
Abstract
Background
Pollybeak deformity due to abundant fibrosis formation in the supratip region after rhinoplasty is still a common problem. The aim of this study was to investigate the effects of a modified subcutaneous approximation suture on pollybeak deformity of soft tissue origin.
Methods
Three groups, each consisting of eight rabbits, were included in the study. Nasal skin was elevated with an open rhinoplasty approach in all groups. During closure of the skin, to minimize supratip dead space, a horizontal subcutaneous approximation suture was used in group I, external tape fixation was used in group II, and no further action was taken for supratip skin approximation in the control group. Full-thickness supratip skin biopsy specimens reaching down to the underlying cartilage tissue were taken from each subject on the 60th day after the operation. Thicknesses of subcutaneous scar tissues were measured histologically in all groups and compared.
Results
The mean thickness of the subcutaneous scar tissues was significantly lower (0.98 ± 0.32 mm) in group I than in group II (1.65 ± 0.61 mm; p = 0.036) and the control group (1.72 ± 0.49 mm; p = 0.019). However, there were no significant differences between group II and the control group in the mean thickness of subcutaneous scar tissues (p = 1.000).
Conclusion
The findings of this study indicate that the subcutaneous approximation suture is effective for preventing excessive scar tissue formation in the supratip area after rhinoplasty in rabbits. Further clinical studies are needed to determine its efficacy in humans.
Pollybeak deformity represents a postoperative fullness in the supratip area, which causes a disproportion between the tip and the supratip, impairing the expected nasal profile. It may be a result of the disarrangement of the cartilaginous framework or postoperatively abundant soft tissue formation in this region. Excessive cartilaginous tissue in the supratip area may be considered the main reason for postoperative pollybeak deformity formation. However, overresection of the caudal dorsum does not prevent recurrence of the problem. On the contrary, it has been reported that this practice accentuates postoperative supratip fullness by increasing subcutaneous dead space, which is replaced by scar tissue. 1 Inadequate tip projection, cephalically oriented lower lateral cartilages, overprojected caudal dorsum, overresected midvault, and poor redraping of the nasal skin may be other contributing factors in the development of postoperative pollybeak deformity. 2
Regardless of the primary etiology, postoperative supratip fullness is exacerbated by soft tissue formation at the dead space, lying between the nasal skin and the cartilaginous nasal dorsum. Pollybeak deformity caused by any structural abnormality in the cartilaginous framework can be eliminated with fine surgical techniques. However, there is no satisfactory method for the prevention of supratip fullness that results from excessive new soft tissue formation during the postoperative healing period. Currently, the most commonly used method for this purpose is vigorously taping the supratip region, but the tapes loosen, especially on oily skin, limiting its efficacy. The subcutaneous approximation suture method was used in a previous clinical study to eliminate supratip dead space, but its effect on scar tissue formation after rhinoplasty operations was not clear. 2 The current study aims to investigate the effects of a modified approximation suture, which creates direct contact between supratip nasal skin and the underlying cartilages on postoperative pollybeak deformity of soft tissue origin in an animal study.
Materials and Methods
This study was approved by the Animal Research Ethics Committee of Gulhane Military Medical School (09/75-K), which follows the ethical rules of the European Union for animal experimentation. All subject animals were provided by the Research and Development Center, Gulhane Military Medical Academy, Ankara, Turkey. The study was conducted between November 2009 and March 2010. Three groups of eight rabbits each were formed, based on the type of intervention used for preventing dead space at the supratip region after open rhinoplasty.
Surgical interventions were performed under general anesthesia (ketamine hydrochloride at 50 mg/kg and xylazine hydrochloride at 8 mg/kg, intramuscular). The nasal skin was elevated by open rhinoplasty procedure. A transcolumellar incision was made and connected to bilateral marginal incisions with a number 11 blade. The lower lateral cartilages, the upper lateral cartilages, and the os nasale were exposed through the subcutaneous areolar tissue plane by using sharp scissors. No excision of cartilaginous or bony framework was performed. Bleeding was controlled with cautery, and the skin incisions were closed with 4-0 Prolene sutures (Ethicon, Inc., Somerville, NJ). Three different techniques were used during skin closure. In group I, a suture that eliminates dead space by creating full contact between the nasal skin and the underlying cartilages was placed at the supratip region (Fig. 1). In group II, a 2-cm-wide nasal tape was used externally, without placing a subcutaneous approximation suture (Fig. 2). The ends of the tape were pulled down tightly to provide compression to the underlying skin and then sutured to the lateral sides of the nose. The tapes were removed on the 15th postoperative day. In group III (control group), the elevated nasal skin was closed without using subcutaneous approximation suture or taping.

Subcutaneous approximation suture, passing through the supratip skin and the intranasal part of the caudal septum. Arrows indicate the route of the suture.

External nasal taping in group II. Ends of the tape were fixed to the furry skin of the nose.
Two months after the initial surgery, a horizontal incisional, full-thickness skin biopsy of the supratip region (10 mm long and 5 mm wide) was taken from the animals in all three groups, under general anesthesia. The biopsy specimens included epidermis, dermis, and subdermal scar tissue extending down to the underlying cartilage. All biopsy specimens were taken from 20 mm above the nasal tip (Fig. 3). All of the biopsy specimens were fixed in 10% neutral buffered formalin.
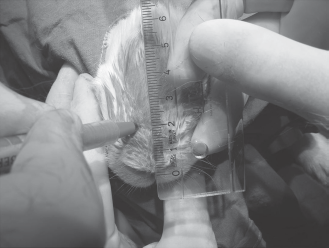
Full-thickness skin biopsy site at the supratip region.
Scar thickness measurements were performed at the Pathology Department by a pathologist using the double-blind method. After routine overnight tissue processing and paraffin embedding, 4-μm-thick sections were prepared and stained, using Masson's trichrome method to increase the contrast between connective and nonconnective tissues by emphasizing the collagenous component. Then, digital images showing the full thickness of the samples were obtained under 20X magnification. ImageJ (Rasband; W.S. U.S. National Institutes of Health, Bethesda, MD), an open-source, Java-based image processing and analysis software was used for measurements. Two measurements from the thickest parts of the samples were taken. The first measurement showed the distance from the epidermis to the lower border of the subcutaneous muscle layer, and the second measurement showed the distance from the lower border of the subcutaneous muscle layer to the deepest point of the biopsy material, which consisted of newly formed scar tissue (Fig. 4). All measurements were expressed in millimeters. Thicknesses of the skin and the subdermal scar tissue were compared among the groups.
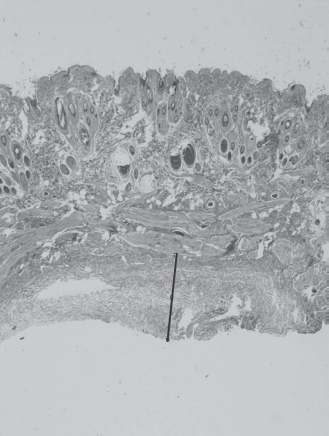
An example of the subcutaneous connective tissue thickness measurement. Measurements of the newly formed connective tissue and the overlying skin were marked with lines.
MS Excel (Microsoft, Inc., Redmond, WA) and SPSS for Windows Version 15.0 (SPSS, Inc., Chicago, IL) software packages were used for statistical analysis of data. A one-way ANOVA test was used fordetermining any significant differences between measurements among the three groups. If the results of the initial ANOVA test were significant, Bonferroni's post hoc test was used to determine the origin of the differences. The cutoff value for statistical significance was accepted as p < 0.05.
Technique of the Approximation Suture
We modified the subcutaneous suture that was used by Guyuron et al. for eliminating supratip dead space. 2 Guyuron et al. placed a stitch between the subcutaneous tissue and the immediate underlying cartilage at the supratip region. 2 We passed a 4-0 Vicryl suture (Ethicon, Inc.) from inside the left nasal passage to the outside of the cartilaginous roof, at the top of the nasal valve location (Fig. 1). Lateral placement of the suture was especially avoided for the prevention of nasal valve narrowing. The suture was passed horizontally through the subcutaneous tissue until the top of the other nasal passage was reached (Fig. 1) and then inserted into the right nasal passage from the symmetric location on the left side. Finally, the needle was passed through the intranasal part of the caudal septum to the initial side of the nasal passage. After closing the columellar incisions, the free ends of the suture were pulled outside of the nostrils as needed to create direct contact between the nasal skin and the underlying cartilages, and then the suture was tied (Fig. 5).

Final knot of the suture at the initial side of the nasal passage.
Results
Twenty-four male rabbits, 15–17 months old (mean, 16 months) and weighing 2000–2250 g (mean, 2150 g), were included in the study. Histopathological measurements from biopsy materials that were taken from the supratip region on the 60th postoperative day are shown in Table 1. Mean thicknesses of the skin in the biopsy region were 3.53 ± 0.75 mm in group I, 3.62 ± 0.43 mm in group II, and 3.37 ± 0.28 mm in group III; the thicknesses did not differ significantly among the three groups (p = 0.633).
Thicknesses of postoperative subcutaneous scar tissue and the supratip skin
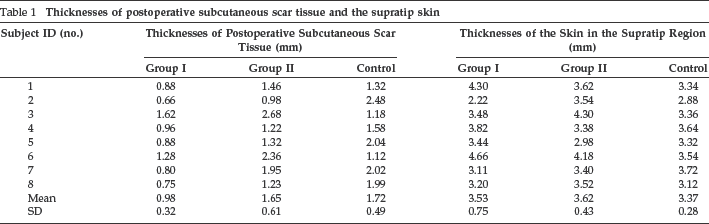
Mean thicknesses of the measured subcutaneous scar tissues on the 60th postoperative day were 0.98 ± 0.32 mm in group I, 1.65 ± 0.61 mm in group II, and 1.72 ± 0.49 mm in group III. The mean thickness of subcutaneous scar tissue was significantly lower in group I compared with group II (p = 0.036) and the control group (p = 0.019). There was no significant difference between group II and the control group (p = 1.000) in terms of mean thickness of subcutaneous scar tissue.
Discussion
Supratip fullness is one of the most common, esthetically unpleasant, postoperative nasal deformities requiring revision rhinoplasty.3–5 Pollybeak deformity originating from cartilaginous disarrangement is out of the scope of this study. Excessive scar formation during the postoperative healing period may result in independent fullness at the supratip region, or it may accentuate any previously existing fullness on the cartilaginous framework. In a study by Guyuron et al., 77.3% of patients who underwent secondary rhinoplasty had histologically proven excessive fibrosis at the supratip region. 2 In that study, other elements that were found in the supratip connective tissues other than fibrosis were newly formed hyaline cartilage, distorted skeletal muscle, and nerve segments. 2
Predicting which patients might develop pollybeak deformity in the postoperative period is not an easy task. Patients with a history of previous hypertrophic scarring or keloid formation, as well as those who have thick skin, may be the most likely candidates. 2 Taping the supratip region is a classic precaution for preventing immediate postoperative supratip fullness due to hematoma and edema. An external nasal splint, placed between the radix and the supratip, also may prevent edema. Squeezing the splint from the lateral direction should be avoided, because it may lift the nasal skin and create an additional unwanted tissue space at the supratip region. 6 The splint and tapes may be removed at the end of the 1st week or, if considerable edema persists in the supratip area, the nose can be retaped for an additional week. 6 Compressive taping of the supratip area at night is recommended until a supratip break is created permanently. 6
Several other methods are advocated for preventing postoperative pollybeak deformity. If no satisfactory response is achieved within 4 weeks by taping, 0.1–0.2 mL of triamcinolone acetonide at 40 mg/mL can be injected into the supratip area. 2 Hanasono et al. reported a good, subjective supratip definition in 85% of patients who underwent rhinoplasty and had two triamcinolone injections at the 1st and 4th postoperative weeks. 7 They reported no complications due to steroid injection in a series of 127 patients. 7 However, there is a risk of side effects, such as dermal telangiectasias, depressions, color changes, and contour irregularities, which may result from reduced skin thickness. 2 Conrad et al. used homologous fibrin glue to adhere the nasal skin to the underlying skeletal framework, and they reported successful esthetic outcomes in patients who underwent rhinoplasty operations. 8
If enough reduction of supratip fullness is not achieved after three steroid injections by the 4th week, surgery may be considered to remove excess scar tissue. Nevertheless, before any action is taken, at least 1 year should pass after the initial procedure. 2 Revision surgery basically aims to adjust the cartilaginous framework, remove excess scar tissue, and eliminate potential subcutaneous space. After resection of the supratip scar, deficient caudal septum may be supported with several kinds of cartilage grafts during revision surgery.2,9,10 However, elimination of the dead space at the initial operation or during revision surgery should be the main concern for preventing excessive postoperative scar tissue reformation at the supratip area. Overresection of the caudal dorsum, which inevitably increases the supratip dead space, should strictly be avoided. The most important caution for minimizing the supratip dead space is establishing direct contact between the nasal skin and the underlying cartilages. Guyuron et al. recommended a suture that was passed through subcutaneous tissue and the underlying cartilages to diminish this space, especially in patients with thick skin. 2 This suture creates an ideal supratip break and also may decrease the need for additional grafting for tip projection. 11 However, the effect of this suture on postoperative subcutaneous scar formation has not been clearly established in previous clinical studies.
In this study, we aimed to investigate the effect of a modified approximation suture on postoperative subcutaneous scar tissue formation at the supratip region in an objective animal study. This suture begins from one nasal passage, passes outside of the nasal cartilaginous roof, horizontally passes through the supratip subcutaneous tissue, and enters the other nasal passage. Contrary to the approximation suture used by Guyuron et al., the suture knot is placed in the nasal passage after closing the surgical incisions. 2 Therefore, the length of the skin between the subcutaneous suture line and the columellar incision fits well into the underlying framework. Direct contact between the supratip skin and the underlying cartilaginous framework is established by pulling the suture out of the nostrils. Furthermore, it provides an opportunity to adjust the tightness of the suture as needed. This suture is believed to eliminate supratip dead space more efficiently than external taping.
Conclusion
In conclusion, findings of this study showed that subcutaneous approximation suture is an effective measure for preventing excessive scar tissue formation in the supratip area after rhinoplasty in rabbits. Additional clinical studies are needed to determine the efficiency of this suturing technique in humans.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article