
Abstract
Background
Previous research suggested that the biofilm of Staphylococcus aureus contributes greatly to the recalcitrant nature of chronic rhinosinusitis (CRS). However, the lack of a simple and stable animal model limited further study in this field. The aim of this study was to ate a convenient animal model of S. aureus biofilms in the maxillary sinus of rabbit.
Methods
New Zealand white rabbits were used as model animals and incised vertically along the median line of the nasal dorsum to expose the anterolateral wall of maxillary sinus, on which a 1.5-mm-diameter hole was drilled to enter the sinus cavity. Through the hole, a piece of gelatin sponge was inserted and then inoculated bacterial suspension into the maxillary sinus. One to 8 weeks after the surgery, the sinus mucosa were harvested and examined with scanning electron microscopy (SEM) and hematoxylin and eosin (H&E) staining.
Results
All rabbits tolerated the surgical procedures and had developed sinusitis by the time they were killed. SEM revealed that biofilms were presented in 100% of rabbits who had bacteria infected for ≥2 weeks, during which the ciliated epithelial cells were encapsulated and gradually destroyed. H&E staining revealed morphological changes of the epithelial cells and infiltration of inflammatory cells in subepithelial layer, which showed a strong correlation with the results of SEM.
Conclusion
This biofilm model of sinusitis avoids excessive damage to the nasal cavity and sinuses of the rabbits. It may be a desirable animal model for studying the pathogenesis and eradication strategies of bacterial biofilms in sinusitis.
Since 2004, bacterial biofilms have been consistently identified on the mucosal surface of patients with chronic rhinosinusitis (CRS),2–9 and they have been associated with more severe disease preoperatively and poorer outcomes after endoscopic sinus surgery.10,11 Staphylococcus aureus is the most common bacteria isolated from CRS patients12–14 and also the most common biofilm-forming organism of CRS patients.9,15 Therefore, S. aureus biofilms were believed to play an important pathological role in the incidence, maintenance, and ongoing burden of CRS. 16 Some experts believed that future studies evaluating therapeutic intervention should specifically target S. aureus biofilms.17,18
To facilitate the study of biofilms in sinus disease, researches on the animal models are currently increasing. In 2005, Perloff and Palmer published an animal model of sinusitis by using Pseudomonas aeruginosa as the inciting organism. 19 Subsequently, Wormald et al. presented an S. aureus biofilms model in sheep. 20 Although these two animal models were all successful, the modeling procedures were somewhat complicated.
For these reasons, it would be desirable to have a biofilm model of sinusitis that is easier to operate and has stable results with more representative pathogens. The aim of this study was to provide a more optimal model of biofilm-related sinusitis in rabbits by using S. aureus as the pathogen and to observe the development of S. aureus biofilms in the paranasal sinuses.
Materials and Methods
Animals
Forty-five New Zealand white rabbits (2.5–3.5 kg) were provided by the Laboratory Animal Center of Fudan University and caged individually in an air-conditioned room with dark-light cycles of 12 hours and free access to water and food. The rabbits were randomly divided into nine groups, including four model groups, four negative control groups, and one blank control group, five rabbits in each group. All of the procedures were performed with permission of the Animal Care and Use Committee of Fudan University (Shanghai, China).
Bacterial Preparation
Twenty-one clinical isolates of S. aureus, Sa001-Sa021, were screened for one with relatively strong biofilm formation capacity. Biofilm-forming ability was examined in 96-well flat-bottom polystyrene microtiter plates (Corning, Inc., Corning, NY) using a traditional crystal violet biofilm assay.21,22 If the optical density (OD) value was >0.12, the isolate was deemed to be biofilm positive. 23 In our experiment, Sa006 was selected as the experimental strain, in which its OD value was 0.46, the largest among all of the tested strains. A single colony of Sa006 was inoculated in tryptic soy broth supplemented with 0.5% glucose (TSBg), incubated at 37°C overnight with shaking. Next, the bacterial suspension was diluted 200-fold with TSBg and kept on ice for further use.
Surgical Procedure
The right maxillary sinus of rabbits was chosen as the model side. Rabbits were anesthetized with an intramuscular injection of ketamine (50 mg/kg) combined with diazepam (5 mg/kg). Then, the nasal dorsum was shaved and prepared in a sterile fashion. A dose of 1 mL of lidocaine (1%) with epinephrine (1:100,000) was injected over the nasal dorsum in a subcutaneous fashion. Skin and periosteum was incised vertically along the median line of the dorsum, and the distance from the midpoint of incision to the anterior nostril was ∼2.8 cm. A laterally based flap of periosteum ∼0.5–0.8 cm in width was elevated from the midline to the right side, and then a small hole, 1.5 mm in diameter, 0.4 cm laterally to the midpoint of incision, was drilled to enter the maxillary sinus (Fig. 1 a). After that, a cylindrical absorbable gelatin sponge kneaded to size was inserted into the maxillary sinus through the hole (Fig. 1 b), and then 0.5 mL of previously prepared bacterial suspension was inoculated into the sinus with a syringe. Next, the periosteal flap was replaced and fixed in place by apposition suture, and the skin incision was closed with interrupted suture. For the negative control groups, the animals only underwent maxillotomy and Gelfoam placement, without bacterial inoculation. The rabbits in the blank control group did not receive any treatment.
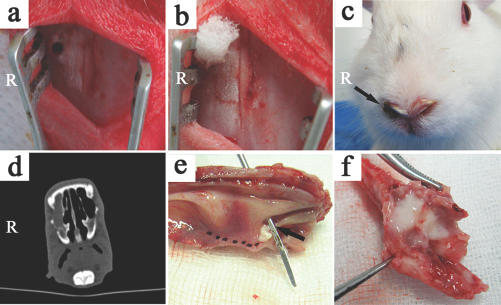
The key steps of modeling procedure and evidence of sinusitis. (a) Incision and the hole drilled on the anterolateral wall of the maxillary sinus. (b) Insert gelatin sponge into maxillary sinus. (c) Puric crust attached to the front nostril of the model side (black arrow), the incision has completely healed. (d) Computed tomography scan revealed right maxillary sinusitis. (e) The inner surface of rabbit maxillary sinus, pus located on the ostium (black arrow). (f) Mucopurulent secretions within the maxillary sinus (cut along the dotted line shown in panel e; panels c–f, at 4 weeks postsurgery; R, right).
After surgery, the animals were still caged individually and were observed daily for vitality and signs of infections, without any special care regimen. To avoid antibiotics' affecting on the biofilm formation process, no antibiotics were used in this experiment.
Animal Death and Tissue Harvest
For the model groups and negative control groups, the maxillary mucosa was harvested at each of the following time points after the operation: 1, 2, 4, and 8 weeks. The rabbits in the blank control group were killed at the end of the whole experiment. Before death, two rabbits were randomly selected from each group and anesthetized with ketamine (50 mg/kg, intramuscularly) for computed tomography scanning (window width, 1500 H; window level, 500 H; thickness, 0.8 mm) to observe the occurrence of sinusitis. After that, the rabbits were intraperitoneally anesthetized with 10% chloral hydrate (350 mg/kg) and locally with lidocaine (1%). The skin and periosteum were opened to expose the entire anterolateral wall of the maxillary sinus, and then the maxillary sinuses were resected and opened with a scissors. The sinus mucosa was carefully removed, immediately placed in normal saline, and washed thoroughly to remove blood clots, mucous, and debris. Then, the specimens were divided into two segments and subsequently placed into 4% paraformaldehyde for routine histological examination by hematoxylin and eosin (H&E) staining and into 2.5% glutaraldehyde for scanning electron microscopy (SEM) specimen preparation. After that, animals were killed with air injection though the ear vein.
H&E Specimen Preparation and Analysis
The mucosal specimens were fixed in 4% paraformaldehyde for 48 hours and then embedded into paraffin blocks according to routine procedures. The blocks were cut to 5-μm sections and stained with H&E using standard procedures. Next, the stained sections were analyzed by light microscopy using a Nikon Eclipse 80i epifluorescence microscope (Nikon, Tokyo, Japan). Images were acquired with a CCD digital camera at 400x magnification.
SEM Specimen Preparation and Analysis
The specimens were initially fixed for 24 hours in 2.5% glutaraldehyde at 4°C, and then rinsed three times with 1x phosphate-buffered saline and fixed with 1% osmium tetroxide for 2 hours. They were then rinsed three times again with phosphate-buffered saline and then dehydrated through a graded ethanol series as follows: 50, 70, 90, and 100%, 15 minutes in each concentration. The specimens were then immersed in a mixture of 100% ethanol and isoamyl acetate (2:1), and then in pure isoamyl acetate, 15 minutes each time. All specimens were dried in carbon dioxide critical point dryer and sputter coated with gold, examined with a SU8010 SEM (Hitachi, Tokyo, Japan) at an accelerating voltage of 10 kV. Images were taken from 2000∼5000x magnification. Structures characterized by water channels, three-dimensional structure, and matrix-embedded spherical bodies were evaluated for evidence of bacterial biofilms. 6
Results
In general, the rabbits tolerated both the surgical procedure and the S. aureus inoculation well during the whole experiment. Five of the 20 model rabbits developed subcutaneous abscesses, which were just confined to the dorsum and had no effect on the rabbits' vital signs and living habits. All of the rabbits in the model groups had purulent nasal discharge that lasted for about 1 week; after that, there remained some puric crust attached to the right front nostrils (Fig. 1 c). And they all developed sinusitis that was confirmed by computed tomography CT and existence of mucopurulent secretions in the maxillary sinus at the time of death (Fig. 1, d–f); however, for the negative control groups, only eight animals had slight runny nose, and no rabbit suffered from subcutaneous abscess. The Gelfoam residues had been found in the maxillary sinus at 1 and 2 weeks after surgery; however, at 4 and 8 weeks, the Gelfoam completely disappeared, and no pus was found in the maxillary sinus.
For the model groups, H&E staining showed that the sinus mucosa had undergone dramatic histological changes. In the 1-week group, the nasal mucosa was swollen with some inflammatory cells infiltrated in the lamina propria and accompanied by submucosal gland hypertrophy and goblet cell hyperplasia with nuclei lateralization, indicating greater mucus production (Fig. 2 a). A sharp increase of inflammatory cells, including lymphocytes, neutrophils, eosinophils, and plasma cells, in the subepithelial layer and lamina propria was observed at 2 weeks (Fig. 2 b). At 4 weeks, there were also massive inflammatory cells that infiltrated in the subepithelial layer and lamina propria, but the epithelial cells became swollen with vacuole-like large nuclei, and many of the epithelial cells appeared damaged or disintegrated. However, the cells contours were visible and the basal lamina was continuous (Fig. 2 c). At 8 weeks, mucosal swelling and infiltration of inflammatory cells did not change dramatically, but the epithelial cells appeared totally or near totally denudated from the basal lamina. The basal lamina was relatively intact for the most part but not present in some places (Fig. 2 d). In contrast to the model groups, the rabbits in the negative control groups only had some inflammatory cells (mainly neutrophils) infiltrated in the subepithelial layer at 1 and 2 weeks after surgery (Fig. 2, e and f). The histological features of 4- and 8-week negative control groups (Fig. 2, g and h) were similar with the blank control one, which was characterized as normal respiratory mucosa with columnar ciliated epithelium and no significant inflammatory cells infiltrated in the subepithelial layer (Fig. 3 a).
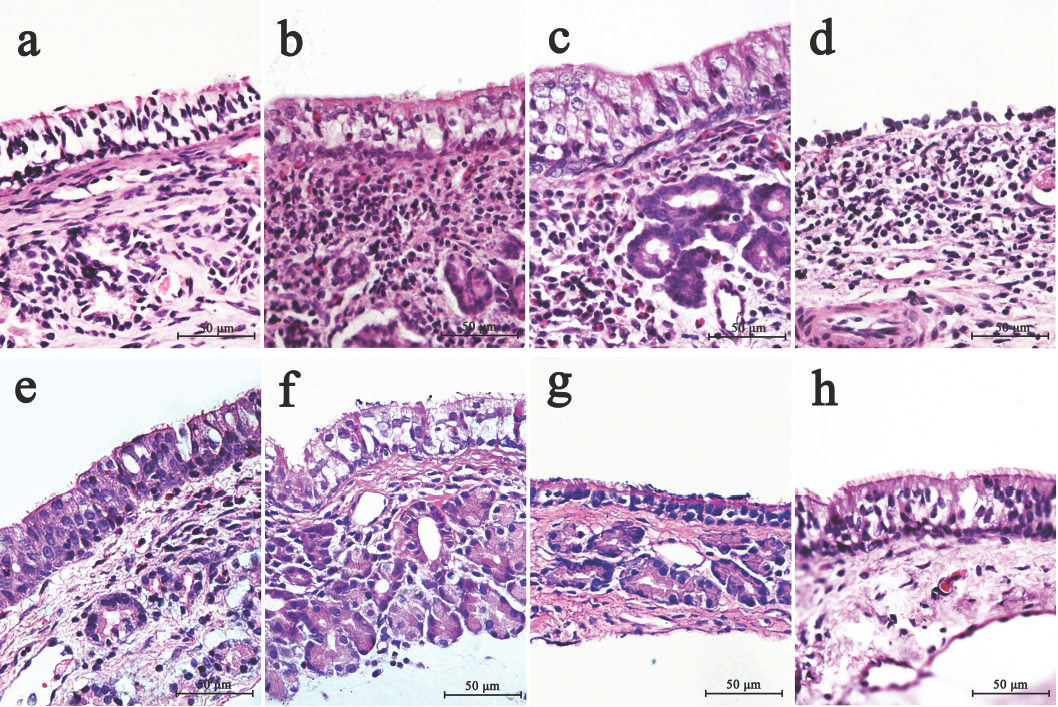
Hematoxylin and eosin (H&E) staining of rabbit maxillary sinus mucosa. (a–d) Images of model groups after inoculated with Staphylococcus aureus at (a) 1 week, (b) 2 weeks, (c) 4 weeks, and (d) 8 weeks. (e and f) Images of negative control groups after Gelfoam placement at (e) 1 week, (f) 2 weeks, (g) 4 weeks, and (h) 8 weeks (400x magnification).
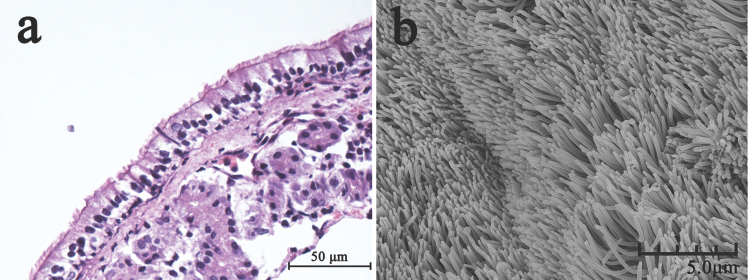
Hematoxylin and eosin (H&E) staining and scanning electron microscopy (SEM) image of normal rabbit maxillary sinus mucosa. (a) H&E staining shows normal mucosa with columnar ciliated epithelium, with no significant inflammatory cells in the subepithelial layer (400x magnification). (b) SEM image shows normal mucosa with intact cilia (5000x magnification).
SEM clearly showed the characteristic changes of the mucosal surface, and the results showed that biofilms presented in 100% of rabbits, which was infected with bacteria for ≥2 weeks. At 1-week postinoculation, SEM showed that the cilia were covered by a large amount of mucus-like substance, and lots of scattered bacteria can be seen on the mucus blanket, with no obvious bacterial biofilm (Fig. 4 a). At 2 weeks postsurgery, the main feature of the mucosa is that the cilia were divided into pieces and encapsulated by pod-like structures, which appeared to be composed of multiple smaller organisms that presented with extracellular glycocalyx (Fig. 4 b). At 4 weeks postsurgery, the bunchy cilia disappeared, and only some spheroidal structures of encapsulated cilia remained, and clusters of organisms attached to the infected mucosa, which had characteristic morphological features of biofilms, such as water channels, three-dimensional structure, and matrix-embedded spherical bodies (Fig. 4 c). At 8 weeks postsurgery, a large number of epithelial cells disintegrated with large areas of epithelial shedding that appeared, but the biofilms were also visible without any dramatic changes (Fig. 4 d); however, for the negative control groups, the integrity of the epithelium was always presented, without evidence of bacterial biofilm. The morphological changes of mucosal surfaces were mainly characterized as shorter and sparser cilia at 1-week postsurgery (Fig. 4 e), and with local scaling at 2 weeks (Fig. 4 f). These changes were only observed at 1 and 2 weeks after Gelfoam placement. As for the 4- and 8-week groups, the cilia recovered to normal (Fig. 4, g and h) and the mucosa surfaces were similar to the blank control group, which was characterized as normal mucosa with intact cilia (Fig. 3 b).
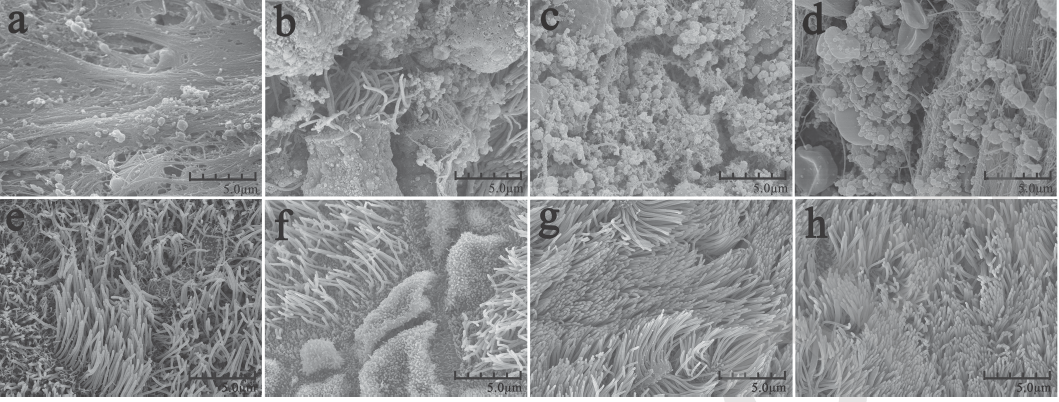
Scanning electron microscopy (SEM) images of rabbit maxillary sinus mucosa. (a–d) Model groups after inoculated with Staphylococcus aureus at (a) 1 week, (b) 2 weeks, (c) 4 weeks, and (d) 8 weeks. (e–f) Negative control groups after Gelfoam placement at (e) 1 week, (f) 2 weeks, (g) 4 weeks, and (h) 8 weeks (5000x magnification).
Discussion
In this study, we used SEM and H&E staining to identify the bacteria biofilms and histological changes of nasal mucosa after S. aureus inoculation. SEM is a generally accepted method for identifying biofilms that can clearly show the presence of biofilm on mucosa. Recently, researchers have found that H&E staining is also a reliable method for the detection of bacterial biofilm.24,25
In our study, SEM showed that biofilms presented in 100% of rabbits which were inoculated with bacteria for ≥2 weeks; however, for the rabbits without bacterial inoculation, although they underwent maxillotomy and Gelfoam placement, no bacterial biofilm had been found at any time point after the modeling surgery. This suggested that bacterial inoculation is essential for forming biofilms in the sinus.
Meanwhile, H&E results of the model groups showed a strong correlation with those of the SEM. At different time points, however, the morphology of biofilms, the severity of epithelial cells, and cilia injury were different. At 1-week postsurgery, the pathological changes of the nasal mucosa were mainly presented as submucosal gland hypertrophy and goblet cell hyperplasia. Consistently, SEM showed the epithelial layer covered by mucus-like substance with lots of scattered bacteria. These results suggest that the mucociliary system and inflammatory secretions might prevent initial bacterial attachment to some extent. For the 2-week group, the pathological changes mainly appeared as abundant inflammatory cells infiltrated in the subepithelial layer, including lymphocytes and plasma cells, which were considered to be the most important predictors of biofilm presence. 25 Accordingly, SEM showed bacteria attached to the cilia and formed biofilms, and some cilia wrapped and showed loss of activity. These phenomena may be reflected by the early stage of biofilm formation on the nasal mucosa. At 4 weeks, SEM revealed that a large amount of bacterial biofilms attached to the epithelial surface with no normal cilia structure. These results were consistent with the results of H&E staining, in which the swollen epithelial cells appeared necrosis and disintegrated. All of these changes still existed at 8 weeks, suggesting a stable phase of the disease.
A large number of eosinophils were also found infiltrated in the mucosa with biofilms. However, this phenomenon was not observed in the negative control groups, indicating that it was not caused by the Gelfoam placement. This result is consistent with the discovery of Foreman et al., who found an association between S. aureus biofilms and an eosinophilic inflammation in CRS. 26
It is well known that ciliary beat defects can be associated with CRS. Our results clearly showed that biofilms formed by S. aureus can destroy the cilia. Conversely, the disarray and absence of mucociliary apparatus might facilitate biofilms development, which is a vicious cycle. Therefore, the protection of cilia may be the first step in blocking the attachment and aggregation of bacteria that would otherwise initiate biofilm formation. 27
This study also showed that rabbits might be the most suitable animal for the investigation of S. aureus biofilms in CRS. First, rabbits are relatively easy to operate on and can tolerate S. aureus inoculation well, as we showed in this study. Second, the relative volume and anatomic structure of the nasal cavity in rabbits resembles that of humans.28,29 At the same time, the maxillary sinus of rabbits connected with the nasal cavity by a narrow slit-like orifice, which is easily blocked and makes the former vulnerable to pathologies (Fig. 1 e). Furthermore, the large volume of rabbit maxillary sinus not only makes it easy to be accessed but also provides more samples for further testing (Fig. 1, e and f).
Compared with the existing models of biofilm-related sinusitis, our method is extremely simple and can easily be reproduced without special instruments or complex animal operations. This new model does not need complete obstruction of the ostium, which usually need to remove the anterolateral bone and mucosa of maxillary sinus or need to do complicated endoscopic sinus surgery to improve exposure of the sinus ostium. Our modeling surgery only resulted in an orifice on the anterolateral wall that has little effect on the maxillary sinus mucous. The gelatin sponge is selected because it can expand when absorbed bacterial suspension and thus partly or totally blocked the sinus ostium. At the same time, when the Gelfoam absorbed TSBg, it can be used not only as a culture medium to promote the overgrowth of pathogenic bacteria, but also as a foreign body to interfere with the ciliary activity, and the slower ciliary beat frequency may be conducive to bacterial attachment. 30 More importantly, accompanied by the absorption and liquefied degradation of the gelatin sponge, the ostium block improved; however, the ostium stenosis caused by mucosal swelling will still exist, which is quite similar to the mechanism of human sinusitis. In addition, the pathogen used in our study is a clinical isolate of S. aureus strains, which has strong virulence and biofilm-forming ability. Perhaps these characteristics are more conducive to biofilm formation and reflect the pathological changes caused by biofilms in humans.
In conclusion, this study provides a simple animal model of S. aureus biofilms in the rabbit maxillary sinus. This model has the advantages of simplicity and closely resembles human sinusitis. It is a potentially useful tool for the research of sinusitis, biofilms, and their treatment.
Footnotes
Acknowledgments
The authors thank Huayong Liu, Institute of Medical Microbiology and Institutes of Biomedical Sciences, Shanghai Medical College, Fudan University, for helping in bacteriological experiments; Yang Wang, Department of Human Anatomy, Histology and Embryology, Shanghai Medical College, Fudan University, for preparing paraffin-embedded maxillary sinus tissue sections and slides; and Hongyang Gao, Electron Microscopy Center, Shanghai Medical College, Fudan University, for helping in specimen preparation and photography.