sniffin’ Sticks discrimination test, 0.754 (p < 0.01); CST and Sniffin. Sticks identification test, 0.811 (p < 0.01). The scatter graph of the correlation of the Sniffin’ Sticks identification test and the CST is shown in Fig. 2.
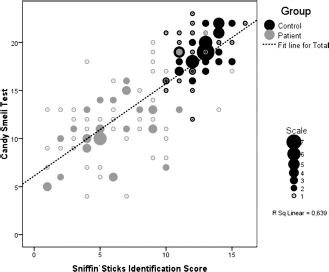
Correlation of the Candy Smell Test (CST) score and the Sniffin’ Sticks identification score. Scaled dots represent the control (black) and the patient group (gray).
CST Scores and Sniffin’ Sticks Classifications
The distribution of CST results based on the Sniffin’ Sticks test results of normsomia, hyposmia, and anosmia (after 15 ) is shown in Fig. 3. The differences between the three groups were prominent (p < 0.001, Kruskal-Wallis test). Subjects who were found to be functional anosmic in the Sniffin’ Sticks test (TDI < 16) scored between 4 and 14 in the CST (n = 52; median, 10; SD = 2.74); 75% scored in the range of 6–12 points. The multivariable logistic analysis revealed a CST value of 15.2 as a cutoff point for the probability of a pathological finding (hyposmia or anosmia in the Sniffin’ Sticks test).
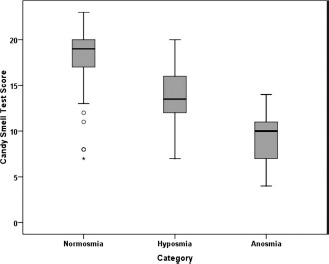
Box whisker plot of Candy Smell Test (CST) scores according to the diagnostic group including all participants (n = 167; normosmia, hyposmia, and anosmia derived from gender and age-adapted Sniffin’ Sticks [threshold, discrimination, and identification {TDI} score] results referring to the study by Hummel et al. 15 ). The lines represent the medians; the boxes include 75% of the results; the whiskers include 95%.
ROC Curve
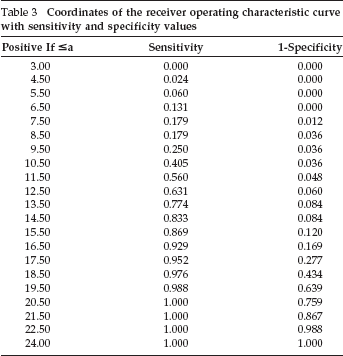
The ROC curve is shown in Fig. 4. The area under the curve was 0.925 (p < 0.01). The table of the curve coordinates for calculating sensitivity and specificity is shown in Table 3.

Receiver operating characteristic (ROC) curve of Candy Smell Test (CST) results.
Coordinates of the receiver operating characteristic curve with sensitivity and specificity values
Discussion
In this study we showed that the CST is an instrument that can be used to assess a subject's retronasal smell perception in patients with olfactory impairment and in healthy controls. The comparison with Sniffin’ Sticks revealed good correspondence with a correlation coefficient of r = 0.84. Hence, our study could replicate previous findings of the article that introduced the CST. 12 In our study, both groups (patients and controls) showed a consistent correlation between the CST and Sniffin Sticks (r = 0.60 and r = 0.46, respectively). Because the CST is an identification test, it was not surprising that it correlated best with the Sniffin’ Sticks identification test (r = 0.81, see Fig. 2).
The multivariable logistic analysis revealed a cutoff point in the CST for a normal performance a value of >15.2. Therefore, if a person reaches scores ≥16 in the CST, an olfactory impairment can be ruled out with high probability. The cutoff point to differentiate between hyposmia and anosmia could be defined as CST scores lower than 13 because only 6% of the anosmics reached higher values in the CST (14 or 15 correct items). A cutoff point for anosmia of 13 items in the CST was also proposed by Renner et al. 12
The ROC curve is a marker for the quality of the new test compared with a standardized method. In the present study, the ROC curve of the study population revealed that the CST was a very good indicator to differentiate between normal and pathological results, suggesting a cutoff point of 16 correct answers with a sensitivity of 87% and a specificity of 88%. A higher value of 17 correctly identified items would lead to an increase of sensitivity to 93% but also to a decrease of specificity to 83%, which meant a much higher number of false positive results. Therefore, previously proposed cutoff limits for the CST (≤16) to differentiate between normosmia and dysosmia by Renner et al. 12 were also valid in this study.
In contrast to the same previous report, 12 we were not able to detect differences of age or gender using the CST performance. This might be because of the lower number of normosmic individuals with a lower mean age investigated in our actual study.
The CST is a new approach for assessing retronasal olfaction in different pathologies. There are numerous publications on differences in orthonasal and retronasal olfactory performance after mechanical obstruction of the anterior olfactory cleft, 7 which might be the leading cause for reduced olfaction in patients with nasal polyposis. 16 But also in subjects with other causes for impaired olfaction (posttraumatic, idiopathic, and after upper respiratory tract infection), significant differences in the psychophysical and electrophysiological testing of olfaction could be established in some cases. 6
In a study by Heilmann et al., 17 a similar technique using 20 different powders that were applied to the mouth has been described. The authors compared the retronasal performance to the standard orthonasal Sniffin’ Sticks test and found a significant effect of gender in the retronasal testing, with women reaching higher scores than men. In addition, there was a trend for their scores to decline with increased age. The identification scores correlated quite well (r = 0.78) with orthonasal testing. The powders that were used for retronasal presentation were all commercially available in grocery stores or from food companies. Because the test needs to be prepared by the individual investigator, there is the chance of variance due to lack of controlled procedures. The CST would provide a more standardized stimulation method that might result in a more reliable differentiation between normal and pathological olfactory perception (see ROC curve in Fig. 3).
In a clinical application in patients with decreased olfaction due to a nasal polyposis, the comparison between the two presentation methods showed a significantly better retronasal than orthonasal perception of odorants. 16 Because of the limited number of subjects in our study we found no differences in the CST results of patients with different causes for olfactory impairment.
Conclusion
In conclusion, the CST is a reliable method for assessing human retronasal olfaction with good correlation to an established orthonasal testing method. Limits for hyposmia and functional anosmia have been determined and therefore the CST could be used as a reliable screening method. Furthermore, this test could be a new approach to measure retronasal smelling deficits in humans with different pathologies.