
Abstract
Background
Nasal packing is usually performed to control bleeding after endoscopic sinus surgery (ESS). Although new packing materials have been developed, they still cause pain. This study was designed to evaluate the effect of lidocaine-soaked packs on pain after ESS.
Methods
A prospective, randomized, double-blind controlled trial was conducted in 63 patients with CRS undergoing ESS. At the conclusion of the operation, 2% lidocaine-soaked biodegradable synthetic polyurethane foam and saline-soaked polyurethane foam were inserted in both nasal cavities of 31 patients and 32 control patients, respectively. The same lidocaine or saline was reapplied into the nasal packs at postoperative 8 hours. Pain was evaluated using a visual analog scale at postoperative 1, 4, 8, 16, 20, and 24 hour(s). The number of gauze that cleaned the blood around the nose was counted. Heart rate, rhythm, and blood pressures were checked preoperatively and postoperatively to evaluate the influence of lidocaine on vital signs.
Results
Postoperative pain decreased in lidocaine group at all of the postoperative time periods (p < 0.05). Lidocaine reduced postoperative bleeding at postoperative 8 and 24 hours. Changes of blood pressure from preoperative values in the lidocaine group were not different from those in the control group (p > 0.05). Heart rate in the lidocaine group was more stable than that in the control group (p < 0.05).
Conclusion
Lidocaine-soaked packs significantly reduced postoperative pain without serious changes on vital sign. These findings suggest that topical lidocaine application to nasal packs could be a useful method to reduce pain during the early postoperative period after ESS.
Nonabsorbable nasal packs have been used widely to control bleeding and to prevent accumulation of blood after ESS. Although modified techniques of nasal packing have been introduced to reduce pain during packing removal, 3 the presence of nasal packing and its subsequent removal is usually uncomfortable and painful and is often rated as the most unpleasant aspect of the ESS surgical experience by patients.4–6 Recently, absorbable packing materials are replacing nonabsorbable ones and are commonly used to reduce pain by obviating the need for removal.4,7,8 However, headache and facial pain are still common complaints in the early postoperative period, even when absorbable nasal packing is used.
Lidocaine is an amide local anesthetic used routinely as a local anesthetic to decrease pain resulting from nasal packing and surgery itself in ESS. Lidocaine has a rapid onset of action and therefore it is suitable for use in cases such as infiltration, block, and surface anesthesia. 9 However, the effectiveness of lidocaine-soaked nasal packing on early postoperative pain after ESS has never been studied.
In this study, we aimed to evaluate the effect of lidocaine-soaked nasal packing on early postoperative pain in patients undergoing ESS because of refractory CRS.
Materials and Methods
A prospective, randomized, double-blinded, placebo-controlled trial was conducted on 63 consecutive patients aged 18–65 years with CRS with or without polyps who underwent bilateral symmetric ESS from July 2011 to March 2012.
All patients were diagnosed with CRS refractory to maximal medical therapy and had evidence of significant disease on computed tomography imaging. Patients meeting inclusion criteria were enrolled consecutively into this randomized, controlled, and blinded study. Ethics approval was obtained from the Internal Review Board of the Dankook University Hospital, and informed consent was obtained from all patients before enrollment. Patients were excluded if they were <18 years old; were ineligible for informed consent; had a history of coronary artery disease, heart disease, or seizure; or had any history of intolerance to lidocaine. Patients who underwent additional septal or turbinate surgery were also excluded.
After induction of general anesthesia, the nose was prepared with topical 1:1000 epinephrine to decongest the nasal mucosa. Submucosal injection of 1:100,000 epinephrine was performed to control bleeding at the incision site at the beginning of the operation. ESS was then performed bilaterally using similar techniques by two surgeons (J.M. and Y.C). No local anesthetic was used preoperatively or intraoperatively.
The enrolled patients were randomized according to computer-generated random numbers and assigned to one of two groups. One of which was packed with 2% lidocaine hydrochloride-soaked biodegradable synthetic polyurethane foam (NasoPore; Polyganics BV, Groningen, the Netherlands; n = 31) and the other with 0.9% NaCl-soaked biodegradable synthetic polyurethane foam (n = 32) in both nasal cavities at the conclusion of the procedure. The randomization process was performed by a third party; the patients, surgeons, anesthetists, and operating room personnel were not aware of the group assignment for each patient. The quality of the surgical field regarding bleeding and visibility was also assessed at the conclusion of the procedure on a numeric rating scale introduced by Boezzart et al. 10
The same solution was reapplied into the nasal packs at the postoperative 8th hour. Patients rated their severity of subjective pain on an 11-point visual analog scale from 0 (no pain) to 10 (the worst pain they could imagine) at the 1st, 4th, 8th, 16th, 20th, and 24th postoperative hours. They also counted the number of gauze, which cleaned the blood around the nose in each time interval to evaluate the degree of postoperative bleeding. Heart rate, rhythm, and blood pressures were checked preoperatively and postoperatively to evaluate the influence of lidocaine on vital signs. Acetaminophen at 650 mg was administered when the patient needed additional analgesics, and the amount of acetaminophen administered during the postoperative 24 hour was evaluated as an objective pain parameter.
Mean subjective pain scores and bleeding scores for each group were compared between two groups. Statistical analysis was performed using the SPSS software for Windows, Version 13.0 (SPSS, Inc., Chicago, IL). An independent t-test at each time point was used to examine the difference of two groups. A value of p < 0.05 was considered statistically significant. Ji-Hun Mo and Young-Min Park contributed equally to this paper.
Results
Sixty-three consecutive patients (45 men and 18 women) with a mean age of 36.7 (SD, 16.7 years) years completed the trial. The demographics of the patient population are highlighted in Table 1. There were no statistically significant differences in the preoperative Lund-Mackay computed tomography score, duration of surgery, and the surgical field grading score between the two groups.
Patient characteristics and baseline data
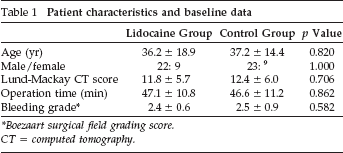
Boezaart surgical field grading score.
CT = computed tomography.
The mean pain scores at the postoperative 1, 4, 8, 16, 20, and 24 hour(s) for lidocaine group were 3.03, 2.09, 1.39, 0.87, 0.87, and 0.71, respectively. In addition, those at each time point were 6.59, 4.72, 3.78, 3.16, 2.29, and 1.81, respectively, in the control group. The lidocaine group had significantly lower pain scores than the control group at all intervals (p < 0.05 for all; Fig. 1). Patients in the control group requested a rescue drug more frequently than the lidocaine group. However, there was no significant difference in the number of patients who requested rescue drugs between the two groups (p = 0.801; Fig. 2).
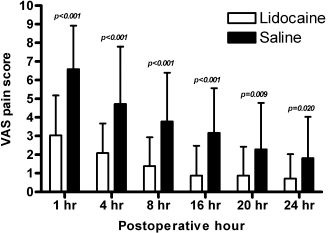
Visual analog scale (VAS) in the postoperative pain between the lidocaine (white bar) and control group (gray bar).
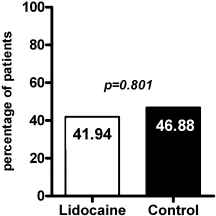
The percentage of patients who requested rescue drug. White bar, the lidocaine group; gray bar, the control group.
The lidocaine group had less postoperative bleeding, and it was significantly different at the postoperative 8 and 24 hours (p = 0.026 and 0.022, respectively; Fig. 3).
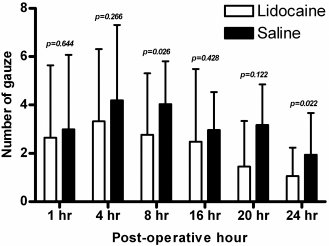
Comparison of nasal bleeding and discharge between the lidocaine (white bar) and control groups (gray bar).
Postoperative blood pressure change was not significantly different between the two groups (p > 0.05; Table 2). However, changes of heart rate in the lidocaine group were less fluctuated than those in the control group at the postoperative 1, 4, 8, and 16 hours (p = 0.007, 0.045, 0.008, and 0.004, respectively; Table 3). No adverse side effects were noted in the patient series.
Comparison of blood pressure changes from preoperative baseline values between the lidocaine and control groups
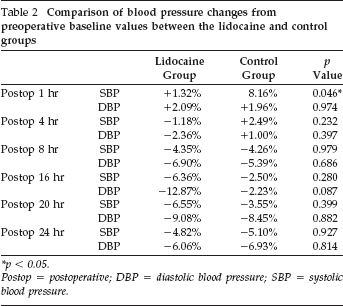
p < 0.05.
Postop = postoperative; DBP = diastolic blood pressure; SBP = systolic blood pressure.
Comparison of heart rate changes from preoperative baseline values between the lidocaine and control groups
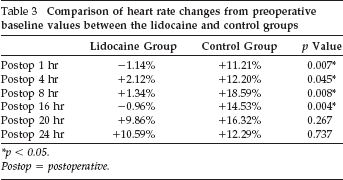
p < 0.05.
Postop = postoperative.
Discussion
Nasal packing is usually placed to prevent postoperative bleeding after ESS, because risk of delayed postoperative bleeding may be higher without nasal packing. 11 Nonabsorbable nasal packing has been the most common method to control postoperative bleeding and to prevent adhesion formation, middle turbinate lateralization, and restenosis after ESS. However, these materials cause considerable discomfort and pain to patients, both caused by the presence of the packing material and by its subsequent removal. 12 Von Schoenberg et al. 13 showed that patients undergoing endonasal surgery often consider packing removal to be the most unpleasant aspect of the perioperative experience.
Therefore, various absorbable materials have been developed and marketed to obviate the need for removal and to overcome the disadvantages of no packing. 4 However, it was reported that even the absorbable pack causes significant pain and discomfort compared with the traditional nonabsorbable nasal pack in the duration of nasal packing. 14
Hence, we used lidocaine-soaked absorbable nasal packing to investigate the analgesic effect of lidocaine. Postoperative pain in ESS results from the surgical sinus wound and the nasal pack itself, and its management is one major goal of ESS. The present study showed that the topical lidocaine application reduced pain scores at all postoperative intervals and lidocaine is assumed to provide analgesia through surface effect and diffusion into the surgical mucosal wound.
Several previous studies have attempted to assess the effect of topical lidocaine application on postoperative pain. Lavy et al. 15 evaluated the effectiveness of 4% lidocaine solution in reducing pain associated with removal of Merocel packs (n = 34). They found that the rehydration of the nasal package with 4% lidocaine solution before removal of nasal packs reduced the level of discomfort compared with the side rehydrated with saline, although this reduction did not reach statistical significance. Kuo et al. 12 assessed the effect of topical 5% lidocaine ointment on reducing the pain in patients with septal surgery and showed that postoperative pain at postoperative 3 hours was halved in patients receiving a lidocaine-impregnated nasal pack compared with those having a standard Vaseline gauze pack. Pain scores at postoperative 6 hours and at pack removal were also reduced without reaching statistical significance. Buchanan et al. analyzed 62 patients who received either bupivacaine- or saline-soaked Merocel packs in bilateral nasal surgery and showed that bupivacaine, a long-acting amide local anesthetic, significantly reduced postoperative pain at the 2, 4, and 6 hour, but not on pack removal. 16 They enrolled patients with heterogeneous nasal surgeries including ESS, polypectomy, turbinectomy, septoplasty, and other various procedures and that might explain the difference with our results.
This study also showed that the lidocaine group had less postoperative bleeding until 24 hours and with statistical significance in 4th-to 8th-hour and 20th- to 24th-hour intervals. Less postoperative bleeding could be explained by the effects of lidocaine on heart rate and pain. Lidocaine has been reported to reduce heart rate. 17 Many comparative studies showed less bleeding in patients with decreased heart rate, although the effect of heart rate on bleeding has been underestimated.10,18,19 The present study evaluated the sympathetic responses by measuring blood pressures and heart rate and showed blunted sympathetic responses in the lidocaine group. Especially, heart rate was significantly decreased in the lidocaine group until postoperative 16 hours. These findings could suggest that lidocaine-soaked nasal packing effectively induced pain reduction, followed by blunting of the sympathetic tone and decreased postoperative bleeding.
Lidocaine is generally used in several situations including topical anesthesia, arrhythmia, etc.; however, it is contraindicated in the following conditions; a known history of hypersensitivity to local anesthetics of the amide type; concurrent treatment with quinidine, flecainide, disopyramide, or procainamide (class I anti arrhythmic agents); prior use of amiodarone hydrochloride; hypotension not caused by arrhythmia; bradycardia; and porphyria, especially acute intermittent porphyria. In addition, even topically applied lidocaine should be used with caution in patients with hypovolemia or dehydration, myasthenia gravis, shock, or cardiac disease. Patients with impaired cardiac function, particularly atrioventricular block, may be less able to compensate for functional changes associated with prolonged atrioventricular conduction (i.e., PR or QT prolongation) caused by lidocaine. 20 In our study, none of our patients met the aforementioned criteria.
This study has some limitations. First, plasma concentrations of lidocaine were not measured to evaluate the systemic absorption of topical lidocaine. Further investigation of plasma concentrations will be needed to achieve maximal clinical benefit without major side effects. Second, the sample size of the study was relatively small.
Despite those limitations, this is the first double-blind placebo-controlled study to assess the effect of lidocaine-soaked absorbable nasal packs on the early postoperative pain after ESS with the largest sample size as far as we know.
Conclusion
Lidocaine-soaked nasal packing reduced the early postoperative pain without serious complications in patients who underwent ESS. Therefore, topical lidocaine application to nasal packs could be a useful method to reduce early postoperative pain and to reduce bleeding.
Footnotes
Acknowledgments
The present research was conducted by the research fund of Dankook University in 2011.