
Abstract
Background
Although both nasal steroids and macrolide antibiotics have been recommended for the treatment of chronic rhinosinusitis without nasal polyps (CRSsNPs), whether there is any difference in their clinical efficacy remains unexplored. In addition, few studies have investigated their clinical efficacy in a Chinese population living in China, who present distinct inflammatory patterns compared with white patients in western countries. This study compares the efficacy of mometasone furoate and clarithromycin treatment in CRSsNP in Chinese adults in a preliminary prospective, open-label, randomized trial.
Methods
Forty-three CRSsNP patients were randomized to receive mometasone furoate nasal spray at 200 μg (n = 21) or clarithromycin tablet at 250 mg (n = 22) once daily for 12 weeks. Patients were assessed before the treatment and after 4, 8, and 12 weeks after treatment. Subjective symptoms were scored on a visual analog scale. Endoscopy physical findings were scored according to Lanza-Kennedy scoring system. Moreover, smoking and atopic status and coexistence of allergic rhinitis (AR) and asthma were recorded.
Results
Before the treatment, no significant difference in symptoms and nasal endoscopic physical findings were found between mometasone furoate and clarithromycin group. As early as 4 weeks after dosing, a significant reduction of total symptom scores, nasal obstruction, headache, rhinorrhea and overall burden scores, and mucosal swelling and nasal discharge scores were observed in both groups. No significant difference in symptom or endoscopic scores was observed between these two groups at any posttreatment observation time point. The coexistence of AR was correlated with lower scores of mucosal edema and nasal secretion in the mometasone furoate group after 12-week treatment.
Conclusion
Mometasone furoate and clarithromycin show a comparable clinical effect for CRSsNPs in Chinese adults. Mometasone furoate is more effective in improving edema and secretion for CRSsNP patients with concomitant AR.
Recently, a large body of evidence has emerged to suggest that 14- and 15-membered ring macrolide antibiotics have intrinsic anti-inflammatory properties in addition to their well-established antibiotic effect.3,4 Macrolides have been shown to inhibit the production of several inflammatory cytokines, diminish the formation of pseudomonal biofilms, decrease airway mucus secretion, block the activation of the transcription factor nuclear factor κB (NF-κB), and induce the apoptosis of neutrophils.3,4 Clinical studies suggest that long-term, low-dose administration of macrolides is effective in the treatment of CRS, 3 – 6 particularly for those with higher interleukin (IL)-8 and lower IgE levels,3–6 indicating that the effect of macrolides may mediate through inhibiting neutrophilic inflammation. Glucocorticoids are potent immunosuppressive agents with complex actions on immune cells. 7 Glucocorticoids can block the activation of various transcription factors including NF-κB, activator protein 1, and anti-interferon regulatory factor 3; reduce the synthesis and release of both Th1 and Th2 cytokines 8 ; and inhibit inflammatory cell migration. 9 In addition, glucocorticoids can delay neutrophils apoptosis and shift neutrophils to a necrosis during inflammation. 10 Several studies have suggested a clinical benefit of nasal glucocorticoids in the treatment of CRSsNPs. 11
Currently, both nasal glucocorticoids and macrolide antibiotics have been recommended for the treatment of CRSsNPs by the European Position Paper on Rhinosinusitis and Nasal Polyposis. 1 CRSsNPs presents a Th1-predominant and neutrophil-biased inflammatory pattern. 12 Although glucocorticoids and macrolides share some similarities in their pharmacologic actions and a recent ex vivo study has indicated that clarithromycin is as potent as prednisone to inhibit the production of IL-5, IL-8, and granulocyte-macrophage colony-stimulating factor in sinonasal mucosa from CRSsNP patients, 13 there are clear differences between these two agents. Whether these two agents have comparable clinical efficacy in the treatment of CRSsNPs is unclear. Moreover, few studies have investigated the clinical efficacy of these two medicines in a Chinese population living in China, although recent studies have indicated distinct inflammatory patterns between these Chinese and white patients in western countries, e.g., increased expression of Th17 transcription factor and cytokines including retinoic-acid related orphan receptor C, IL-17A, IL-22, and IL-23, which suggests an enhanced Th17 response, is found in both CRSsNPs and CRSwNPs in Chinese patients but not in white patients; in addition, over one-half of Chinese patients with CRSwNPs present noneosinophilic inflammation, whereas most white patients with CRSwNPs present Th2-dominated eosinophilic inflammation. 12,14 In this study, we compared the clinical efficacy of mometasone furoate nasal spray versus clarithromycin tablet in the treatment for CRSsNPs in Chinese adults in a preliminary prospective, open-label, randomized trial.
Methods
Patients
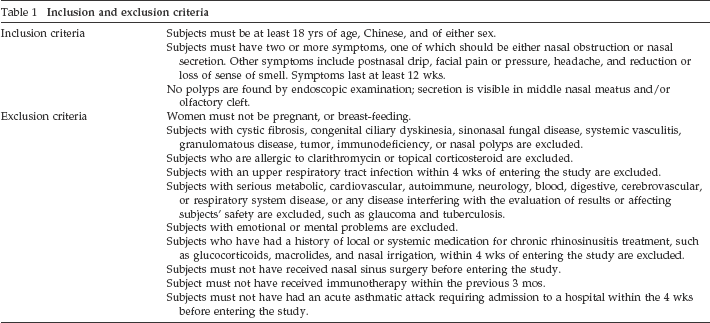
Forty-three patients were recruited from January 2009 to June 2010 at our department. Patients were eligible for the inclusion in the study if they were aged ≥18 years, in good health, had CRSsNPs, and were free of diseases that would interfere with the study (Table 1). The diagnosis of CRSsNPs was made according to the European Position Paper on Rhinosinusitis and Nasal Polyposis 2007 and American guidelines,1,2 which is based on clinical history, anterior rhinoscopy, and nasal endoscopy (Table 1). None had previous sinus surgery. Patients were included only if none of the exclusion criteria were present (Table 1). Atopic status was evaluated using the ImmunoCAP Phadiatop test (Phadia, Uppsala, Sweden), detecting IgE antibodies against various common inhalant allergens (birch, timothy grass, mugwort, olive, cat, dog, horse, Dermatophagoides pteronyssinus and Dermatophagoides farinae, Cladosporium herbarum, and Parietariajuclacia). The diagnosis of allergic rhinitis (AR) was based on the concordance between a typical history of allergic symptoms and the Phadiatop test. The diagnosis of asthma was based on history and chest physicians’ diagnosis according to the Global Initiative for Asthma 2006 guidelines. 15 This study was approved by the Ethics Committee of Tongji Medical College of Huazhong University of Science and Technology, and conducted with written informed consents from patients.
Inclusion and exclusion criteria
Randomization and Study Scheme
After recruitment into the study, subjects were randomly assigned to mometasone furoate or clarithromycin group using a random number table. In the mometasone furoate group, patients were given mometasone furoate nasal spray (Schering-Plough China, Shanghai, China), 200 μg once daily for 12 weeks. In the clarithromycin group, patients received 250-mg tablets of clarithromycin (Abbot China, Shanghai, China) once daily for 12 weeks. During the study, patients did not receive other additional treatments.
Outcome Measures
All of the patients were assessed by symptom questionnaire and endoscopy after enrollment and at follow-up visits. Follow-up visits were scheduled for 4, 8, and 12 weeks after dosing.
Subjective symptoms were scored on a visual analog scale (VAS) of 0–10, with 0 being “no complaints whatsoever” and 10 being “worst imaginable complaints.” Five major symptoms were focused on: nasal obstruction, rhinorrhea, loss of sense of smell, facial pain or pressure, and headache. A total VAS symptom score (combined symptom score) was calculated based on the sum of these five VAS symptom domains. In addition, patients were asked to rate his/her overall burden of CRS symptoms on a VAS of 0–10 as mentioned previously.
The nasal cavities were examined with a nasal endoscope by the senior investigator (ZL), who was blinded to the treatment. The presence or absence of discharge and swelling, particularly in the middle meatus and olfactory cleft, was noted. Endoscopic scoring was performed according to Lanza-Kennedy (discharge: 0, no discharge; 1, clear thin discharge; 2, thick purulent discharge; swelling: 0, no swelling; 1, mild swelling; 2, severe swelling). 16 Each side was graded separately, and the scores from each side were then added to determine the overall endoscopic score.
The primary efficacy measure was the total symptom VAS scores (combined symptom scores). Secondary analyses were performed on individual symptoms scores, overall burden scores, and endoscopy scores.
Statistical Analysis
The statistical analysis of efficacy was based on all randomized subjects in this study. Statistical analyses were performed with SPSS for Windows, Version 13.0 (SPSS, Inc., Chicago, IL). Data are expressed as means ± SD. The t-test was used to compare baseline values between groups. Changes in clinical parameters were evaluated by repeated-measures ANOVA analyses. Multiple linear regression analysis was used for multivariate analysis. Values of p < 0.05 were considered as statistically significant differences.
Results
Subjects
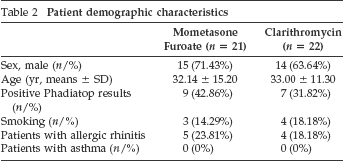
Forty-three patients met the study eligibility criteria and were randomized to receive mometasone furoate nasal spray (n = 21) or clarithromycin tablet (n = 22). None of the patients withdrew from the study. No significant differences were identified between mometasone furoate and clarithromycin group in terms of age, gender, atopic and smoking status, and AR and asthma comorbidity (Table 2).
Patient demographic characteristics
Symptom Outcome
Overall, symptom severity did not differ significantly at pretreatment baseline between the mometasone furoate and clarithromycin groups (Table 3). As early as 4 weeks after dosing, a significant reduction of total symptom VAS scores, nasal obstruction, headache, rhinorrhea, and overall burden scores was observed in both groups compared with the baseline values (Table 3). A significant maximal reduction in total scores, nasal obstruction, nasal secretion, and overall burden scores during the study period was found after 12 weeks of treatment in the clarithromycin group (Table 3). In the mometasone furoate group, although these parameters improved gradually with time of treatment, there was no significant difference between 8-week and 12-week treatment (Table 3). No significant improvement of facial pain was found in either group and a significant improvement of olfactory function was only observed in the mometasone furoate group at the 4-week treatment time point, despite that their scores decreased after treatment (Table 3). No significant difference in total symptom scores, individual symptom scores, or overall burden scores was discovered between these two groups at any follow-up visit (Table 3).
Changes in symptom scores (means ± SD/mean percent change from baseline)
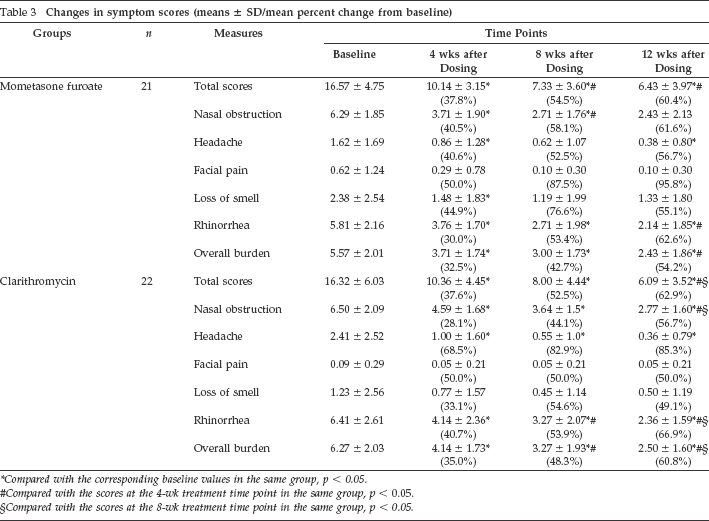
Compared with the corresponding baseline values in the same group, p < 0.05.
Compared with the scores at the 4-wk treatment time point in the same group, p < 0.05.
Compared with the scores at the 8-wk treatment time point in the same group, p < 0.05.
Endoscopy Outcome
The pretreatment baseline scores of mucosal swelling and nasal discharge determined by endoscopy did not show a significant difference between the mometasone furoate and clarithromycin groups (Table 4). Similar to the changes of symptom scores, a significant decrease of mucosal swelling and nasal discharge scores were revealed in both groups as early as 4 weeks after dosing in comparison with the baseline values (Table 4). Although these endoscopy scores tended to decrease gradually with time of treatment, no significant difference was found between the 8-week and 12-week treatment in either group (Table 4). In line with the changes of symptom scores, no significant difference in endoscopy scores was revealed between these two groups at any follow-up visit (Table 4).
Changes in endoscopy scores (means ± SD/mean percent change from baseline)
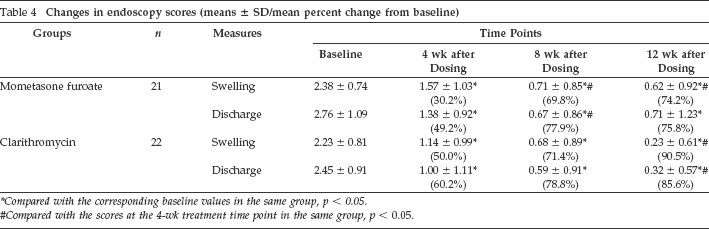
Compared with the corresponding baseline values in the same group, p < 0.05.
Compared with the scores at the 4-wk treatment time point in the same group, p < 0.05.
Analysis of Factors Affecting the Therapeutic Effect
Multiple linear regression analysis was used to study the influence of potential confounding factors on the total symptom VAS scores, overall burden scores, and endoscopy scores after 12 weeks of treatment in both groups, which included gender, age, atopy, AR, and smoking status. The results showed that the mucosal swelling and nasal discharge scores determined by endoscopy at the time point of the 12-week treatment were negatively correlated with the coexistence of AR in the mometasone furoate group (regression coefficient B = -1.195 and -1.497 for mucosal swelling and nasal discharge, respectively; p < 0.05 for both), whereas no factor influencing the clinical efficacy was identified in the clarithromycin group.
Discussion
Although nasal corticosteroids and 14- or 15-membered ring macrolide antibiotics have been recommended as a main anti-inflammatory treatment for CRSsNP patients before and after surgery, whether they possess a similar clinical effect is unknown. To the best of our knowledge, this is the first study comparing the clinical efficacy of nasal glucocorticoids and macrolides in the treatment of CRSsNPs. We have shown that both mometasone furoate nasal spray (200 μg once daily for 12 weeks) and clarithromycin tablets (250 mg once daily for 12 weeks) are capable of producing significant improvements in a range of subjective and objective outcome measures and there is no significant difference between these two treatments.
The principal efficacy measure used in this study was the combined symptom scores, which reflects the fact that CRS is defined clinically by the presence of a cluster of symptoms, rather than by any single symptom. Our study discovered that both mometasone furoate and clarithromycin with a period of 3-month treatment could significantly improve combined symptom scores, indicating that both treatments can produce clinical meaningful symptom relief. Moreover, two major symptoms of CRS (nasal obstruction and rhinorrhea) and overall symptom burden, as well as mucosa swelling and secretion were also improved markedly in both groups, further supporting the clinical benefit of mometasone furoate and clarithromycin. These findings are consistent with the previous reports. 17 However, neither mometasone furoate nor clarithromycin showed a statistically significant effect on olfactory dysfunction and facial pain despite that their scores decreased after treatment. This may be caused by the mild levels of these two symptoms at baseline and the small sample size of this study. While using the Sniffin’ sticks olfactory function test, Wallwork et al. also failed to find a significant improvement of olfactory function after 3 months of treatment with roxithromycin. 18 Interestingly and importantly, in this study, we found no significant difference in therapeutic efficacy at any posttreatment observation time point between mometasone furoate and clarithromycin. In our study, both treatments showed significant clinical effects as early as 4 weeks after dosing. However, in Wallwork's study, patients receiving roxithromycin only reported significant improvements in the linear rating scale after a 12-week course, but not after a 6-week course. Nevertheless, we did find that the efficacy of clarithromycin, but not mometasone furoate, on the relief of symptoms reached maximum significance after a 12-week treatment during the study period, suggesting that a long-duration therapy is needed to achieve the best results for macrolides. As to the changes of endoscopic signs, the effect of clarithromycin did not increase significantly with time of treatment. It is not surprising, because a lot of studies indicate that the symptoms and endoscopy and computer tomography findings are not always in concordance with each other. 19 Although macrolides and glucocorticoids have different anti-inflammatory actions, they do share some similarities, such as inhibiting the activation of NF-κB. NF-κB is a key proinflammatory transcription factor and mediates the production of many proinflammatory mediators involved in both neutrophilic and eosinophilic inflammation, such as IL-5 and IL-8. These similarities may underlie the comparable clinical effect of these two agents in the treatment of CRSsNPs.
To further study the factors influencing the response to these two managements, multiple linear regression analysis was performed. Among all of the confounding factors tested (gender, age, atopy, AR, and smoking status), only the presence of AR was found to negatively correlate with endoscopy scores after a 12-week course in the mometasone furoate group, indicating that mometasone furoate may be more effective in relieving nasal swelling and secretion in CRSsNP patients with concomitant AR. This may be partially because of the prominent therapeutic effect of glucocorticoids on AR.20–22 Although it remains controversial whether there is a causal relationship between allergic reaction and CRS, AR may exacerbate the development of CRS through promoting mucosal edema and increasing mucosal reactivity to allergic and nonallergic stimulus.23,24 Regarding macrolides treatment, some studies suggested that the symptom improvement inversely correlated with peripheral blood eosinophil count and serum IgE levels,5,18 indicating that those with atopy and eosinophilic inflammation are less likely to respond to macrolides treatment. However, in this study, we did not find the influence of atopy on the therapeutic effect of clarithromycin in the treatment of CRSsNPs. An ex vivo study indicated that clarithromycin could produce a significant, dose-dependent reduction in the production of eosinophilic cytokines IL-5 and granulocyte-macrophage colony-stimulating factor in sinonasal mucosa from CRSsNP patients. 13 Twelve-week treatment with clarithromycin could significantly reduce nasal lavage eosinophil cationic protein levels in CRS patients in an open-label study. 25 Therefore, additional studies are warranted to investigate the effect of macrolides on eosinophilic inflammation.
In this study, the doses of these two agents were chosen based on a previously published article showing that mometasone furoate nasal spray, 200 μg once daily, is effective and safe in treating CRSwNPs for reducing polyp size and improving nasal obstruction and rhinorrhea, 26 and clarithromycin, 250 mg once daily, provides marked improvement of quality of life and reduces IL-8 and eosinophil cationic protein levels in nasal lavage. 25 Moreover, these regimens are commonly used in China for the treatment of CRSsNPs. It is possible that a twice-a-day regimen of either of these treatments may be more efficacious; however, it needs further investigation.
It should be noted that this study is a preliminary trial with several limitations, such as a small sample size, no placebo control, no follow-up for recurrence after cessation of treatment, no measurement of inflammatory mediators, etc. Despite these limitations, the results of this study clearly show that both mometasone furoate nasal spray (200 μg once daily for 12 weeks) and clarithromycin tablet (250 mg once daily for 12 weeks) are effective in reducing symptoms and improving mucosal swelling and nasal discharge for CRSsNPs in Chinese adults and these two treatments have comparable clinical effects. It will be of great interest to investigate whether there is a synergistic effect between these two agents in the treatment of CRSsNPs in the future.
Footnotes
Acknowledgments
The authors thank Dr. Jian-Bo Shi and Dr. Hua-Bin Li (Otorhinolaryngology Hospital, the First Affiliated Hospital of Sun Yat-sen University) for their helpful suggestions.