
Abstract
Background
Methotrexate (MTX) is a very effective treatment for chronic inflammatory diseases, which are often associated with increased angiogenesis. Angiogenesis is dependent on a perfectly coordinated balance between endogenous-positive and -negative regulatory factors, including vascular endothelial growth factor (VEGF) and the angiopoietins (Ang). The aim of this study was to investigate the effects of MTX on levels of VEGF, Ang-1, and Ang-2 in organ-cultured nasal polyps (NPs.
Methods
To determine the effects of MTX, NP tissues were cultured using an air-liquid interface method. Cultures were maintained in the absence or presence of MTX (10 or 100 micromoles) for 24 hours. Hematoxylin and eosin, and TUNEL (terminal deoxynucleotidyl transferase [Tdt]-mediated dUTP-biotin nick-end labeling) staining were performed to observe apoptosis. Enzyme-linked immunosorbent assay was used to quantify tissue concentrations of VEGF, Ang-1, and Ang-2.
Results
MTX treatment resulted in marked alterations in inflammatory cells, especially eosinophils. In contrast, the mucosal epithelium, microvessels including arterioles, veins and capillaries, and fibroblasts maintained their structure. TUNEL+ cells (apoptotic cells) were seen in the MTX-treated specimens. The more induction of TUNEL+ cells was observed 100-micromolar MTX-treated specimens. VEGF and Ang-1 levels were significantly lower, and Ang-2 levels were significantly higher in NPs treated with 100-micromolar MTX than in nontreated NPs (p < 0.01.
Conclusion
MTX may inhibit the growth of NPs via local regulation of VEGF, Ang-1, and Ang-2 protein levels. We suggest that MTX can be used to treat NPs.
Long-term therapy with potent intranasal glucocorticoids is widely advocated to control NP inflammation and growth. However, the response to this treatment is often only partially successful, 9 and additional therapies are needed to treat glucocorticoid-resistant NPs.
Methotrexate (MTX), which is used at low dosages to treat a variety of chronic inflammatory diseases, has been proposed to have steroid-sparing effects in steroid-dependent asthmatic patients. 10 The mechanism of action of MTX as an anti-inflammatory or antiangiogenic drug is not fully understood. Angiogenic factors play significant roles in the regulation of capillary and basilar membrane permeability in NPs.11–13 However, nothing is known about the effects of MTX on angiogenesis in NPs. In this study, we evaluated the effects of MTX on the expression of VEGF, Ang-1, and Ang-2 in NP using an air-liquid interface organ culture model.
Materials and Methods
NP Tissues
Twelve subjects with NPs were recruited at the Department of Otorhinolaryngology, Inje University Busan Paik Hospital, Busan, Korea. Informed consent was obtained from each patient, and the study was approved by the local ethics committee. Individuals were diagnosed with NPs based on the minimal criteria for chronic rhinosinusitis with NPs. 14 NPs were removed from the middle meatus at the beginning of the surgical procedure. No patients had been treated with steroids (systemic or topical), nonsteroidal anti-inflammatory drugs, antihistamines, or macrolide antibiotics during the 4 weeks before biopsy.
Organ Culture of NPs
Twelve NPs were cut, using blades, into 2- to 3-mm3 pieces under sterile conditions. Tissue fragments were washed three times with phosphate-buffered saline (PBS) containing an antimycotic (5 μg/mL of fungizone) and an antibiotic (300 μg/mL of penicillin G) and then rinsed with 98% Dulbecco's minimum essential medium (DMEM) supplemented with calf serum (10%) and gentamicin (20 μg/mL). To determine the effects of MTX treatment on NPs, tissues were next saturated for 1 hour in culture medium (DMEM + 10% calf serum + 10 μg/mL of gentamicin) in the presence or absence of MTX (10 or 100 μM). Tissue fragments were then placed on hydrated 1 x 1-cm gelatin sponges (Spongostan; Johnson & Johnson, San Angelo, TX) with the mucosa facing upward and the submucosa facing downward. Each sponge was placed in a well of a 6-well plate containing 3 mL of culture medium so that the mucosa was above the liquid phase. The plates were then placed in a humidified incubator and maintained at 37°C in a 95% air/5% CO2 atmosphere under continuous shaking at 15 rpm for 24 hours. Where specified, MTX (10 or 100 μM) was added to culture medium. Subjects were divided into four groups: (1) fresh (control, NPs were saturated for 1 hour in culture medium, but not organ culture); (2) nontreated (NPs were saturated for 1 hour in culture medium and then organ cultured for 24 hours in culture medium); (3) 10 μM of MTX treatment (NPs were saturated for 1 hour in culture medium containing 10 μM of MTX and then organ cultured for 24 hours in culture medium containing 10 μM MTX); and (4) 100 μM MTX treatment (NPs were saturated for 1 hour in culture medium containing 100 μM of MTX and then organ cultured for 24 hours in culture medium containing 100 μM MTX).
Histological Analysis
Tissue fragments were fixed in 2% phosphate-buffered paraformaldehyde and embedded in paraffin. They were then sectioned to a thickness of 5 μm and stained with hematoxylin and eosin.
Cryosectioned tissues were stained using a TUNEL (terminal deoxynucleotidyl transferase [Tdt]-mediated dUTP-biotin nick-end labeling) kit (Merck, Darmstadt, Germany) for apoptotic cells. Briefly, specimens were air-dried and fixed in 1% paraformaldehyde for 10 minutes and then postfixed in ethanol/acetic acid (2:1) for 5 minutes. After quenching any endogenous peroxidase with 3% hydrogen peroxide (Fluka Chemie AG, Buchs, Switzerland) for 5 minutes, the sections were reacted using the Apoptag kit (Merck). Sections were washed and then visualized using diaminobenzidine tetrahydrochloride (Sigma, St. Louis, MO) and 0.03% H2O2 in PBS (0.05 M, pH 7.4).
Enzyme-Linked Immunosorbent Assay
Tissue samples were chopped with scissors and crushed in tissue lysis buffer containing a proteinase inhibitor. The lysates were centrifuged, and total protein concentration in each supernatant was measured using Bio-Rad Protein Assay Dye Reagent (Bio-Rad, Hercules, CA). Supernatant concentrations of VEGF, Ang-1, and Ang-2 were determined using a DuoSet ELISA Development System (R&D Systems, Minneapolis, MN) according to the manufacturer's instructions. Each 96-well microtiter plate, precoated with a monoclonal antibody raised to one of the antigens, was incubated with blocking buffer (1% bovine serum albumin, 5% sucrose, and 0.05% NaN3 in PBS) for 1 hour at room temperature to minimize nonspecific antibody binding. Protein standards and supernatants were added to individual wells, and the plates were incubated for 2 hours at room temperature. The samples were then aspirated, and the plates were washed three times with buffer. Biotinylated secondary antibody was added, and the plates were incubated for 2 hours. After aspiration/washing, the plates were incubated with streptavidin–horseradish peroxidase and substrate solution for 20 minutes each. The reaction was stopped, and absorbance at 450 nm was measured within 30 minutes.
Standard curves were constructed using the concentrations of each antigen (which ranged from 0 to 3–8 ng/mL), and these curves were then used to convert the absorbance value obtained from each well to a concentration (ng/mL) of growth factor. Total protein concentrations were also calculated using a standard curve. Data (ng of protein/mg of total protein) are presented as the mean ± SEM.
Statistical Analysis
Results are expressed as the mean ± SEM. Statistically significant differences were identified by ANOVA with correction for multiple comparisons using SPSS software Version 11.0.0 (SPSS, Inc., Chicago, IL; *p < 0.05 and **p < 0.01).
Results
Histological Analysis
MTX treatment resulted in marked alterations in inflammatory cells, especially eosinophils. In contrast, the mucosal epithelium, microvessels including arterioles, veins and capillaries, and fibroblasts maintained their structure (Fig. 1).
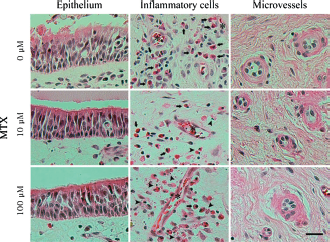
Methotrexate (MTX) treatment resulted in marked alteration of inflammatory cells, especially eosinophils (arrow). Apoptotic eosinophils (arrowhead) were frequently increased around capillaries (asterisk). However, mucosal epithelium, microvessels such as arterioles, veins, and capillaries and fibroblasts maintained their structure (scale bar = 100 μm).
TUNEL+ cells (apoptotic cells) were seen in the MTX-treated specimens. More induction of TUNEL+ cells was observed in the 100-μM MTX-treated specimens (Fig. 2).
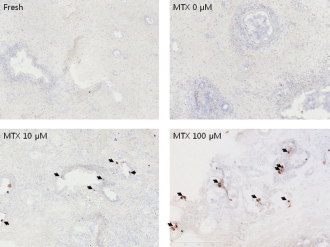
TUNEL (terminal deoxynucleotidyl transferase [Tdt]-mediated dUTP-biotin nick-end labeling) staining of apoptotic cells visualized with diaminobenzidine tetrahydrochloride (DAB; brown color) in nasal polyp specimens. TUNEL+ cells (apoptotic cells) were seen in the methotrexate (MTX)-treated specimens (brown color, arrows). More induction of TUNEL+ cells was observed in 100-μM MTX-treated specimens.
Expression of VEGF, Ang-1, and Ang-2 in Organ-Cultured NPs
VEGF, Ang-1, and Ang-2 levels before and after the 24-hour application of MTX (10 or 100 μM) were measured by ELISA (Table 1). VEGF levels were significantly lower in 100-μM MTX-treated polyps than in nontreated polyps. Ang-1 levels were also significantly lower in 100-μM MTX-treated polyps than in nontreated polyps. In contrast, Ang-2 levels were significantly higher in 100-μM MTX-treated polyps than in nontreated polyps (Fig. 3).
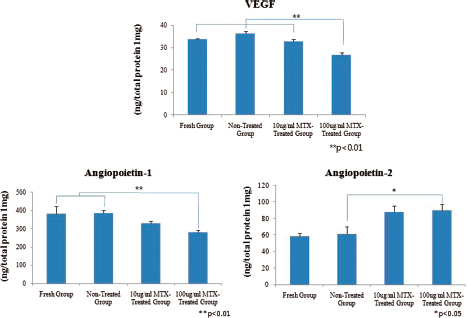
Enzyme-linked immunosorbent assay (ELISA) measurement; concentrations of vascular endothelial growth factor (VEGF), angiopoietin 1, and angiopoietin 2 in the fresh, nontreated group, 10-μM methotrexate (MTX)-treated group, and 100-μM MTX-treated group (n = 12 for each group). The concentration of protein was calculated by using a standard curve run together with known concentrations. Data were presented as mean ± SEM nanograms of protein normalized to 1 mg of total protein.
Concentrations of vascular endothelial growth factor (VEGF), angiopoietins Ang-1, and Ang-2 in nasal polyps before and after methotrexate treatment (mean ± SEM, values reported as ng/mg)
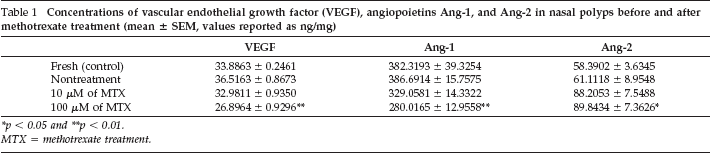
p < 0.05
p < 0.01.
MTX = methotrexate treatment.
Levels of VEGF and Ang-1 tended to be lower in 10-μM MTX-treated polyps than in nontreated polyps, and Ang-2 levels were higher in 10-μM MTX-treated polyps than in nontreated polyps. However, these differences were not statistically significant.
Discussion
NPs are a chronic inflammatory disease of the nasal mucosa characterized by infiltration of inflammatory cells, especially eosinophils, and tissue remodeling, which includes basement membrane thickening, extracellular matrix accumulation, and fibrosis. Angiogenesis and microvascular remodeling are elements of the tissue remodeling in chronic inflammatory diseases. 15 Angiogenesis is dependent on a perfectly coordinated balance between endogenous-positive and -negative regulatory factors, including VEGF and the Ang's. 16 In a previous study, we showed that VEGF and Ang-1 levels were significantly higher and Ang-2 levels were significantly lower in NPs than in inferior turbinates. 12 Based on these observations, we suggested that VEGF and Ang-1 act as positive regulators of angiogenesis in NPs, and Ang-2 is an inhibitor.
MTX is a very effective treatment for chronic inflammatory diseases such as psoriasis, rheumatoid arthritis, ulcerative colitis, and asthma.17–19 Its mode of action in these conditions has not been fully elucidated, although several mechanisms have been postulated. MTX is a potent inhibitor of the enzyme dihydrofolate reductase, leading to the inhibition of purine and pyrimidine synthesis and reduced T-cell proliferation. Additionally, it is believed that the anti-inflammatory action of MTX stems from the extracellular accumulation of adenosine, which acts as an endogenous anti-inflammatory agent. Adenosine binds to specific adenosine receptors and inhibits lymphocyte proliferation as well as the production of the proinflammatory cytokines TNF-α, IL-6, and IL-8, while stimulating transcription of the gene encoding IL-1 receptor antagonist and the production of IL-10.20,21 Low-dose MTX reportedly plays a role in antiangiogenesis for the synovial blood vessels in rheumatoid arthritis. 22 Recently, Buyukozturk et al. 23 described two patients with steroid-dependent asthma whose NPs dramatically decreased in size after a course of MTX therapy, administered as an auxiliary treatment. However, the precise mechanism involved was not determined. In our previous study, 12 we found that dexamethasone, at a concentration of 100 μM, significantly decreased VEGF and Ang-1 levels in NPs while significantly increasing Ang-2 levels. In the present study, 100 μM of MTX similarly reduced NP levels of VEGF and Ang-1 and increased Ang-2 levels. It also resulted in marked alterations in inflammatory cells, especially eosinophils. However, the mucosal epithelium, microvessels, and fibroblasts maintained their structure. TUNEL+ cells (apoptotic cells) were seen in the MTX-treated specimens. More induction of TUNEL+ cells was observed in 100-μM MTX-treated specimens. Overall, our results suggest that MTX may inhibit the growth of NPs via the local regulation of VEGF, Ang-1, and Ang-2 levels.
Conclusion
MTX may inhibit the growth of NPs via local regulation of VEGF, Ang-1, and Ang-2 protein levels, leading to decreased VEGF and Ang-1 activity and increased Ang-2 activity. We suggest that MTX can be used to treat NPs.