
Abstract
Background
There is a correlation between 18F-fluorodeoxyglucose (FDG) uptake and the level of intracellular metabolic tumor activity, which in turn may be associated with active proliferation, invasion, and prognosis as well as distant metastases in head and neck cancer. This study was designed to assess whether tumor uptake of FDG positron emission tomography (PET) expressed as the maximum standardized uptake value (SUVmax) can be used to predict survival in subjects with paranasal sinus malignancy.
Methods
We enrolled 42 consecutive subjects with a histological diagnosis of squamous cell carcinoma in paranasal sinus malignancy, into a retrospective institutional imaging trial. Thirty-eight subjects (90.5%) underwent a baseline FDG-PET scan before curative treatment and were eligible for analysis.
Results
A total of 38 subjects with paranasal sinus malignancy undergoing PET/computed tomography imaging in the initial stages were assessed separately for a potential correlation between SUVmax and T staging, histological grading, and overall survival. Log-rank testing revealed a significant correlation between overall survival and histological grading (p = 0.046); and there was some correlation between SUVmax and histological grading, but not significantly different. The receiver operation characteristic curve was identified for cutoff value of SUVmax as a prognostic factor. We compared the low tumor of the SUVmax group with the high tumor of the SUVmax group divided by the cutoff value of SUVmax. We did find a significant correlation between SUVmax and disease control and mortality (p = 0.003, p < 0.001).
Conclusion
In our study, we concluded that subjects with higher tumor FDG uptakes should be considered for a more aggressive disease.
Materials and Methods
Subjects
We retrospectively reviewed the charts of all subjects who had presented for initial treatment of paranasal sinus malignancy with a histologically confirmed diagnosis of squamous cell carcinoma between January 2005 and October 2011.
A total of 38 subjects with a confirmed histology and previously untreated paranasal sinus malignancy underwent FDG-PET/CT for initial staging.
Each case was staged according to the 2010 American Joint Committee on Cancer TNM staging system. 7 A subject presenting with distant metastatic disease (M1) was excluded. The distribution of TNM stages in the 38 patients was as follows: stage I in 1 patient, stage II in 1 patient, stage III in 16 patients, and stage IV in 20 patients.
This retrospective analysis was conducted according to the ethical guidelines of the Severance Hospital, Yonsei University College of Medicine Institutional Review Board.
Histological Grading
The histological workup of the primary tumor was performed according to the guidelines of the Swiss Society of Pathology. The specimens were subdivided into well differentiated, moderately differentiated, and poorly differentiated groups.
Imaging Protocol
A combined PET/CT inline system (Discovery LS or Discovery ST; GE Healthcare, Milwaukee, WI) was used for this study. This device integrates a PET scanner (DSTe; GE Healthcare) with a multislice helical CT (16 slice; GE Healthcare) and permits the acquisition of coregistered CT and PET images in the same session. Subjects fasted for at least 4 hours before scanning, which started 60 minutes after the injection of a standard dose of ~350 MBq of FDG. All subjects were examined in the supine position with arms up. The CT scan was acquired during free shallow breathing. In the normal expiratory position, the following parameters were used: 140 kV, 80 mA, 0.5-second tube rotation, 4.25-mm section thickness, and a scan length of 867 mm with a 22.5-second scan time. Acquisition of the FDG PET scan was started immediately after the CT with an emission time of 3 minutes per table position, resulting in a total scan time of 18 minutes for six table positions from the head to the pelvic floor. CT data were used for attenuation correction. PET images were reconstructed using a standard two-dimensional iterative algorithm (ordered subset expectation maximization).
SUVmax Analysis
A board-certified physician in nuclear medicine and radiology in reading combined FDG-PET/CT in head and neck cancer subjects determined the SUVmax retrospectively. SUVmax was calculated using a commercially available workstation (Advantage Workstation, software Version 4.4; GE Healthcare). Before determining SUVmax, the rhinologic physician measured the correct localization of the primary tumor retrospectively. In this procedure, the rhinologist was blinded and did not know the outcome of treatment and patient status; only the coded unit number was provided. A region of interest (ROI) was defined on screen that included the FDG uptake related to the primary tumor on multiple consecutive image sections by the radiologist. The value of the single voxel with the highest activity within this ROI was used for calculation of SUVmax. The software provides this value automatically. All values were normalized to the lean body mass of the subject. The use of lean body mass instead of body weight has been shown to be less dependent on the body habitus of the study population.
Statistical Analysis
This study analyzed the following end points: the correlation between SUVmax and survival time and the potential correlation between SUVmax and histological grading, treatment strategy, and disease control. The Kaplan-Meier method and log-rank test were applied to calculate overall survival rates between histological grading groups. The Mann-Whitney U test was used to assess the potential correlation of SUVmax in the survival group and nonsurvival group. We applied Fisher's exact test for prognostic effect with mortality and SUVmax. The values of p < 0.05 were considered significant.
Cox proportional hazards analysis was performed for primary tumor SUVmax and each of the other individual tested risk factors. We also determined the cutoff value of SUVmax between the survival group and nonsurvival group using a receiver operation characteristic curve. All calculations were performed using SPSS Version 18.0 for Windows (SPSS, Inc., Chicago, IL).
Results
Demographics
Between 2004 and 2011, a total of 42 subjects were evaluated using FDG-PET/CT for previously untreated paranasal sinus malignancy. Two subjects were excluded because of missing PET data, and two subjects were excluded because the primary PET was not evaluated in our hospital. Finally, 38 subjects remained for evaluation. The mean follow-up length was 40.44 ± 21.63 months (range, 1–101 months). There was a male predominance (n = 30; 78.9%), and the mean age was 54.42 ± 11.36 years (range, 29–83 years; Table 1).
Subject characteristics
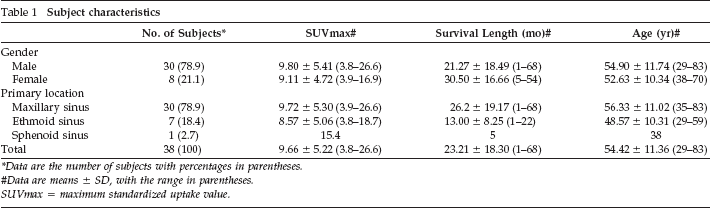
Data are the number of subjects with percentages in parentheses.
Data are means ± SD, with the range in parentheses.
SUVmax = maximum standardized uptake value.
Correlation between Histological Grading and Overall Survival with SUVmax
Of the 38 primary tumors, 4 (10.5%) were well differentiated, 20 (52.6%) were moderately differentiated, and 14 (36.8%) of paranasal sinus malignancy were found to be poorly differentiated (Table 2). The well-differentiated and moderately differentiated groups had significantly better 5-year overall survival than the poorly differentiated group in log-rank testing (Fig. 1). The 5-year overall survival for subjects by histological grade was 75.0, 75.0, and 28.6%, respectively (p = 0.046).
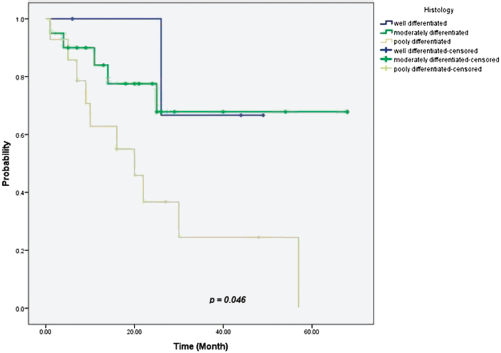
Five-year overall survival of histological grading groups. The graph shows Kaplan-Meier disease-free survival probabilities for histological grading. There were 3, 15, and 4 subjects that were disease-free for each histological grading category, respectively, at the end of the follow-up period.
Histological grading characteristics
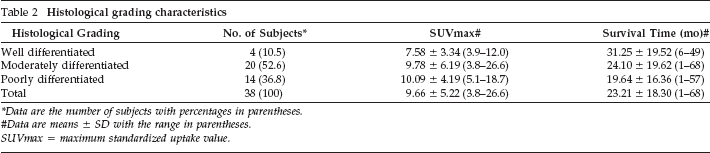
Data are the number of subjects with percentages in parentheses.
Data are means ± SD with the range in parentheses.
SUVmax = maximum standardized uptake value.
The median survival times for subjects in the well-differentiated, moderately differentiated, and poorly differentiated groups were 31.25 ± 19.52 months (range, 6–49 months), 24.10 ± 19.62 months (range, 1–68 months), and 19.64 ± 16.36 months (range, 1–57 months), respectively. However, the difference in mean SUVmax for each group was not statistically significant (p = 0.446).
Cutoff Value of SUVmax as a Prognostic Factor
The most discriminate cutoff SUVmax value for positive prognosis proved to be 9.05, which corresponds to 83.3% sensitivity and 95.0% specificity on the receiver operation characteristic curve (Fig 2). It was evaluated by Youden index (index = 0.783).
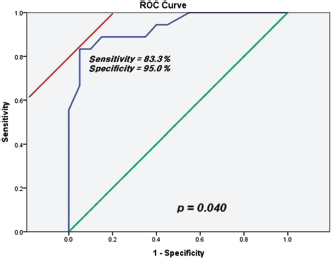
The receiver operation characteristic (ROC) curve for the SUVmax cutoff value. A positive actual status is death and the area of the 95% confidence interval covers between 0.732 and 0.973. An SUVmax of 9.05 has 83.3% sensitivity and 95.0% specificity in this study.
Disease Outcome According to SUVmax
We divided the subjects into two groups: subjects with an SUVmax of <9.05 (low tumor SUVmax) and subjects with an SUVmax of ≥9.05 (high tumor SUVmax; Table 3). In the group of subjects with a low tumor SUVmax, T4 stage value had a greater association with poorer outcomes than T1-3 stage value (p = 0.035); however, in the group of subjects with a high tumor SUVmax, the trend was not found (p = 0.686). It meant that high SUVmax affected more poorer outcomes with or without high T staging. The group of subjects with a high tumor SUVmax (12/17 deaths) were associated with poorer outcomes than those with a low tumor SUVmax (4/21 deaths; p = 0.003).
Probability of mortality according to T Stage in the low SUVmax and high SUVmax groups
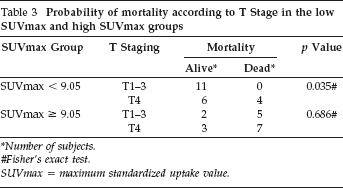
Number of subjects.
Fisher's exact test.
SUVmax = maximum standardized uptake value.
Univariate and Bivariate Analysis for SUVmax
Nonparametric testing using the Mann-Whitney U test showed an insignificant correlation between SUVmax and T staging (p = 0.306; Table 4). We found a statistically significant correlation between SUVmax and disease control and mortality; however, there was no significant correlation between SUVmax and treatment strategy (p = 0.311).
Clinical characteristics and correlations between SUVmax and T staging and disease control, mortality, and treatment
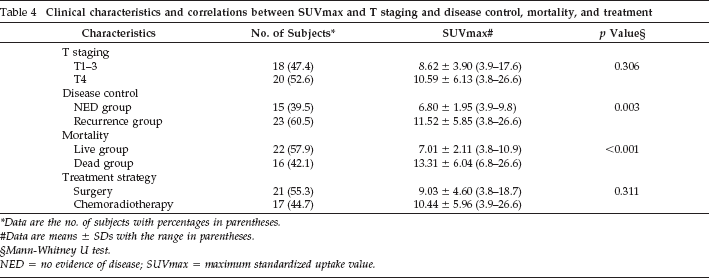
Data are the no. of subjects with percentages in parentheses.
Data are means ± SDs with the range in parentheses.
Mann-Whitney U test.
NED = no evidence of disease; SUVmax = maximum standardized uptake value.
In Cox proportional hazards analysis, SUVmax, T staging, and histological grading were found to be significant independent predictors of disease-free survival at 5 years, whereas subject age and treatment strategy were not identified as significant prognostic factors for disease-free survival (Table 5).
Cox proportional hazards analyses for local control and disease-free survival at 5 yr
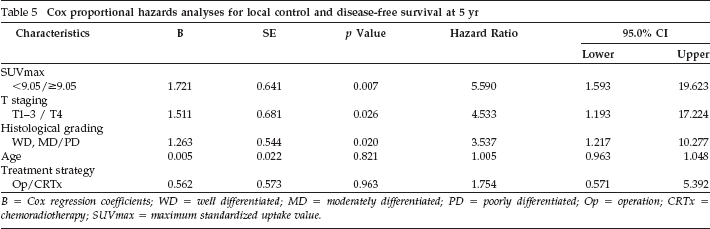
B = Cox regression coefficients; WD = well differentiated; MD = moderately differentiated; PD = poorly differentiated; Op = operation; CRTx = chemoradiotherapy; SUVmax = maximum standardized uptake value.
Discussion
FDG-PET/CT is an essential tool for initial staging in advanced HNSCC. Many important questions, such as the feasibility of SUVmax as a prognostic factor in paranasal sinus malignancy, can be answered at the time of diagnosis using FDG-PET. 2 Studies published in the last few years have shown a growing tendency to take into account tumor metabolic information when planning treatment for HNSCC and predicting a subject's outcome. 8
The aim of this study was to assess the correlations between different clinical and pathological parameters and SUVmax in paranasal sinus malignancy. In other previous studies these parameters may play an important role in confirming or refuting the latest theories that suggest FDG uptake of the primary tumor is related to treatment response and survival in HNSCC.9–12 Furthermore, SUVmax is the most widely used parameter for measuring metabolic tumor activity in oncologic FDG-PET/CT imaging. According to Machtay et al., a low SUVmax of the primary tumor was significantly associated with longer disease-free survival after radiotherapy of HNSCC in a series of 60 subjects. 6 On the contrary, Suzuki et al. found no correlation between SUVmax and treatment outcome in HNSCC after radiotherapy in a series of 45 subjects. 13
Therefore, to elucidate the role of SUVmax and its possible predictive value for therapy response, the aim of this retrospective analysis was to assess potential correlations between SUVmax and different clinical and pathological parameters at initial staging in paranasal sinus malignancy subjects. The results of our study also show that the group of subjects with a high tumor SUVmax (≥9.05) had a poorer outcome than those with a low tumor SUVmax (<9.05). In the group of subjects with a low tumor SUV, a high T stage was moderately associated with a poorer outcome compared with a low T stage (p = 0.035), but in the group of subjects with a high tumor SUV, there is no significant difference between a high T stage and a low stage (p = 0.686) suggesting that the combination of a high tumor SUVmax and a high T stage may be predictive of lower overall survival after initial treatment.
The potential value of FDG PET in predicting outcomes in head and neck cancer has been described in previous clinical studies. Minn et al. reported that a primary tumor SUV > 9.0 predicted an advanced clinical stage, low histological grade of differentiation, and poor overall disease survival in 37 subjects with head and neck cancer. 14 In another study, a tumor SUV > 10.0 predicted significantly inferior overall survival after surgery or definitive radiation therapy in 58 subjects. 10
Our findings confirm those of previous studies by showing significantly inferior local control and overall survival in subjects with a primary tumor SUVmax of ≥9.05, although treatment was heterogeneous in our study. However, treatment heterogeneity can not explain this result because both SUVmax subgroups were well balanced in this regard: 9 subjects versus 12 subjects in the surgery group and 8 subjects versus 9 subjects in the chemoradiotherapy group, for the high and low SUVmax subgroups, respectively.
To predict the clinical response to treatment, the dynamic FDG PET has been applied to several tumors, including head and neck cancer. 14 It has been concluded that the rate of tumor glucose metabolism could be a meaningful predictor of treatment response, although dynamic PET and kinetic analysis are complicated and time-consuming for both the subjects and the physicians in routine clinical work. The measurement of SUVmax is a simple and widely used method with good reproducibility and is highly correlated with kinetic parameters. 15 However, when SUVmax is applied, there is no definite, reliable cutoff for prognoses of paranasal sinus malignancy.
The important characteristic of this study is limited to squamous cell carcinoma of paranasal sinus malignancy, although other many previous studies have included subsites of head and neck cancer.16–20 Therefore, despite being present in the head and neck compartment, there can be many different clinical features depending on the subsites such as pathophysiological trend of lymph node metastasis. Putting all of the subsites together may neglect the important features of each subsite.
Especially, paranasal sinus malignancy near the brain was more intricate to define the ROI than the other head and neck subsites. Therefore, the SUVmax gave the significant meaning to the paranasal sinus malignancy, although more studies are needed to determine whether the separation of subsites in head and neck cancer will affect the feature of SUVmax.
In the same thing, although the relatively small population of this study gave the burden of statistical analyses, we performed evaluation in a single institution rather than multiple institutions to purify the conditions of this study such as settings and protocols of FDG PET-CT inline system; therefore, we suggest the 38 subjects were not small size considering low incidence. 21
Some limitations of this study need to be mentioned. Despite low incidence of paranasal sinus cancer in all malignancies, the small sample size limited an accurate assessment of the sensitivity and specificity of SUVmax. Additional studies are needed to confirm the possible value of SUVmax as a predictive factor of prognostic outcome. A bias could exist in the study design when determining the outcome of treatment when the rhinologist measured the location of primary site. Future prospective studies are needed using PET as the pretreatment to help make decisions about treatment and prognosis.
Conclusion
Our study showed that high FDG uptake in paranasal sinus malignancy is significantly associated with poor outcomes. We also found the clinical usefulness of continuous tumor SUVmax to be a significant and independent prognostic factor. In addition, high SUVmax of >9.05 may be predictive of poorer outcomes after initial treatment. Therefore, this study provided evidence that SUVmax could be suggested as a prognostic factor in paranasal sinus malignancy.