
Abstract
Malignant tumors of the sinonasal tract are uncommon tumors of the head and neck. Patients often present in the later years of life with unilateral symptoms and potential involvement of nearby structures such as the orbit, brain, or cranial nerves. Presenting symptoms are similar to patients suffering from inflammatory sinonasal disease and thus early diagnosis relies heavily on a high clinical suspicion. There are established risk factors based on exposure to the by-products of woodworking, metal, textile, and leather industries. Sinonasal malignancies are generally divided into those of epithelial origin (squamous cell carcinoma, adenocarcinoma, and adenoid cystic carcinoma) and nonepithelial origin (olfactory neuroblastoma, chondrosarcoma, and mucosal melanoma). Accurate histopathology confirmation and staging of the tumor is critical prior to making treatment decisions. Both computed tomography and magnetic resonance imaging are required to accurately determine the extent of local disease. Treatment is based on multimodality therapy, primarily surgical excision, and postoperative radiotherapy. This article reviews the classification of malignant tumors of the paranasal sinuses, their clinical presentation, relevant diagnostic investigations, and the principals of therapy and management.
As with other malignancies, the presentation may be related to local, regional, or distant disease. Defining the histology of the tumor and its stage are the key goals of investigations. Finally, treatment is generally multimodal with a combination of surgery and radiotherapy as the mainstay for most lesions. The proximity of critical structures, specifically the orbit, brain, and cranial nerves, dictate the morbidity from curative interventions.
Pathophysiology
The World Health Organization classification 10 is listed in Table 1 with the most common subtypes included. The epithelial versus nonepithelial distinction is easy and reflects the frequency of tumors. Epithelial tumors are the most common with squamous cell carcinoma (SCC), adenocarcinoma, and adenoid cystic carcinoma most commonly reported. 10 The nonepithelial tumors are lymphoma (hematologic), olfactory neuroblastoma (neuroectodermal), chondrosarcoma (bone/cartilage), and mucosal melanoma (neuroectodermal).
The World Health Organization classification system for sinonasal malignancies
The main subtypes are described here with common pathologies.
SCC = squamous cell carcinoma.
Undifferentiated nasopharyngeal carcinoma is often included in discussions on upper airway malignancy. However, it is not considered a sinonasal tumor and its origins are from epithelial and b-cell interactions of the nasopharynx. It is a common malignancy of young Southeast Asian men compared with the uncommon nature of most tumors discussed in this article. Its etiology is unique in that it is thought to arise from early Epstein-Barr virus infection in a genetically susceptible host.
There are several associated risk factors for the development of sinonasal malignancy. The most notable is wood dust exposure and adenocarcinoma. The large-particle dust from certain hardwoods (ebony, oak, and beech) are thought to provide a 900-fold risk of developing adenocarcinoma.9,11 Less than 5 years exposure is still considered critical and the latency to tumor development is delayed (~40 years).9,12 Smoking has been linked to SCC. 7 Metal industry products (chromate and nickel), leather and boot products and the textile industry (chrome pigments) and thorium dioxide, and imaging agents, are all risk factors for SCC. 13 Evidence for the role of human papilloma virus as a primary carcinogen in the sinonasal tract is strong but inconclusive and additional studies are required. 13
Diagnosis
The most important element in accurate diagnosis of sinonasal malignancy is clinical suspicion. The insidious onset of unilateral symptoms, the lack of previous inflammatory sinus disease or rhinitis, and the relative age of the patient (>50 years old for tumors compared with <50 years old for inflammatory disease) should be key features that prompt exclusion of neoplasia as a cause for a patient's symptoms.
Presentation
Although the presentation can be with regional symptoms (neck lumps, orbital changes, diplopia, epiphora, or cranial nerve dysfunction) and/or distant metastasis, this is relatively uncommon for most tumors and local (nasal obstruction, bleeding, discharge, and hyposmia) are the more common presenting symptoms. These symptoms share common presenting complaints of patients with inflammatory sinonasal disease, which again highlights the importance of initial clinical suspicion. Unilateral eustachian tube dysfunction can also occur. Gross macroscopic changes to hard palate mucosa or the skin are uncommon in developed countries. Endoscopic examination reveals a mass within the nasal cavity (Figs. 1 and 2).
Imaging
Imaging should always focus on what is trying to be achieved, viz., tumor staging. Accurate information on local tissue involvement is critical for “T” staging. Most patients will undergo both computed tomography (CT) and magnetic resonance imaging (MRI; Figs. 1 and 2). There are several key principals in rationale for both modalities. First, distinguish tumor from retained mucus. The T2 MRI will highlight edematous mucus and retained secretions compared with the tumor, seen on T1 postcontrast imaging (Fig. 2). Second, the involvement of the periobita is determined by bone loss on CT and fat enhancement on MRI. Third, dural (and brain parenchyma) involvement is defined by bone loss on CT and dural enhancement on MRI (Figs. 1, 2). Perineural involvement of cranial nerves is usually defined using fine slice fat-saturated T1 postcontrast MRI. Finally, the relationship of the tumor to the intracranial course of the internal carotid artery and its branches are defined by either CT angiography or MR angiography.
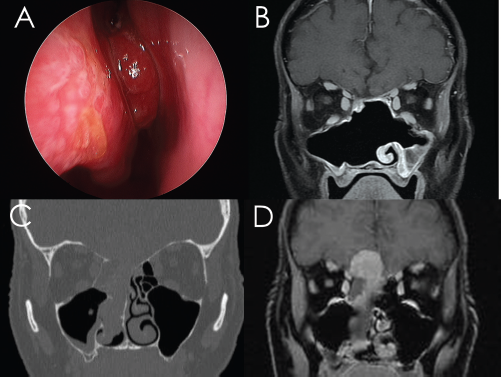
Olfactory neuroblastoma is a neuroectodermal tumor. It is radiosensitive and has a better outcome than epithelial tumors. (A) The characteristic strawberry red appearance of a mass arising from medial to the middle turbinate. (B) The postoperative magnetic resonance imaging (MRI) view. (C) The typical bone loss of the skull base must always be further assessed with an MRI (D) because it is a marker of potential intracranial involvement.
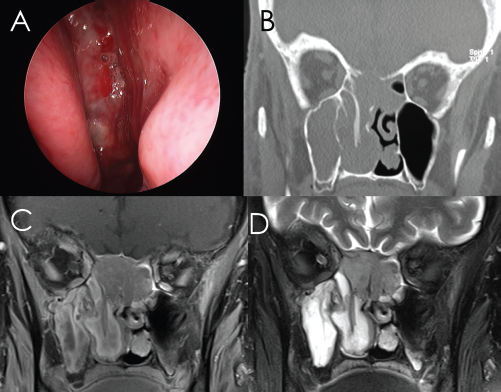
Squamous cell carcinoma (SCC) arising in a 62-year-old smoker. (A) The endoscopic view of a friable hemorrhagic mass filling the right nasal cavity. (B) Computed tomography (CT) showing loss of skull base bone and diffuse opacification of the surrounding sinuses. The T1 postgadolinium magnetic resonance imaging (MRI) (C) showing the sphenoid centered mass and T2 series (D) showing that much of the surround sinus changes is obstructive disease secondary to the tumor.
Regional and distant disease is commonly defined with a positron emission tomography/CT assessment. This technique is a combination of full-body CT and assessment of focal radioactive glucose uptake (18FDG) by cells. This is the most efficient form of staging and can provide standard uptake value information for subsequent follow-up. 14 Imaging of the neck, chest, and abdomen as well as simple blood tests for calcium and alkaline phosphatase would also suffice. Specific investigations for bone, brain, or other metastasis is usually driven by clinical suspicion rather than routine.
Pathology
Obtaining histopathological confirmation of malignancy and its subtype is critical before therapy. This is usually done before treatment decision making and the use of “frozen” or intraoperative specimens is ill-advised and not recommended. This is important because some tumors such as lymphomas are unique in that they are radiosensitive and do not require surgery whereas a diagnosis of melanoma would prompt an aggressive search for metastasis before local treatment.
Traditional teaching that “all” tumors should be biopsied in the operative setting is neither necessary nor practical. Such statements are designed to avoid disastrous consequences of biopsying an ill-defined nasal mass. As a general rule, nasal masses that present without any imaging and when the diagnosis is uncertain should not be biopsied in the office (avoiding biopsy of encephalocele or aneurysm). Likewise, masses deep within the nose (beyond the middle turbinate) should not be biopsied unless there is a special setup for controlling posterior nasal bleeding. There should also be appropriate sampling for fresh tissue (for flow cytometry), when suspicion of lymphoma exists, and needs to be available as well as formalin-fixed tissue.
Treatment
Most patients with disseminated disease rarely undergo surgical therapy. The focus of treatment is symptom control (palliation) and short courses of radiotherapy are often given. With the exception of lymphomas, chemotherapy, radiotherapy, or combinations are not curative therapies but are performed as adjuncts to surgical resection with curative intent. Radiotherapy is used to control local and regional disease. There are complex lymphatic channels in the paranasal sinuses and the skull base that prevent full excision of the lymphatic compartments during surgery. Additionally, close margins occur next to orbits, carotids, and cranial nerves that benefit from additional local therapy. Radiation therapy can be performed before surgery, termed “neoadjuvant,” or after surgery, termed “adjuvant.” When chemotherapy is added, the goal is to enhance radiotherapy, reduce tumor growth, and manage potential micro-metastasis.
Some centers use chemoradiotherapy, for sensitive tumors such as olfactory neuroblastoma, before surgery because this is generally quick to initiate and can reduce tumor size making surgery less technically demanding (less bulk and bleeding). With this approach, it does not mean that a lesser region of the skull base can be removed and the resection must still follow the originally involved anatomic sites. The down side is that the surgeon is working with postirradiated tissues with impaired healing. When performed after surgery, adjuvant therapy starts 4–6 weeks post-surgery, when there is a balance between early residual tumor cell killing and the skull base that has healed and the chance of wound breakdown is minimal.
The orbit is a critical factor is decision making and morbidity. The decision to remove the orbit is typically considered an “all-or-none” approach. It is not practical to remove portions of the orbital contents (periorbita, fat, and/or muscle) and subsequently irradiate the remaining orbital contents. This results in a nonfunctional eye with restricted ocular movements, diplopia, visual loss, poor cosmesis, and, potentially, pain. Thus, if the periorbita is not breeched on MRI or intraoperatively, the eye is spared and the close margin is acknowledged. Close observation is required and early reoperation and orbital exoneration is required if recurrence occurs.
Dura, frontal lobe, and cranial nerves are routinely removed if they are involved by tumor. These structures often bring about the morbidity imparted on the patient. However, if the eye is removed, the ipsilateral cranial nerves 1–6 can be removed with minimal impact on function. Mastication remains functional with an ipsilateral loss of the trigeminal nerve. This differs greatly to the dysfunction caused by lower cranial nerve loss (7–12). The neck generally is not empirically treated with either surgery or radiotherapy in the N0 (no clinically detectable disease in the cervical lymph nodes) presentation because the risk of subclinical disease is <20%. However, a case could be made for N0 therapy in olfactory neuroblastoma. 15 When nodal disease occurs at presentation, the neck is typically managed with a local excision with modified radical neck dissection, although there is little evidence to suggest an advantage of selective neck or radical neck dissection as an alternative.
The main complications of treatment include the early risks of cerebrospinal fluid leak, epistaxis, pneumocephalus, and meningitis. Delayed complications included sinonasal dysfunction, hypopituitarism (post-radiation therapy), post-radiation therapy cranial neuropathy, and osteoradionecrosis of the skull base.
Prognosis
The prognosis for sinonasal malignancy is generally poor. Locoregional recurrence is a critical factor because many tumors present late and wide en bloc removal is difficult. For some tumors such as olfactory neuroblastoma, adenoid cystic carcinoma, and mucosal melanoma, nodal and distant disease can occur late. Up to 15% of olfactory neuroblastomas will recur with neck nodes. 15 The overall survival for SCC and adenocarcinoma is 60% at 5 years. 13 Some radiosensitive tumors, such as olfactory neuroblastoma, have survival rates of >80% for early stage tumors. 16 Mucosal melanoma survival is worse than that for cutaneous origins with 20% 5-year rates. 17
Clinical Pearls
Sinonasal malignancies are uncommon malignancies and nasopharyngeal carcinoma is not considered part of this group.
Unilateral nasal symptoms in an older patient without a history of inflammatory airway conditions should prompt clinical suspicion.
Both CT and MRI are required to accurately stage local tissue involvement.
The involvement of the orbit, dura, brain, palate, and cranial nerves will determine the degree of surgical resection.
As with all tumors, accurate tissue diagnosis and local, regional, and distant staging must occur before treatment decisions.
Surgery and adjuvant radiotherapy are the mainstay of therapy. Close surveillance every 3 months for 2 years and then every 6 months until 5 years is standard care.