
Abstract
Background
Allergic rhinitis (AR) is a symptomatic disorder of the nose induced after allergen exposure by an IgE-mediated inflammation of the nasal mucosa. This study was designed to investigate the role of nasal mucosa temperature in AR.
Methods
We investigated the relationship between eosinophilic infiltration, nasal obstruction, and nasal mucosa temperature in 35 children with rhinitis aged 6–12 years.
Results
A significant relationship was shown between nasal temperature values and eosinophil infiltration at nasal cytology (p < 0 01). Nasal temperature was also significantly associated with nasal obstruction, assessed in terms of nasal volume (Vol [2–5 cm]; p < 0.05) and minimum cross-sectional area (p < 0.01). No significant correlation emerged between the degree of nasal obstruction and presence of eosinophils at nasal cytology (p > 0.05).
Conclusion
These results suggest a relationship between nasal temperature and nasal mucosa inflammation and obstruction. (ClinicalTrials.gov number: NCT00952835)
Nasal congestion can be objectively assessed by acoustic rhinometry, which is a validated method to measure nasal patency also in young children3,4 needing a specifically dedicated device and trained operators.
The severity of AR has been shown to be related to the degree of nasal mucosa eosinophil infiltration,5,6 which can assessed by the evaluation of cytological samples obtained by nasal scraping. 7
Although the collection of nasal cells by scraping the nasal mucosa is only minimally invasive for the patient, it requires some laboratory facilities to get stained slides and a degree of skill for the operator to have a reliable result.
Airway temperature has been suggested to represent a marker of mucosal inflammation and remodeling in asthmatic children,8,9 being related with mucosal eosinophilia and vascular remodeling. 10
The aim of this study was to evaluate whether the temperature of nasal mucosa, which is easily assessable by a direct measurement, is related to nasal eosinophil infiltration 11 and obstruction.
Patients and Methods
Subjects and Experimental Design
This study enrolled 35 patients (22 male and 13 female patients) ranging in age from 6 to 12 years attending the Center of Pediatric Allergy, G.B. Rossi Hospital (Verona, Italy). All of the children had positive SPT results for at least one of the most common aeroallergens relevant in the area of Northern Italy as well as a medical history positive for symptoms and signs of AR. Twenty-two children (63%) were affected also by asthma. The presence of a family history positive for atopy and of atopic symptoms (asthma, AR and conjunctivitis, and atopic eczema) was evaluated for each patient. None of the children was receiving drug treatment such as intranasal corticosteroids or antihistamines 1 month before and at the time of the study. The presence of fever or cold was excluded.
The study was performed over a 6-month period, starting from February to July 2010. All of the patients underwent nasal scraping for cytology evaluation and nasal airway temperature and patency assessment. To avoid bias due to possible interferences between the different methods, measurements were performed following this order: (1) nasal temperature evaluation, (2) acoustic rhinometry, and (3) nasal cytology.
This study was approved by the University of Verona Research Ethics Committee and has been registered on Clinicaltrials.gov (NCT00952835).
Skin-Prick Test
Children underwent SPT with commercial extracts (Stallergenes, Milan, Italy) for the following allergens: grasses, plantain, Alternaria, Parietaria, birch, hazelnut, Artemisia, Cladosporium, Aspergillus, Dermatophagoides pteronyssinus, Dermatophagoides farinae, and cat and dog dander. The positive control was histamine at 1 mg/mL. The negative control was diluent of extracts. The results were evaluated after 15 minutes. Wheals at least 3 mm greater in diameter than the wheal at the site of the negative control were considered positive.
Nasal Temperature Evaluation
The temperature of the nasal mucosa was evaluated by means of an infrared electronic thermometer (GENIUS 2; Kendall, Mansfield, MA). The measurements were performed at least after 30 minutes of rest in a sitting position and patients were asked to keep breathing during the acquirement of the data (5–6 seconds). The environmental temperature was controlled to maintain a stable condition of 23 ± 1°C and a relative humidity of 40–50%.
Axillary body temperature was always measured by an electronic thermometer and had to be 36.5 ± 0.3°C to allow the subject to be enrollment in the study data collection.
Temperature measurements were performed by placing the thermocouple in contact with the mucosal surface of the nasal valve and anterior turbinate area. The measurements were repeated three times in each nostril and the mean value was used for analysis.
Upper Airway Patency
Nasal patency was assessed by acoustic rhinometry according to standardized international guidelines. 12 Measurements were made by a trained research assistant using the Hood Laboratories continuous wideband acoustic rhinometer (Sensormedics, Milan, Italy) with a small-sized anatomic nose adapter. To improve the connection between the anatomic nose adapter and the nostril and to significantly improve speed, precision, and reproducibility of measurements, a rim of gel has been applied on the nose adapter. 13 The child was seated facing the examiner and stopped breathing for ∼5 seconds with the probe tube applied to the nostril. Two independent measurements were obtained from each nostril and the mean value was used for statistical analysis. The volume of the nasal cavity corresponding to the lower turbinate (Vol [2–5 cm]) and the minimum cross-sectional area (MCA) were selected as important variables for mucosal changes.14,15
Nasal Cytology
Cells were collected by gently scraping the middle third of the inferior turbinate with a nasal plug. After fixation and staining with May-Grunwald-Giemsa, the samples were evaluated for the presence of eosinophils and a score was assigned to each field as follows: 0 = none; 1 = few, scattered cells; 2 = moderate number of cells, small clumps; 3 = large clumps, not covering the whole field; and 4 = clumps covering the whole field. 16 At least 10 fields were observed from each slide under a magnification of X100 with immersion oil. The final result was expressed as the mean score for each slide.
Statistical Analysis
Associations between nasal mucosa temperature, nasal patency, and presence of eosinophils at nasal cytology were studied using linear models while comparison between asthmatic and nonasthmatic subgroups of patients was performed by unpaired t-test. The level of probability was considered significant if p < 0.05. All analyses were performed using StatGraphics software Version 9.1 for Windows (SAS Institute, Cary, NC).
Results
Environment temperature was kept between 22 and 23°C and relative humidity was between 40 and 50% throughout the study period.
Body temperature ranged between 36.5 and 36.8°C. Twenty-eight children (80%) had a family history positive for asthma, AR and conjunctivitis, and/or atopic eczema.
Considering the whole group of 35 patients, there was a significant relationship between nasal temperature values and the score of eosinophil infiltrate at nasal cytology (r = 0.64; p < 0.01; Fig. 1). Nasal temperature was also significantly and inversely associated with nasal airway volume (Vol [2–5 cm]; r = -0.35; p < 0.05; Fig. 2) and nasal MCA (r = -0.44; p < 0.01; Fig. 3). When considering the presence of eosinophils at nasal cytology, no association emerged between nasal patency and the score of eosinophil infiltrate (p > 0.05). The mean values for nasal temperature, presence of eosinophils at nasal cytology, and nasal patency in the two subgroups of asthmatic and nonasthmatic children are reported in Table 1. Nasal temperature values and eosinophil scores were significantly higher in the group of asthmatic patients than in the group of patients with only AR (p = 0.01 and p < 0.001, respectively). In contrast, no significant difference was observed for nasal airway obstruction (p > 0.05). The maximum value for Vol (2–5 cm) was 2.35 cm3 in the asthmatic children subgroup and 3 cm3 in the nonasthmatic group.
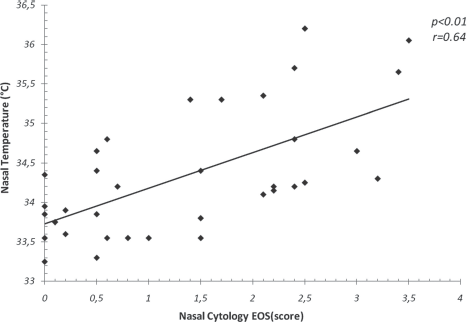
Association between nasal mucosa temperature and eosinophils (EOS).
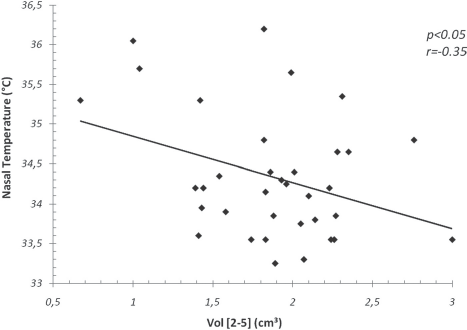
Inverse association between nasal mucosa temperature and nasal airway volume (Vol [2–5]).
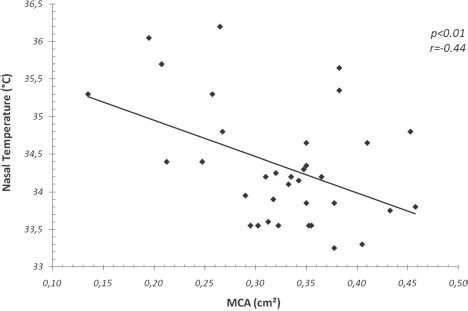
Inverse association between nasal mucosa temperature and nasal minimum cross-sectional area (MCA).
Nasal mucosa temperature, eosinophils score, MCA, and nasal cavity volume (Vol [2–5]) mean, minimum, and maximum values in the two subgroups of asthmatic and nonasthmatic children with rhinitis
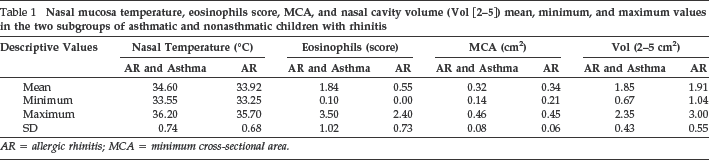
AR = allergic rhinitis; MCA = minimum cross-sectional area.
Discussion
The results of this study show that nasal mucosa temperature is related to the presence of eosinophils in nasal mucosa cell samples, which is an objective marker of mucosal inflammation in children with AR.17–20 This finding is in agreement with previous studies in allergic asthmatic patients who showed significant positive correlations between the temperature of exhaled air and exhaled nitric oxide as a marker of lower airway inflammation.8,9
Nasal temperature is related not only to nasal eosinophilia but also to nasal obstruction assessed by measurement of patency (Vol [2–5 cm]; MCA). Nasal congestion and obstruction are important features of allergic inflammatory response.21–23 However, only few studies, performed by the technique of facial thermometry and not by a direct assessment of nasal mucosa temperature, have analyzed the relationship existing between nasal congestion and nasal temperature showing mucosal blood flow to be strictly involved in the determination of both of them.24,25 At the site of the nasal mucosa a large supply of subepithelial capillaries, arterial systems, and venous cavernous sinusoids 26 may play a key role in the pathogenesis of nasal obstruction. In our study population no statistically significant relationship has been found between the degree of eosinophil infiltration of the nasal mucosa and the degree of nasal obstruction, thus further supporting the hypothesis that the pathology of the nasal is somehow paralleling the events occurring in the deeper airways in asthma. In fact, the nasal congestion in AR could represent a tissue remodeling process of the nasal mucosa like that observed in the bronchi of asthmatic patients. 27 This hypothesis is in agreement with previous studies in AR children, which showed an irreversible nasal airway obstruction probably because of the remodeling of the mucosa. 4 It is therefore tempting to speculate that chronic inflammation and remodeling of the upper airways might be a part of a generalized remodeling of the airways, including lower airways in accordance with the “one airway, one disease” model.28,29
Loss of the protective functions of the nose is the simplest mechanistic explanation, while absorption of inflammatory mediators such as IL-5 from sites of inflammation into the systemic circulation has been shown to result in release of eosinophils from the bone marrow, prolonged blood eosinophilia, and thereby possibly systemic propagation of the disease from the nose to the lung. 30 However, because the relationship between nasal obstruction and mucosal vascular changes and remodeling is still not fully understood, further studies need to be performed in AR patients assessing upper airway patency by acoustic rhinometry before and after decongestion with intranasal α-agonist. 31 Considering nasal temperature measurements, it is important to underline that a precise definition of the site and time of detection in the respiratory cycle is of primary importance to avoid the influences of these factors on the mucosal surface temperature within the nasal airways.32–34 In fact, mucosal temperature decreases during inspiration by evaporation and colder inspired air, whereas it increases during expiration because of the effect of the warm air that comes from the lungs. Moreover, in the nasal valve area and anterior turbinate area, the end inspiratory and end expiratory temperatures are significantly lower than in the nasal vestibule and the nasopharynx because of the closer contact between the colder inspired air and the nasal mucosa.
In conclusion, an objective approach to childhood AR is essential to improve the management of this pathology as well as the health-related quality of life of these patients and to reduce the incidence of comorbid disorders such as asthma.35–37 The results of this preliminary study show that nasal mucosa temperature is related to both nasal eosinophilia and nasal congestion and obstruction, suggesting a possible use of this parameter in the clinical practice. The data obtained in this study give also the basis for a new field of investigation in AR, which warrants better defining the role of nasal mucosa temperature as a disease marker in AR.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article