
Abstract
Background
In recent decades, the amount of data about allergic rhinitis (AR) in Korean National Health Insurance Service has increased.
Objective
To investigate the prevalence and quality of sensitized allergens of AR in Korean children and adolescents.
Methods
This study obtained the results of the Korean International Study of Asthma and Allergies in Childhood questionnaires and the skin-prick test (SPT) results of 14,356 students who participated in a health screening from 2010 to 2014. AR was defined as one with current symptoms of AR with at least one or more positive results of an SPT with inhalant allergens.
Results
The prevalence of AR in children was 20.8%. Positive rates of the allergen group were 87.3% for house-dust mites, 37.0% for pollen, 12.4% for mold, and 8.4% for pets. The common allergens in descending order were Dermatophagoides pteronyssinus, Dermatophagoides farinae, Betula, Humulus, Alnus, and Alternaria. As the children became older, pollen-sensitization rates tended to increase (p value for trends, <0.001). In metropolitan and middle inland areas, weed pollen was the most common pollen. The rates of tree-pollen sensitization were the highest at the seaside and in the southern inland. The most common comorbid allergic diseases associated with AR were pollen allergy and allergic conjunctivitis at 37.0% and 34.5%, respectively.
Conclusions
This was the first study conducted in Korea to investigate the prevalence of AR in the general population by using both questionnaires and SPTs. The allergens used for the SPTs were chosen based on the common allergens in this study, and this current pollen data will contribute to establish the cause of increasing AR prevalence in Korea.
Allergic rhinitis (AR) is a common problem during childhood. AR is defined as an immunologic response modulated by immunoglobulin E and characterized by sneezing; rhinorrhea; nasal congestion; and pruritus of the nose, eyes, oral mucosa, or face. 1 Patients with AR usually experience a significant emotional burden and restrictions to daily life, sleep disorders, and impairment in activities and social functioning. 2
Reports that span recent decades indicate that the prevalence of AR seems to be increasing.3,4 In Korea, the prevalence of AR has also been increasingly associated with improvements in general hygiene, air pollution, pollen, and Westernized lifestyle and environments.5,6 An annual report of the National Health Insurance Service of Korea demonstrated that the medical costs of AR treatment is on the rise in children ages ≤18 years, and the insurance burden has more than doubled during the past 10 years from 57.3 million in 2004 to 131.7 million in 2013.7,8 Despite recognition that AR is a global health problem, 4 insufficient epidemiologic data persist, and more data are needed with regard to etiologic allergens.
Many national or multinational studies have increased our knowledge regarding the prevalence of AR and the possible risk factors. 9 However, studies that used questionnaires may only overestimate the true prevalence of AR because many patients poorly perceive nasal symptoms of AR; some exaggerate symptoms, whereas others tend to dismiss the disease. 10 Because previous reports on objective tests for immunoglobulin E-mediated allergy investigated patients who had visited allergy clinic, there was concern about sample bias leading to the overinflated positive rate of the test. 11 Thus, this study was designed to investigate the prevalence of sensitized allergens in the unselected general population of children and adolescents living in metropolitan, seaside, middle inland, and southern inland in Korea, based on both questionnaires and skin-prick tests (SPT). Interestingly, few Korean data are available of children to evaluate the prevalence of comorbidities with AR, asthma, atopic dermatitis, allergic conjunctivitis, food allergy, and pollen allergy. Therefore, this study aimed to determine the prevalence of comorbidities by focusing on AR with other allergic diseases to compare these results with previous literature.
Methods
Subjects and Case Definition of AR
The subjects included were 14,356 children and adolescents in metropolitan, seaside (Busan), middle inland (Chungbuk), and southern inland (Gwangju) in Korea from 2010 to 2014. We obtained the results of the Korean International Study of Asthma and Allergies in Childhood (ISAAC) questionnaires and SPTs. AR was defined as having current symptoms of AR with at least one or more positive results of an SPT. The institutional review board of Inha University Hospital approved this study.
Questionnaire
From the questionnaire, basic personal data and information related to the prevalence of allergic diseases for each subject were obtained. Because the clinical manifestations of allergic diseases vary, the prevalence can be demonstrated differently, depending on how the disease is defined. However, it is possible to assess and compare the prevalence of allergic diseases across the world by using the ISAAC questionnaire. 12 For AR, a question such as, “In the past 12 months, have you had a problem with sneezing or a runny or blocked nose when you did not have a cold or the flu?” was asked. If the response was “yes,” then it was considered as leaning toward “the prevalence of allergic rhinitis symptoms currently.” This study used the Korean version of the ISAAC questionnaire to determine the presence of symptoms of AR. 13
Allergens Used in SPTs
Preschool children and elementary school students were tested for 16 and 21 common inhalant allergens, respectively, whereas middle and high school students were tested for 27 inhalant allergens. The 29 allergens included a positive control (1% histamine), negative control (normal saline solution), house-dust mites (HDM) (Dermatophagoides pteronyssinus, Dermatophagoides farinae), pollen (tree: Cryptomeria [Japanese cedar], Pinus [pine], Salix [willow], Acer [maple], Betula [birch], Quercus [oak], Alnus [alder], Ulmus [elm]; weed: Ambrosia [ragweed], Artemisia [mugwort], Humulus [Japanese hop], Chenopodiaceae [fat hen], Plantago [plantain]; grass: Cynodon [Bermuda grass], Phleum [timothy grass], Lolium [rye grass], Dactylis [orchard grass], Poa [meadow grass], Anthoxanthum [vernal grass]), mold (Penicillatum, Aspergillus, Cladosporium, and Alternaria), and pet (dog hair and cat fur). The 21 allergens used on elementary school students were the same as the above mentioned, with the exception of Ulmus, Plantago, Lolium, Dactylis, Poa, and Anthoxanthum. Further, the 16 allergens were used on preschool children except for Cryptomeria, Salix, Chenopodiaceae, Cynodon, and Phleum, which was less than the number applied on the elementary school students. The positive and negative controls and all the allergens were manufactured by Allergopharma (Hamburg, Germany) except Chenopodiaceae. The reagents for Chenopodiaceae were manufactured by Shin Kwang New Drugs Company (Seoul, Korea).
In this article, the pollen name was indicated by the scientific name according to the internationally accepted notation of the International Code of Botanical Nomenclature, and the English name was written in parentheses to facilitate comprehension of the scientific name. Generic names that were difficult to classify morphologically were written as family names.
SPTs
SPTs were performed as follows. Researchers sterilized the forearms of students with an alcohol swab and introduced the reagent at constant 2.5-cm intervals. The cutting edge of the lancet was held flush with the skin, and pricks were administered with consistent intensity and depth. After 15 minutes, the results were read according to wheal and flare size. A wheal of >3 mm in diameter and larger than a negative control, produced by the positive control (1% histamine) was considered as a positive result. For middle and high school students, SPTs were carried out with 14 and 15 types of allergens on each arm. For preschool age and elementary school students, 10 allergens were pricked on one arm and the remaining allergens on the other arm. To exclude errors related to the time of day of the examination, all the examinations were performed in the morning by trained inspectors.
Comorbidity
Comorbidities of AR, asthma, atopic dermatitis, allergic conjunctivitis, food allergy, and pollen allergy were assessed, based on the presence of these disorders and positive answers to the written question of “In the last 12 months, has your child had symptoms?” (symptom, past 12 months) except for pollen allergy with a positive result of an SPT.
Statistics
All of the statistical data were calculated by using SPSS version 17.0 (SPSS Inc., Chicago, IL). To analyze differences in the prevalence of AR and the positive rate of allergens according to age, sex, and geographic distribution, a Pearson χ 2 test was performed. A Cochran-Armitage test was used to perform trend analysis of positive rates of sensitized allergens in the age groups. A p value of <0.05 was considered to be statistically significant.
Results
Demographic Characteristics and Prevalence
A total of 14,356 students as a total population included 8027 students from metropolitan areas (4058 girls and 3969 boys), 2598 students from the seaside (1151 girls and 1447 boys), 1483 students in the southern inland (798 girls and 685 boys), and 2248 students from the middle inland (1221 girls and 1027 boys) were sorted by geographic distribution (Fig. 1). A total of 1306 preschool children, 5053 elementary school students, 4322 middle school students (first to second grade, 13 to 14 years old), and 3675 high school students (first grade, 16 years old) were classified by age. A total of 2991 students (1255 girls and 1766 boys) were defined as positive for AR among the total participants, and the total prevalence of AR was 20.8% (16.9% girls and 24.8% boys; p < 0.001), and the prevalence of AR based exclusively on the questionnaire was 43.8% (Table 1).

Geographic distribution of study subjects in Korea.
The prevalence of allergic rhinitis in students
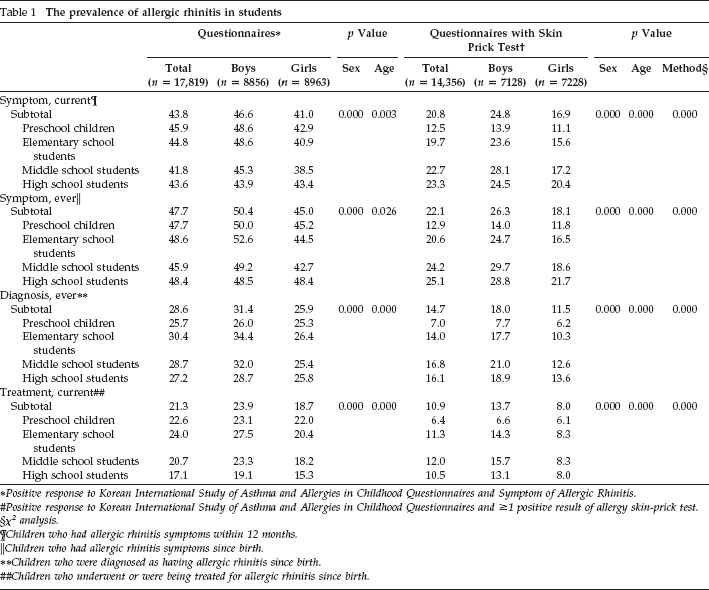
Positive response to Korean International Study of Asthma and Allergies in Childhood Questionnaires and Symptom of Allergic Rhinitis.
Positive response to Korean International Study of Asthma and Allergies in Childhood Questionnaires and ≥1 positive result of allergy skin-prick test.
χ2 analysis.
Children who had allergic rhinitis symptoms within 12 months.
Children who had allergic rhinitis symptoms since birth.
Children who were diagnosed as having allergic rhinitis since birth.
Children who underwent or were being treated for allergic rhinitis since birth.
Comparison of Sensitized Allergens by Sex
Positive rates of sensitized allergens in groups of children with AR were 87.3% for HDM, 37.0% for pollen, 12.4% for mold, and 8.4% for a pet (Table 2). The common allergens in descending order were D. pteronyssinus (76.8%), D. farinae (68.1%), Betula (10.8%), Humulus (10.5%), Alnus (9.7%), Alternaria (8.9%), Artemisia (8.6%), and cat fur (7.4%). No statistical differences in the positive rates of HDM were observed in girls versus boys (87.3% versus 87.2%; p = 0.915). The common pollen allergens were Betula, Humulus, Alnus, Artemisia, and Quercus. The sensitization rates of total pollen allergens were significantly higher in boys versus girls (39.1% versus 33.9%; p = 0.003). Also, mold and pets showed a tendency to be higher in boys than in girls, but there were no statistically differences (p = 0.132 and p = 0.145, respectively) (Table 2).
Sensitized allergens, by sex, in children with allergic rhinitis*
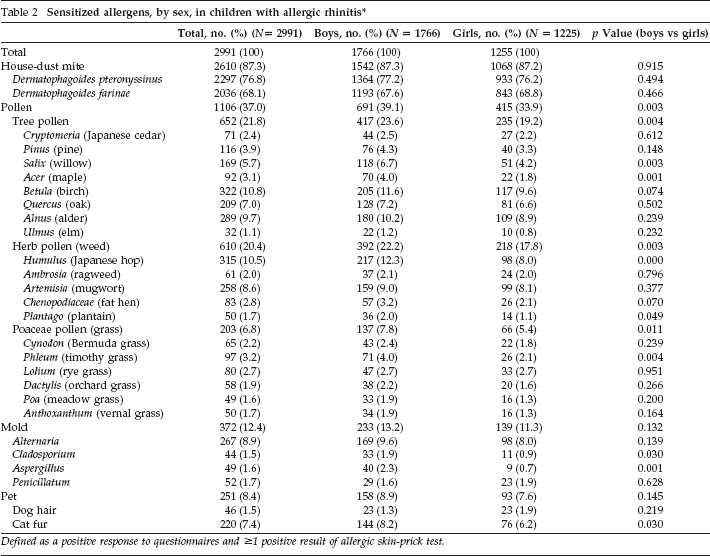
Defined as a positive response to questionnaires and ≥1 positive result of allergic skin-prick test.
Comparison of Sensitized Inhalant Allergens by Age Group
Six-year-old elementary school students were divided into two groups, lower and higher, depending on the respective 3 years of school grade, grades 1-3 and 4-6. As the children became older, from preschool to high school age, no statistical differences in the positive rates of HDM were observed (p = 0.885), yet the sensitization rates of D. farinae tended to increase (p = 0.003). The rate of pollen sensitization had markedly increased in all kinds of pollen (p for trend of < 0.001) (Fig. 2; Supplemental Material 1).
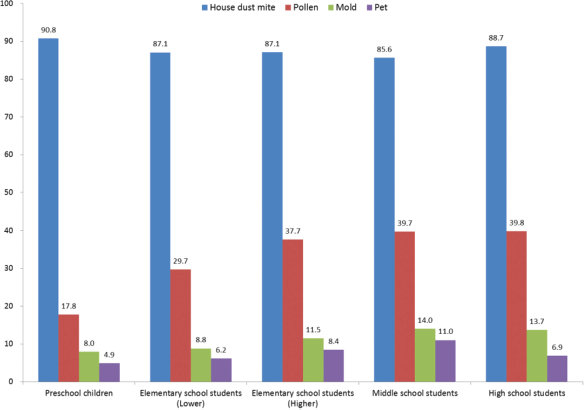
Sensitized allergens in children with allergic rhinitis* by age group.*, Children who have allergic rhinitis symptoms within 12 months plus ≥1 positive result(s) of allergic skin prick test.
Comparison of Sensitized Inhalant Allergens by Geographic Region
The HDM allergen was prevalent at the highest rate among the four regions: 87.9% in metropolitan, 86.7% at the seaside, 89.4% in the southern inland area, and 84.3% in the middle inland area. In the metropolitan and middle inland areas, weed was the most common pollen at 21.7% and 28.9%, respectively. The rates regarding tree pollen were the highest at the seaside (31.1%) and in the southern inland area (28.1%): at 21.7% for Betula, 19.5% for Alnus, and 10.4% for Quercus at seaside; and 14.0% for Betula, 12.0% for Alnus, and 6.9% for Cryptomeria in the southern inland area. Mold registered highest in the middle inland area and was lowest at the seaside (Table 3).
Sensitized allergens, by geographic region, in children with allergic rhinitis *
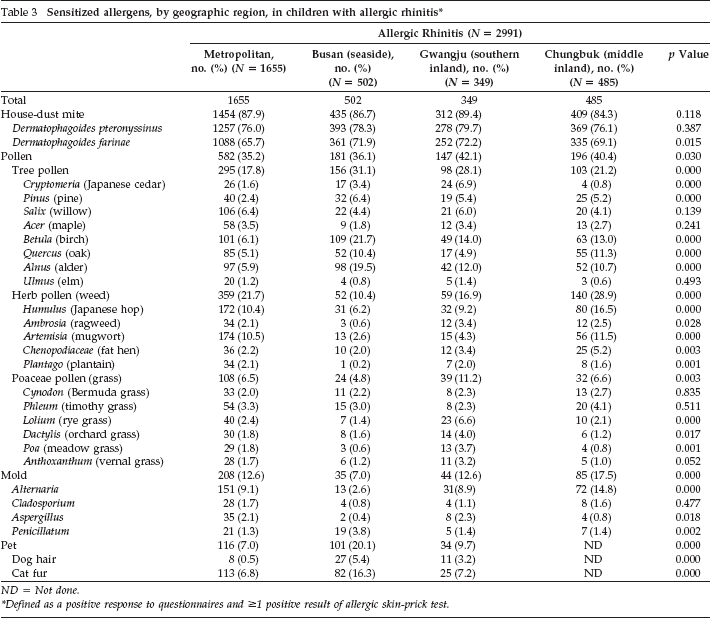
ND = Not done.
Defined as a positive response to questionnaires and ≥1 positive result of allergic skin-prick test.
Comorbid Diseases with AR
Comorbid allergic diseases associated with AR were pollen allergy (37.0%), allergic conjunctivitis (34.5%), atopic dermatitis (22.0%), asthma (14.0%), food allergy (10.5%) (Fig. 3).
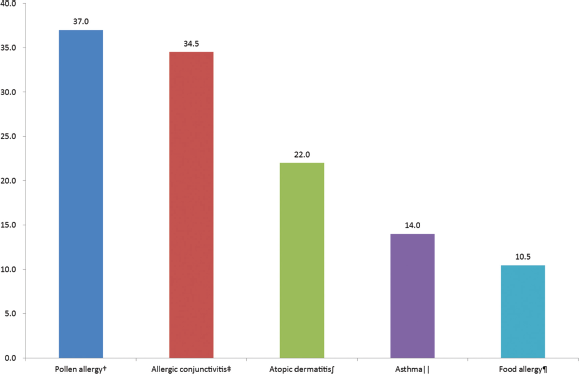
The comorbid diseases with allergic rhinitis.* *Children who have allergic rhinitis symptoms within 12 months plus ≥1 positive result of allergic skin prick test; †children who have pollen allergy symptoms within 12 months plus ≥1 positive result of allergic skin prick test; ‡children who have allergic conjunctivitis symptoms within 12 months; ∫children who have atopic dermatitis symptoms within 12 months; ‖children who have asthma symptoms within 12 months; ¶children who have a food allergy symptoms within 12 months.
Discussion
Analysis of results of this study indicated that the prevalence of AR in children and adolescents was 20.8%, which was even lower than the values reported previously as in the prevalence of an investigation based on a questionnaire only. Self-reported prevalence of 43.6% in Italian adolescents, 14 a telephone-survey prevalence of 33.3% in French patients ages 18-45 years, 15 and lifetime prevalence of 32.8% in school children from the northeast of England 16 are comparable studies. In the ISAAC phase I study, the highest prevalence rates for rhinitis were observed in parts of western Europe, North America, and Australia, whereas the lowest rates were found in parts of Eastern Europe and south and central Asia. 3
The ISAAC phase III analyses revealed that the prevalence rates had increased, with prevalence rates of 1.8 to 24.2% in children ages 6 to 7 years and 1.0 to 45% in 13- to 14-year-old children. 17 In Japan, an epidemiologic study revealed a marked increase in the prevalence of AR between 29.8% in 1998 and 39.4% in 2008. 18 Compared with this study, the difference raised with a previous study was that only a questionnaire was used and that responses for AR may have overestimated the real prevalence of the disease. 19 In a study on the general population in European adults, the clinically confirmable prevalences were 16.9% in Italy (n = 1602), 20.6% in Germany (n = 1613), 21.5% in Spain (n = 1600), 24.5% in France (n = 1606), 26.0% in the United Kingdom (n = 1625), and 28.5% in Belgium (n = 1602), with an overall value of 23% among a total of 9646 subjects, which was much lower than self-aware prevalences, which ranged from 60.6 to 83.8%. 20 The prevalence of AR based exclusively on the questionnaire was also 43.8% in this study (Table 1). To estimate the real prevalence of AR, the study with an objective measurement on etiologic inhalant allergens should be conducted to confirm subjective questionnaires.
The age effect on the prevalence of AR in this study was apparent because the incidence of AR increased significantly as children grew from childhood into adolescence (Supplemental Material 1). It was thought that this trend was caused by sensitization rates of pollen that had increased according to age (Fig. 2). In the ISAAC phase III study, the prevalence of allergic rhinoconjunctivitis symptoms was found to be higher in the 13- to 14-year-old age group versus the 6- to 7-year-old age group: 15.0% versus 6.9% in Germany, 15.3% versus 10.1% in the United Kingdom, and 16.9% versus 5.8% in Belgium. 21 In a prospective study that followed up German children from ages 9 to 11 years until ages 15 to 18 years, the incidence of AR increased from an initial rate of 7% to 14%. 22 In the recent National Health and Nutrition Examination Survey, which assessed 7398 patients, 4492 of whom were older than 20 years of age in the United States, the 12-month prevalence of rhinitis for the entire cohort was 23.5%, with a peak of 31.3% in patients 40 to 49 years of age. 23
In addition, as the children became older, from preschool to high school age in the current study, the positive rates of pollen markedly increased in regard to all kinds of pollen. In a study in western Europe, the crude odds ratio of outdoor allergen exposure was 3.573 (95% confidence interval) for a diagnosis of AR, whereas that of indoor allergen exposure was 1.367. 11 Thus, in this study, the distinction between indoor and outdoor allergens was thought to contribute to the age differences. Further, it should be considered that radical differences of AR prevalence between the sexes were caused by positive rates of outdoor allergens, e.g., pollen and not that of indoor allergens, e.g., HDM, in the current research. Although the exact cause of the difference of AR prevalence may be according to age or sex, pollen was thought to be a key inhalant allergen of AR in this study.
This study revealed that common pollens as allergens were weed pollen (21.7%), tree pollen (17.8%), and grass pollen (6.5%), followed by birch, Japanese hop, alder, mugwort, oak, willow, pine, timothy grass, maple, and rye grass in descending order. In the Swiss Study on Air Pollution and Lung Diseases in Adults, the highest rate of positive SPTs was observed for 12.7% of the study population for grass pollen, followed by 7.9% for birch, 3.8% for cat, and 2.8% for dog from a random sample of 8357 adults ages 18 to 60 years. 24 In a National Health and Nutrition Examination Survey III study of 10,508 subjects ages 6 to 59 years, the prevalences were 26.9% for perennial rye, 26.2% for short ragweed, 26.1% for German cockroach, 18.1% for Bermuda grass, 17.0% for cat, 15.2% for Russian thistle, 13.2% for white oak, 12.9% for Alternaria alternata, and 8.6% for peanut. 25
In Japan, the number of patients with Japanese cedar pollen allergy has increased, from 16.2% in 1998 to 26.5% in 2008. 26 This study revealed that the positive rates of tree pollen and weed pollen were more common than that of grass pollen, unlike the results in the Swiss Study on Air Pollution and Lung Diseases in Adults and the National Health and Nutrition Examination Survey. In Korea, the positive rate of SPT for Japanese cedar was known to be rare in the inland regions. 5 Nevertheless, the high prevalence rate of 6.9% was investigated in the southern inland for the first time. In a previous domestic study in Korea, the positivity of Alternaria and of other molds was 10% and 2-4%, respectively. 27 In the current study, positivity of mold was the highest at 14.9% in the middle inland and was the lowest 2.6% at the seaside, and Alternaria was the leading mold allergen in most regions, except for a result of 3.8% of Penicillatum at the seaside.
This study revealed that comorbid allergic diseases associated with AR were pollen allergy (37.0%), allergic conjunctivitis (34.5%), atopic dermatitis (22.0%), asthma (14.0%), and food allergy (10.5%). In the French part of the European Community Respiratory Health Survey, current asthma was reported in 22.5% of the subjects with rhinitis and 4% of the subjects with no rhinitis. 28 In a part of the birth cohort study that enrolled 3754 healthy, full-term babies in Norway, the most common comorbidity to rhinitis was conjunctivitis symptoms reported in 75.6% of the study population. 29 In a study to analyze the comorbidities for AR in 1275 Spanish children, the most frequent comorbidities were conjunctivitis (53.6%), asthma (49.5%), atopic dermatitis (40%), rhinosinusitis (26.1%), otitis media (23.8%), and adenoid hypertrophy (17.3%). 30 Because this study was conducted in the general population, it was predicted that the prevalence of comorbid allergic disease was underestimated versus other studies with patients who had visited a hospital. In addition, the prevalence of comorbid diseases with AR was expected to increase to European levels as in the above studies, when considering previous domestic reports in Korea.5,31
There were limitations with this study in that the numbers of tested allergens did not match among each age group. However, the reagents of the SPTs were selected based on previous age prevalence in Korea. 5 Furthermore, this study found that most pollen-positive rates revealed an increasing trend as children became older.
Conclusion
The strength of the research was that this was the first nationwide study conducted in Korea to investigate the prevalence of AR in the general population by using both questionnaires and SPTs. The correlation between AR and pollen as an etiologic allergen may be determined by further research on the prevalence of AR. This study will contribute to the establishment of the causes of increasing AR prevalence and to the promotion of national health in Korea.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article
Acknowledgments
The Korean version of ISAAC was provided by the Korean Pediatric Allergy and Respiratory Society.
{kind=link}